Click Here to Download PDF Version

Telehealth Newsletter
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
| What is New?
Since its inception during the COVID period, the e-sanjeevani app has performed 100 million teleconsultations, the prime minister revealed in his Mann Ki Baat programme. This is unquestionably a world record for the most free teleconsultations ever conducted. We’ll wait for a publication to learn more about its accomplishments and difficulties. The clinicians may learn a lot and contribute to the ecosystem’s general expansion. TN-TSI chapter and KCG College of Technology successfully hosted a CME on telemedicine for engineering students this month. The programme was warmly accepted, and we intend to run more programs in the future. One of our members displayed the mobile lab that provides lab results instantly. The recent decision from the Gujarat High Court regarding e-pharmacies is covered by our legal expert Bagmisikha. Even though there is uncertainty regarding their legality, e-pharmacies have expanded. There are unlikely to be any quick fixes to resolve issues related to their status. We are getting ready for the next TELEMEDICON in Goa. Registration is open so do register. Thank You |
 Faculty Empowerment Program on Telemedicine and Health Care Research
Faculty Empowerment Program on Telemedicine and Health Care Research
Dr. Thulasi Bai
Professor, KCG College of Technology
Faculty Empowerment Program (FEP) on Telemedicine and Health Care Research was organised by KCG College of Technology in association with Telemedicine society of India-TN Chapter (TSI-TN) on 18th February 2023 at Mirza Seminar Theatre. Dr.Thulasi Bai, Professor, Department of ECE coordinated the over all program.
The inauguration started with prayer song at 9.15 AM. The workshop was inaugurated through traditional lighting of Kuthuvillakku by the dignitaries of TSI-TN and KCG College of Technology. Dr. Kavitha Balamurugan, Head, ECE department welcomed the gathering. Dr. Sunil Shroff, Senior Consultant – Urologist, Madras Medical Mission and President – TSI, TN Chapter gave the presidential address. In his speech, he explained the importance of Telemedicine.
Dr. T. Senthil CEO, Welcare Health Systems, Honorary Secretary, TSI-TN briefed about the activities of the TSI-TN and telemedicine in general. Dr. Srinath Yeswanth, Co-Founder, Curehealth Systems, LLP explained his experience with Telemedicine. Dr. Sheila John, Head of Teleophthalmology & E-Learning, Sankara Nethralaya, TSI-TN talked various initiatives taken in the hospital for screening the patients in rural areas through telemedicine.
After the inauguration the following speakers delivered their speech to assure the participants the best experience about the Telemedicine.
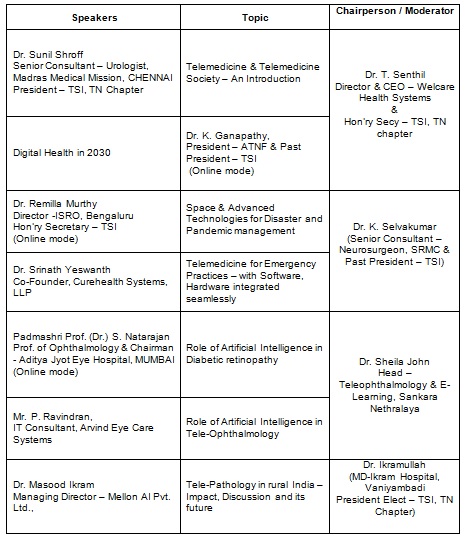
The Faculty Empowerment Program was attended by around 150 participants (Students and faculty) which includes external participants, Faculty of Electronics and Communication Engineering, Students of ECE, IT, AI&DS and Mechatronics department. Tele-Pathology van was brought to the campus and the participants had a chance to explore the facilities which was the highlight of the program.
The participants were given certificates and the FEP received good feedback from them. The workshop came to an end by 2.30 PM.
The organising team thank Management of KCG college of Technology and Principal for hosting the FEP and TSI-TN for arranging the eminent speakers for the sessions.

