Click Here to Download PDF Version

Telehealth Newsletter
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
| What is New?
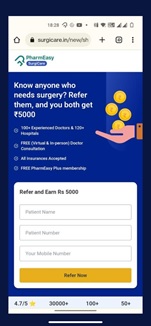
A few notable developments that occurred in 2022 are likely to be helpful and have a big impact on telehealth practice. The first was the National Task Force’s submission of Version 2 of Telemedicine Practice Guidelines to the National Medical Commission. And the second – the public debate over the Personal Data Protection Bill and its final submission this month. After this, the bill is likely to be submitted to the parliament for approval. The future course of telehealth will be set by these two significant developments. There has, however, been also another unsettling development, the expansion of surgical aggregators similar to those in the pharma feild. These aggregators are now offering commission for surgical referrals, which is very worrying trend (See the image). Corporate medicine in India has already resulted in ongoing ethical issues due to a practise known as referral kickbacks used by some of the country’s leading corporate hospitals and diagnostic centres, and now this – perhaps the mother of all kickbacks.
These kickbacks are against the laid ethical norms of NMC Professional Ethical Guidelines. TSI as a society can take a strong stand to condemn these practices before it catches fire and starts corrupting our ecosystem. As the festivities and the year come to a close, our newsletter team wishes all the TSI members a very happy, peaceful and safe 2023. Thank You |
 Uttarakhand Chapter of Telemedicine Society of India, inaugurated at AIIMS, Rishikesh
Uttarakhand Chapter of Telemedicine Society of India, inaugurated at AIIMS, Rishikesh
Dr. Murthy Remilla
Secretary TSI
Telemedicine is the new normal for affordable access to best-in-class universal healthcare in a connected and comprehensive healthcare ecosystem linking even the most remote rural populations to District, State, National and International Centres of Healthcare Excellence.
The Telemedicine Society of India (TSI) inaugurated the Uttarakhand State Chapter of the Telemedicine Society of India during a programme organised at AIIMS Rishikesh on December 10,2022. Professor (Dr) Meenu Singh, President (TSI) and Dr.Murthy Remilla, Hony. Secretary (TSI), jointly launched the Uttarakhand (UK) State chapter of the telemedicine society of India.
Dr.Meenu Singh, is currently the executive director of AIIMS Rishikesh, She highlighted the telemedicine option as a significant advantage for hill states with difficult topographical conditions, such as Uttarakhand and Himachal Pradesh. Dr Meenu Singh stated that additional medical and nursing institutions around the nation would soon be linked to this facility. The Base Hospital, Kotdwar and Lal Bahadur National Academy of Administration (LBSNAA) in Mussoorie are currently linked to AIIMS Rishikesh’s telemedicine capability.
TSI Hony.Secretary Dr. Murthy Remilla described the technology-based telemedicine facility as beneficial for strengthening health facilities across the country. He explained that, with a telemedicine facility, the effort is to strengthen health facilities in every village.
Vice president of TSI Uttarakhand, Professor Shalini Rajaram; Dean Academics, Prof Jaya Chaturvedi; Secretary of TSI Uttarakhand State Chapter and HOD of Urology Department AIIMS Rishikesh, Dr Ankur Mittal and Dr Rajan Arora from Govt of UK also addressed the gathering.
The event was attended by the Medical Superintendent, Prof Sanjeev Kumar Mittal; the Additional Medical Superintendent, Prof Anshuman Darbari; the Principal of the College of Nursing, Dr Smriti Arora; Professor of Physiology, Dr Poorvi Kulshrestha, Professor Arup Kumar Mandal; Dr Yogesh Bahurupi, PPS Vineet Kumar, and a host of others. Representatives of various institutions across the country also participated in the programme online.