|
|
|



|
|
|


 DCGI issues notice to e-pharmacies for online sale of drugs without a license
DCGI issues notice to e-pharmacies for online sale of drugs without a license
Bagmisikha Puhan
Associate Partner, TMT Law Practice
Siddhant Gupta
Associate, TMT Law Practice
The Drug Controller General of India served show cause notices to prominent e – pharmacies earlier this month, for their continued violation of the provisions of the Drugs and Cosmetics Act, 1940 (DC Act). The show cause notice has relied upon the 2018 order of the Hon’ble High Court of Delhi in the matter of Dr. Zaheer Ahmed v. Union of India and Ors., whereby e-pharmacies were injuncted from the online sale of medicines without a due and proper license and were directed to ensure that the same is prohibited forthwith. The DCGI’ action is driven by the complaint forwarded by the All-India Organization of Chemists and Druggists (AIOCD) to multiple government agencies, including the Prime Minister’s Office (PMO), citing blatant abuse and violation of applicable law, and a rise in spurious drugs distribution.
It is interesting to note that while DCGI had forwarded the captioned order for compliance and action by the state drug controllers in 2019, there were no similar actions contemplated in the last 3 years, during the COVID-19 pandemic. E – pharmacies were instrumental in the past years for last mile healthcare delivery, where a considerable size of the demographics was stationed at home and accessibility to efficient and reliable healthcare services was a challenge. In fact, on March 26, 2020, during the lockdown, the Central Government realized that the retail sale of drugs to the doorstep of consumers is essential to meet the requirements of emergency arising out of pandemic COVID-19 and in the public interest, and accordingly notified the prescriptions for regulation of sale and distribution of drugs for their delivery to the consumers.
In addition to the same, the Telemedicine Practice Medicines, 2020 had sought to regularize and regulate the practice of telemedicine and provided nominal guidance to RMPs for their online consultation conduct and provided for necessary compliances to safeguard patient interest. This also provisioned for what happens when the RMP needs to communicate the prescription to a pharmacy, this was also provided within the same. It did seem like there was not just a mere acceptance of this position, but also growing awareness of consumer comfort which was being sought to be achieved by way of this arrangement between online pharmacies, and end users.
With an objective to regulate this market proposition, the amendments which were proposed to the existing regulatory framework by way of introduction of the draft Drugs, Medical Devices and Cosmetics Bill, 2022, which further indicated towards issuance of specific licensing guidelines for e-pharmacies to regulate the online sale of drugs and cosmetics. Furthermore, the draft National Medical Commission Registered Medical Practitioner (Professional Conduct) Regulations, 2022 sought to provide extensive guidance on the online conduct of RMPs, thereby reiterating the government’s intention to rely on digital technology to promote medical accessibility.
Indeed, the Ayushman Bharat Digital Mission (ABDM), the brainchild of the NITI Aayog and Ministry of Health and Family Welfare, further seeks to provide for a federated health information architecture, which will seek to further interoperability, accessibility and portability of health records across public and private healthcare institutions.
The DCGI action could set the Indian pharmaceutical industry on the backfoot again, after spirited efforts have been made by the regulators and industry stakeholders alike, to realign their operations to incorporate a digital component, and provide healthcare services to patients who are bed-ridden, or reliant upon their caregivers, in terms of finding access to the most primitive modes of care delivery. Adoption of technology, specifically the internet, allows for the ecosystem to increase accessibility and affordability of the services which are presented to the end users, bringing healthcare delivery to the last mile. We must afford e-pharmacies similar leeway, and provide them with the necessary guidance and regulation to streamline their operations, and allow the demographic to leverage the countless advantages of such service providers.
What appears to be a disconnect is the fact that the online pharmacies did not necessarily always rely on the large brick-and-mortar pharmacy chains which exist, but turned towards their own warehouses, stores in bringing this service to the last mile. The representation which made its way to the top, seems to be motivated by the lack of opportunities for the existing set-ups, where digital consultation, has paved way for the end users to find consultation, health check-up and drugs/ medicines, all at one point of care on the internet, as opposed to having to visit a doctor in a facility, and then going to another place for seeking their prescription drugs.
A show cause notice seeking information could be the starting point for regulation, however, this should not be considered to be an opportunity to undo the entire online ecosystem which has been created for the benefit of the masses.
 Satellite to Block Chain – A new paradigm in Covid care delivery through Telemedicine under India’s Health care Mission “Ayushman Bharat“
Satellite to Block Chain – A new paradigm in Covid care delivery through Telemedicine under India’s Health care Mission “Ayushman Bharat“
Satyamurthy Lakkavalli and Bhagwant Singh Ratta
Suquino Telehealth India
Introduction
“Ayushman Bharat” meaning blessings of longevity for Indians, is a national flagship mission which is a federally funded government health care delivery system launched in the year 2018. It is an umbrella of two major healthcare initiatives namely:
National Health protection scheme (NHPS): This scheme is envisaged to be applicable for over 100 million poor and vulnerable families for providing up to $ 7,000 (USD) per family annually for secondary and tertiary care hospitalization. Benefits of the scheme are portable across the country with cashless benefits from any public or private empanelled hospitals across the country.
Health and Wellness centres (HWC): Under this scheme a whopping $170 million (USD) is allocated for establishment of 1,50,000 HWCs centres to provide comprehensive health care, covering non-communicable diseases and maternal/child healthcare services at primary level.
Ayushman Bharath and Telehealth:
The Telemedicine Program conceptualization, formulation and implementation in India was primarily spearheaded by the Indian Space Research Organization (ISRO) in the year 2001 under Space Technology applications for societal benefits. ISRO marshalled the diverse stakeholders across the country namely the Doctors, Specialist Hospitals, State Governments, Health Administrators, Technologists and Industry into a common platform for ushering Telemedicine service for rural, semi-rural and urban population.
The important factor of providing satellite connectivity without any charge by ISRO was the major boon for many of the rural district and specialty hospitals.
During the period 2002-2010 India had one of the largest Satcom based Telemedicine network by ISRO with 400 Remote/ rural/ district hospitals and 200 Village resource centres in most of 25 States of the country connected to 50 Specialty hospitals/Medical college hospital located in major cities/towns in the country including 20 Mobile units covering the various medical specialties.
More than Million Teleconsultation took place with several lifesaving instances during that period.
This commendable effort by ISRO demonstrated a beneficial change in reaching out to the rural population of India culminating in a federal government recognizing Telemedicine as an important application under National Health Mission (NHM)of the country.
Ayushman Bharat Digital Mission (ABDM)
ABDM scheme launched in 2018 got a fillip to stitch the silos in Indian health care system. Blockchain technology was thought of since it has the potential to revamp the currently existing processes to unlock new sources of efficiency and value, as was seen and evidenced in the pharmaceutical supply chain, verification and approval of fertiliser subsidies, verification of university certificates and transfer of land records in the country.
The ABDM envisages to register every next provider of healthcare in the country on the portal as the first vertical with all the healthcare facilities in government/ private sector including corporate hospitals and diagnostic Labs registered as second vertical. The third vertical being the population registry with every citizen having healthcare ID called ABHA no (Ayushman Bharat Health Account). The last being the software, hardware, medical devices, health IT companies being registered to provide the service for primary care through Wellness clinics and secondary/tertiary care through hospitals across the nation. With the advent of IT solutions like IoT-driven (Internet of Things) intelligent medical devices, personal healthcare apps for Telemedicine, AI for clinical decision making, online pharmacies for convenience and price comparisons, to name a few, have helped fuel the growth of Indian healthcare.