 Digital Health Course Launched by IIM Raipur in collaboration with the Digital Health Academy
Digital Health Course Launched by IIM Raipur in collaboration with the Digital Health Academy
Dr. Rajendra Pratap Gupta
Programme Chair for the Post-Graduate Certificate Course in Digital Health
Why do we need a course in digital health
Broadly speaking using technology to deliver healthcare is Digital Health, and during COVID-19, all of us have used digital health in some form or the other. Healthcare is adopting technology faster than we can imagine. Online doctor appointments are now widespread, and using mobile apps for doctors’ consultations and management of chronic diseases is now a reality.
The software is now prescribed like a drug (SaaD), and software is now a medical device (SaMD); it is only that some have not used it while others have, and soon the number of people asking for digital therapeutics is going to increase. The age of treating patients with medicines alone is over, now, we would need technology for handling the new-age patient, and that’s why every doctor who is handling a patient will have to use digital health. The role of the doctor is becoming that of an infomediary. Technology is changing the relationship between the doctor and the patient.
The gap between what is happening and what is being taught is huge, and technology does not wait for anyone. Those who use digital health will replace those who don’t; hence, it is important to understand this digital health domain and be prepared so that when the opportunity knocks, people don’t miss it.
This course will help learners secure their organization’s future and medical practice. It will equip clinicians, paramedics, healthcare professionals, and managers to understand the digital health domain and the deployment of digital health tools. Also, now ABDM is incentivizing the adoption of electronic health records, every single provider will need people qualified in digital health to serve the patients under various government schemes and through the use of ABHA number. Also, newer technologies like the metaverse will impact health care. So, such a course will be a basic enabler for existence in the healthcare sector.
Why is this course online ?
Given that working professionals and doctors find it difficult to attend a college or a university to learn about digital health, we created this fully online course with the world’s best faculty teaching digital health from their years of experience in digital health. Also, for digital health, the course should be delivered digitally.
What did it take to build this course ?
The course was developed with over two years of research with the world’s top authorities on Digital Health. The course was designed in consultation with over 60 global leaders across the healthcare domain working in hospitals, the pharmaceutical industry, research & development, med-tech, information technology, regulators, and policymakers spread across the USA, U.K., E.U., South-East Asia, Africa, and after research in over 100 countries on the course’s need and content. The course is a unique blend of the world’s best faculty and use-cases in digital health.
This is the world’s first ‘Certified Digital Health Professional’ (CDHP) course blending the fields of health, technology, and management. The CDHP course has three levels; Basic, Advanced and Professional. This course aims to provide knowledge on theoretical, technological, management, and application aspects of digital health across the continuum of care. The faculty of CDHP™ are the actual practitioners of Digital Health & Management. They are global health technology leaders who have developed and delivered Digital Health. After this course, people will understand the digital health domain and how to deploy digital tools in day-to-day practice and gain a competitive advantage. The learners will get a theoretical, technological, management, and application-level understanding of key digital health tools.
What is the career perspective for those taking this course?
This Post Graduate Certificate Course in the field of Digital health offers people an opportunity to be a formally qualified and trained professional in digital health. This course can help build a career in:
- Pharmaceutical Industry
- Hospitals
- Consulting & Advisory services
- Chronic Disease Management
- Medical Devices
- Information Technology
- Academics & Research
- Digitalizing Medical/ Clinical Practice
- Public Policy & Regulation
- Digital Health Project Management
- Marketing & Business Development for Organizations in Digital Health
- Develop Digital Health Solutions
- Insurance
- Entrepreneurs in Digital Health
Who will award the certificate for this course?
The course certificate will be awarded by IIM Raipur & Digital Health Academy, and those successfully completing the course will become the executive alumni of IIM Raipur. Also, the Digital Health Academy will list the learners in the Certified Digital Health Professionals directory.
What is the international recognition for this course?
The course is endorsed by two of the most prominent bodies in Digital Health; International Society for Telemedicine & eHealth , Switzerland, and the European Connected Health Alliance
What are the eligibility criteria for enrolling in this course?
Graduation degree or its equivalent with work experience of minimum of two years . Clinicians and healthcare professionals, and managers can apply.
How many seats are being offered;
200 seats are available for the 2023 cohort.
What is the Fee structure?
For Indian Students: INR 3.6 Lacs plus applicable taxes
For Foreign Students: US$ 7,000
*The above fees include tuition Fees, Material / Notes & Alumni fees.
3 day Contact Program (Optional) at IIM Raipur.
Website for the course : https://web.iimraipur.edu.in/index.php/programmes/pgcpdh/pgcpdh-overview
NHA aims to promote adoption of Ayushman Bharat Digital Mission (ABDM) by offering incentives of up to Rs. 4 crores to hospitals, labs and digital health solution providers
The National Health Authority (NHA) has announced a Digital Health Incentive Scheme (DHIS) for the stakeholders of the digital health ecosystem. The scheme aims to give a further boost to digital health transactions in the country under the Ayushman Bharat Digital Mission (ABDM). The incentives under this scheme would be provided to hospitals and diagnostic labs and also to the providers of digital health solutions such as Hospital/ Health Management Information System (HMIS) and Laboratory Management Information System (LMIS).
Under the DHIS, the eligible health facilities and digital solutions companies shall be able to earn financial incentives of up to Rs. 4 crores based on the number of digital health records they create and link to ABHA (Ayushman Bharat Health Account). This incentive can be availed by the health facilities (hospitals and diagnostic labs) registered with ABDM’s Health Facility Registry (HFR) and fulfilling the eligibility criterion specified under the scheme.
Elaborating on the same, Dr. R. S. Sharma, CEO, NHA said – “We believe that this scheme will encourage more and more healthcare facilities and digital software companies to come forward and join ABDM for providing patient-centric healthcare. Through this financial incentive scheme, we’re encouraging the adoption of digital health. Further, we’re also including solution (HMIS/ LMIS) providers in the incentive scheme so that they handhold other health facilities to come on board and facilitate strengthening of the ecosystem. Incentives have played a catalytic role in driving early adoption of other citizen centric programs such as UPI, notification of TB cases, Janani Suraksha Yojana, etc.”
Important points under ABDM’s Digital Health Incentive Scheme are:
1.Incentives would be provided to the following entities:
a. Health Facilities having 10 or more beds
b. Laboratory/radiology diagnostics centres
c. Digital Solution Companies (entities providing ABDM enabled digital solutions)
2.The incentives shall be provided on the basis of the number of ABHA-linked transactions i.e. the digital health records created and linked to ABHA.
| Healthcare Facility | Base Level Criteria | Incentives |
| Hospitals | 50 Transactions per bed per month | Rs. 20 per additional transaction above the base level |
| Diagnostic facilities /Labs | 500 Transactions per month | Rs. 15 per additional transaction above the base level |
3.Digital Solution Companies (DSCs) will be given an incentive of 25% of the incentive amount received by the eligible health facilities using their digital solutions.
4.For the ABHA linked transactions done by facilities not eligible for direct incentives (Clinics/ Small Hospitals/ Health Lockers/ Teleconsultation Platforms etc.), an incentive would be provided to Digital Solution Companies.
| Cost Incentives for Digital solution (HMIS and LMIS) Companies | |
| For every Transaction by hospitals/labs using their software and receiving incentives under this policy | 25% of the corresponding incentive amount received by the eligible facilities |
| For other Transactions (including by health lockers, Teleconsultation platforms, small clinics etc.), provided the transactions are more than 200 per month | Rs. 5 per Transaction |
For public sector facilities, the incentives shall be added to the funds under Rogi Kalyan Samiti. The estimated initial financial outlay of the incentive scheme is Rs. 50 crores for a period of six months starting from 1st January 2023 onwards.
Further, public webinars would be organised by NHA starting from Dec 23, 2022 to provide detailed overview of the scheme. The schedule and link for the webinars will be available on the website https://abdm.gov.in/dhis. Full text of DHIS is available at: https://abdm.gov.in:8081/uploads/Digital_Health_Incentive_Scheme_550e710e09.pdf …Read More
Announcement
10th International Conference on Transforming Healthcare Using IT from 13th to 14th February 2023 at New Delhi