Creating a unique EMR under ABDM
One of the potential solutions that is often missing from the discussion is a portable or intra-operational Electronic Medical Record (EMR). In India, EMRs are primarily a platform to generate billing for the patient as there is low penetration of package pricing (an agreed-to and published price for a defined procedure) and thus most patients pay a-la-carte for the services they consume (doctor’s time, drugs, radiology reports, procedure, etc.). In this scenario there are no incentives to contain costs or stop unnecessary services from being performed and/or billed, as hospitals generate revenues by providing additional diagnostic tests which may not always be clinically appropriate. In addition to the billing aspect of an EMR, an EMR should also provide an electronically formatted patient file which provides a medical history and ensuing patient notes which are written by the doctor, nurse or allied health professional, results of lab tests and radiology imaging reports, as well as pharmacy orders.
It is not just in India, but in high income economies like the U.S, most of the EMRs cannot easily transfer data from one hospital to another. Why this is important, especially for poorer patients availing services as part of the Ayshman Bharath scheme? Many of these targeted patients need to travel for life saving care from rural India to a Tier I or Tier II city for surgery and rehabilitation, yet their private health information does not easily travel with them in an organized manner that would ensure timely and smooth transition for admission at a surgery centre and subsequently the post-surgery follow-up phase.
Block chain and EMR
Blockchain technology adopted has the potential to facilitate a national EMR system and provide the backbone for building a robust and centralized EMR system. Uploading and storing EMR data on a blockchain application could ensure that all stakeholders would benefit from EMR data without disturbing the integrity of the data and the privacy of confidential patient information. A blockchain EMR could store patient data and provide a unique file identification number to each patient, akin to an Indian Aadhar card number (UID) or U.S. Social Security card number, but the file can only be unlocked by a confidential code that is generated by the EMR blockchain system and the access code is known only to the patient. Additionally, since blockchain is a peer-to-peer technology, all users have a copy of the data in the database and unauthorized changes to the data can be flagged and deleted automatically in each user’s database, thus further ensuring data integrity.
Some of the benefits of using a blockchain EMR system could include:
- Continuum of care resulting in better outcomes
- Tax payers and Government could track the successful service for greater transparency and understanding as to how services are being utilized and paid for.
- Insurance companies/trusts could more easily identify payment fraud and automatically disburse payments directly to a hospital’s bank account which is also one of the Government’s objectives (cashless, pre-authorized payment for services rendered)
Block chain adopted for Covid care
Covid brought unprecedented challenges in every walk of life due to which a big shift taking place in the healthcare industry. Government of India responded well by bringing in The Telemedicine Practice Guidelines on the very next day of the National lockdown on 25th March 2020. This opened the Pandora’s box for teleconsultations on Government and private platforms.
With the success of Blockchain technology in various Government sponsored program in India such as Aadhar, the world’s largest unified ID based system (1.2 billion biometrics and as more than 25 million authentications per day) and others like Unified Payments Interface (UPI) 1.3 billion transactions in Dec 2019, e Sign, Digi locker, Goods and Services Tax Network; Ayushman Bharat Digital Health mission (ABDM) with ABHA app, unified health interface and sandbox integration using block chain technology permits online search of health services, teleconsultations, diagnostic tests etc for creation of longitudinal health record . This enables connecting the different silos in the healthcare system and giving equitable and ubiquitous access to healthcare there by drastically reduce out of pocket expenses for the beneficiaries.
Conclusion
ABDM has already taken off and about 240 million e Cards have been issued to beneficiaries with approximate 8 million hospital admissions. It is envisaged that more than 80 per cent of India’s 1.35 billion population will be in the ABHA registry in the foreseeable future. 144787 healthcare facilities have already been registered. ABDM has built in security at different stages to prevent fraud in any chain. This enormous effort of integrating all the stake holders is enormous job by the federal government and hope for a successful fruition of this mega programme benefiting the major population of India in the near future.
Bibliography:
National Health Authority of India
Ministry of Health and Family Welfare, Govt of India
Ministry of Electronics and Information Technology, Govt of India
Digital India
The National Portal of India
Centre for Development of Advanced Computing, Govt of India
Disclaimer: The complete work related to Ayushman Bharath, Covid care and adaptation of block chain is being carried out by the different Ministries and Departments of Govt of India under the advice of NITI Aayog, the Think tank of the Indian Government. The authors have only done the research study from the data available and do not claim any credit or responsibility on the success of this mega project.