Telemedicine – News from India & Abroad
Google to Soon Translate Doctor’s Handwritten Prescription
Google to use artificial intelligence (AI) and machine learning (ML) model to identify and highlight medicines within difficult-to-read handwritten prescriptions.This will act as an assistive technology for digitizinghandwritten medical documents by augmenting the humans in the loop such as …Readmore
Artificial Intelligence may Predict Success of Botox Treatment in Dystonia Patients
With the help of artificial intelligence/AI technology, researchers have designed synthetic DNA that controls the cells’ protein production.How our genes are expressed is a process that is fundamental to the functionality of cells in all living organisms. Simply put, the genetic code in DNA is transcribed ….Readmore
Is Artificial Intelligence Better at Predicting Brain Metastasis Outcomes
An innovative artificial intelligence (AI) technique developed is found to be more effective than the human eye when it comes to predicting therapy outcomes in patients with brain metastases.The new research and technology could eventually lead to more tailored treatment plans and better health …Readmore
Virtual Reality Game Detects Attention Deficit Hyperactivity Disorder
Virtual reality games and machine learning approach were used by researchers to detect attention deficit hyperactivity disorder (ADHD).ADHD is a common attention disorder that affects around six percent of the world’s children. Despite decades of searching for objective markers, ADHD diagnosis ….Readmore
Looking towards the future of telehealth in Medicare, evidence is needed
Throughout the COVID-19 pandemic, telehealth services have played an essential role in maintaining and expanding Americans’ access to their health care. But what comes next to ensure that telehealth can work after the pandemic? What can we learn from those with “hands-on” experience with telehealth from the past two years? https://www.whitehouse.gov/ostp/news-updates/2022/11/10/looking-towards-the-future-of-telehealth-in-medicare-evidence-is-needed/
Click here to Become a Member of Telemedicine Society of India
Telemedicine Practice Guidelines – A Foundation Course for RMPs by TSI Faculty
To know more about the Telemedicine Foundation Course click on the link below:
https://tsitn.org/tpg-course/
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TN TSI Newsletter-
|
Submission may be sent to – tsigrouptn@gmail.com
Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff
Editors – Dr. Senthil Tamilarasan & Dr. Sheila John
Technical Partner- https://www.medindia.net