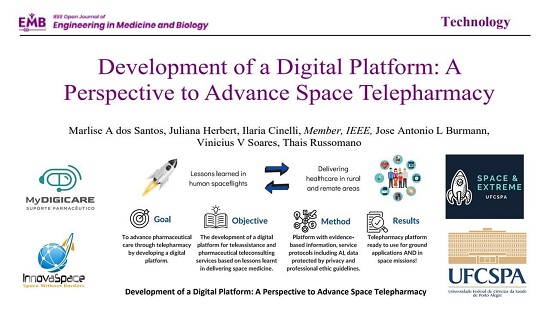
Development of a Digital Platform: A Perspective To Advance Space Telepharmacy
Marlise A dos Santos, Juliana Herbert, Ilaria Cinelli, Jose Antonio L Burmann, Vinicius V Soares, Thais Russomano
Abstract:
Goal : Lessons learned from decades of human spaceflight have helped advance the delivery of healthcare in rural and remote areas of the globe. Inclusion of the public in spaceflights is not yet accompanied by technology capable of monitoring their physical and mental health, managing clinical conditions, and rapidly identifying medical emergencies. Tele-pharmacy is a practice prioritizing pharmaco-therapeutic guidance and monitoring to help improve patient quality of life, and can potentially expand the field of space medicine. We seek to advance pharmaceutical care through tele-pharmacy by developing a digital platform.
Objective: This study focuses on the development of a digital platform for tele-assistance and pharmaceutical teleconsulting services that builds on lessons learned in delivering space medicine.
Methods: The platform contains evidence-based information on various drugs grouped by medical specialty, and also records and saves patient appointments. It has specific service protocols for service standardization, including artificial intelligence, to allow agility in services and escalation. All data is protected by privacy and professional ethics guidelines.
Results: The tele-pharmacy platform is ready and currently undergoing testing for ground applications through validation studies in hospitals or medical clinics.
Conclusions: Although developed for use on Earth, this tele-pharmacy platform provides a good example of how terrestrial healthcare knowledge and technology can be transferred to space missions. Read More
Telemedicine – News from India & Abroad
Transforming India’s Healthcare: Digitize Health Records
The gap between healthcare delivery and digitization is narrowing daily. Global health systems have continued to evolve, especially in the area of information technology (IT) penetration. In India, where 1.6 million people die due to poor quality health care, more stakeholders in the health sector are increasingly searching for solutions to address quality . …Readmore
Can Artificial Intelligence Detect COVID-19 by Listening to Cough Sounds?
Cough sounds do not help Artificial Intelligence (AI) technology to predict COVID-19 better, reports a new study.The AI classifiers trained on audio recordings cannot accurately predict whether someone has COVID-19 by analyzing the sound of their coughs, according to the study led by the UK’s Alan Turing Institute…..Readmore
Life-saver: Apple Watch Saves Wearer’s Life From Fatal Internal Bleeding
our watch can be a life-saver.Apple Watch saved the wearer’s life, by alerting him about a racing pulse following a nap, which led to a diagnosis of severe internal bleeding. Apple Watch can Now Detect Heart Blockage in Real Time Can Apple Watch detect heart problems? Yes, an Apple watch can now help in detecting undiagnosed heart blockage. …Readmore
Can Robots Help Children with Learning Disabilities Stay Focused?
Social robots can assist children with learning disabilities, reports a new study.Engineering researchers at the University of Waterloo are successfully using a robot to help keep children with learning disabilities focused on their work. ….Readmore
Click here to Become a Member of Telemedicine Society of India
Telemedicine Practice Guidelines – A Foundation Course for RMPs by TSI Faculty
To know more about the Telemedicine Foundation Course click on the link below:
https://tsitn.org/tpg-course/
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TN TSI Newsletter-
|
Submission may be sent to – tsigrouptn@gmail.com
Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff
Editors – Dr. Senthil Tamilarasan & Dr. Sheila John
Technical Partner- https://www.medindia.net