 Special Note About the Digital Personal Data Protection Bill, 2022
Special Note About the Digital Personal Data Protection Bill, 2022












 Digital India Act and Pending Legislations
Digital India Act and Pending Legislations TSI Mid-Term Conference – Proceeding and Recommendation Thereof
TSI Mid-Term Conference – Proceeding and Recommendation Thereof



 TELE ICU – Challenges and Solutions
TELE ICU – Challenges and Solutions


 Teleconsultations between doctors
Teleconsultations between doctors Necessity for formally dually trained Clinician Scientists and Clinician Technologists
Necessity for formally dually trained Clinician Scientists and Clinician Technologists

 Mobile Teladoc Health Robots at MMHRC
Mobile Teladoc Health Robots at MMHRC









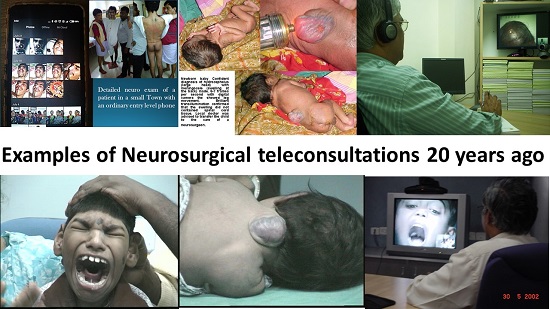
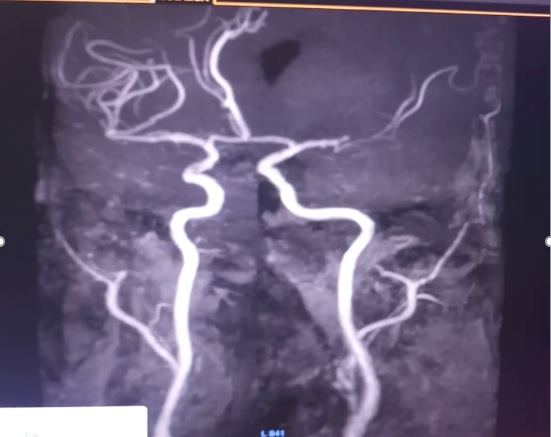
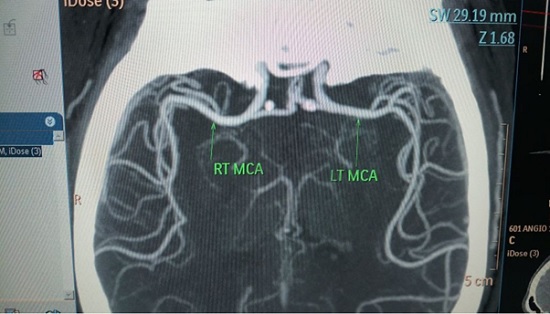
 Role of Telemedicine in Stroke
Role of Telemedicine in Stroke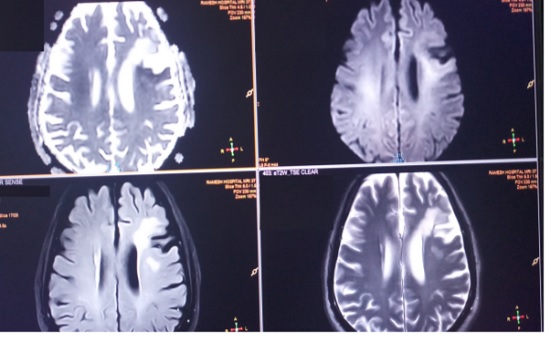
 Tele-Neurorehabilitation: A story from Mumbai
Tele-Neurorehabilitation: A story from Mumbai
 Understanding the implementation of telepractice in speech and language services for children and adults using a mixed-methods approach
Understanding the implementation of telepractice in speech and language services for children and adults using a mixed-methods approach

 Decoding the Healthcare Professional Registry’s Utility in Telemedicine
Decoding the Healthcare Professional Registry’s Utility in Telemedicine TELEMEDICINE IN INDIA: A CRITICAL ANALYSIS OF THE EXISTING LEGAL FRAMEWORK – A Summary
TELEMEDICINE IN INDIA: A CRITICAL ANALYSIS OF THE EXISTING LEGAL FRAMEWORK – A Summary
 Prescriptions and Digital Signatures
Prescriptions and Digital Signatures