
Telehealth Newsletter
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter. |
 Message from Maj Gen (Retd.) A K Singh, President, TSI
Message from Maj Gen (Retd.) A K Singh, President, TSI
It gives me great pleasure and satisfaction that the Tamil Nadu Chapter of Telemedicine Society of India’s first Newsletter is being launched. Last three months have been very busy and productive. The training team led by Dr Sunil Shroff has done a commendable job of providing par excellent training to over 3500+ doctors. The Armed Forces Medical Services led by Lt Gen Madhuri Kanitkar had two sessions, in one the DGAFMS attended. That was the crowning glory of the TSI. The volunteering effort of the editorial team headed by Dr Shiela John is worth appreciating.
A short piece by our executive committee member Ms. Bagamishika Puhan about these training program also is enclosed.
I thank all members of the TSI in contributing to the growth of Telemedicine. The margadarshaks ( Past Presidents) have been a guiding force.
Jai Hind.
Maj Gen (Retd.) A K Singh
President, TSI
 Telemedicine in India: Personal Reminiscences from 1996
Telemedicine in India: Personal Reminiscences from 1996
K. Ganapathy M.Ch (Neurosurgery) FACS FICS FAMS Ph.D is a Past President of the Telemedicine Society of India, Former Secretary & Past President Neurological Society of India, Past President, Indian Society for Stereotactic & Functional Neurosurgery, Formerly Adjunct Professor IIT Madras & Anna University, Madras & Emeritus Professor Tamilnadu Dr MGR Medical University. He is on the Board of Directors of Apollo Telemedicine Networking Foundation & Apollo Tele Health Services.
“Excellence is not a destination – it is a never ending journey”
The beginnings
It all started on the night of Sep 16 1996, I had just finished delivering an institute lecture an IIT Kanpur. Just after the Q&A ended at 09:00PM, Prof. Srivathsan, HOD of Electrical Engineering Department insisted I have dinner with him. He introduced me to the word “Telemedicine” and persuaded me to prepare a project report from 11:00PM – 04:00AM. Then commenced a love affair, which over the next 24 years has taken its toll. My legally wedded wife is often relegated to No. 3. Initially, I was wedded to Neurosurgery and now it is Telehealth. Looking back the journey has always been exciting. Arduous, often frustrating,sniggers were common, comments included “Telemedicine Ha ha ha”- but that was the 20th century. In 1998, I even had the audacity to request the association of Rural Surgeons of India to embrace Telemedicine ( Fig 1). .Having started the first Stereotactic Radiosurgery unit in South Asia and as Secretary of the then 2200 strong Neurological Society of India, conventional wisdom dictated that I should continue to focus my skills and energy completely, on what I was trained for, namely neurosurgery .However deep down was a nagging feeling , “Was there not something else, which I could do, which could help more than a few thousand neurosurgical patients ” and then the story began . I took the road less travelled by and the rest – as they say is history !! In fact I embarked on making Geography History ! and distance meaningless.
The Aragonda Story
On March 24th 2000 Bill Clinton formally commissioned the world’s first VSAT enabled village hospital at Aragonda in Andhra Pradesh . In the first 2 years two hundred fifty echocardiograms were done there, telementored from Chennai by Dr Premshekar a pediatric cardiologist. Unfortunately we were all so inundated with clinical work that no papers were published, in what may have been a first of its kind initiative even globally. Every Tuesday morning, a tele–grand round took place with super specialists from the Department of Pediatrics at Apollo Hospitals, Chennai interacting with doctors in the village hospital.More than 200 tele grand rounds took place up to 2005. When Dr Vilvanathan Pediatrician who worked in this village hospital left it was not continued. Again this herculean effort was never documented.
Formation of ATNF
In 2001 Apollo Telemedicine Networking Foundation was formally established as a not for profit Section 25 company . Taking modern healthcare to remote areas using technology was the mission of ATNF . In between my neurosurgical commitments I spent time and effort to help a skeleton staff of four full time employees to achieve , what in 2001 appeared preposterous – remote consultation !! Every opportunity to put a then hardly existent Indian telemedicine on the world map was utilised. I took part in the first intercontinental live multipoint telemedicine symposium on June 19 2001. Bill Gates was also a speaker .Though today it looks juvenile, it was thrilling to talk to people across the globe from Chennai. I could not resist starting with “ Good morning, good afternoon, good evening and good night ladies and gentlemen!!” Then started teleconferences with, Japan, USA, Saudi Arabia, Hong Kong. 19 years ago for a hospital to embark on video conferencing to conduct clinical meetings was certainly not the norm. Over the next 20years more than 230 regional, national, and international videoconferences in different medical specialties have taken place.
2002
Feb 15 2002 was a red-letter day for the growth of Telemedicine in India. The tension which India went through when Chandraayan 2 was to land on the moon , was experienced by me and my team when we enabled the first VSAT teleconsultation to be witnessed by the Chairman of ISRO. ISRO has publicly acknowledged that their foray into Telemedicine was influenced by that demonstration. Such was my enthusiasm then, that the Vice Chancellor of Anna University even agreed to let me address principals of 600 engineering colleges of Tamilnadu to start telemedicine units. Needless to say only four responded and that too for a short time.Telemedicine for Armed Forces -It has been my privilege to have persuaded the Indian Army to set up telemedicine units in the southern and central commands as early as 2002 with the assistance of Lt Gen Anoop Jamwal who retired as Adjutant General. Unfortunately we were too far ahead of the time and the commissioned Telemedicine units became non functional . In 2017 Telemedicine in the Armed Forces was rte established.
2003
The first formal University accredited 4 week certificate course on Telehealth technology was started with Anna University. Over the next 3 years 150 candidates in 6 batches were trained. Unfortunately due to lack of employment opportunities the course was discontinued. At about this time the Ministry of External Affairs Govt of India produced a documentary India 2.0 where Apollo telemedicine was featured.Franchised Remote Telehealth Centres gradually increased in Tier II and Tier III cities mainly in North Eastern India . Port Blair, Andaman Islands and various other remote places followed. We had almost 30 centres then
2004-05
IIT Madras started working on telemedicine enabled indigenous peripheral medical devices, designed to transmit temperature, pulse rate, blood pressure, oxygen saturation, heart and lung sounds and a 12 lead ECG .We went to the villages, used kitchens in houses, got a 100 volunteers together and transmitted this clinical data to Apollo Main Hospital Chennai for doctors to evaluate. Several such testings and clinical feedbacks led to the birth of Remedi the first indigenous stand alone Telemedicine “ Black Box” . Due to a sickness at home I was unable to attend an international Critical Care Congress. Adversity was turned into Opportunity. I gave the talk from an ICU bedside . This had a great impact. Years later I had just landed in Chandigarh for the TSI annual conference. I was informed that my grand daughter was critical and admitted in the ICU at Bengaluru. I took the return flight. The next day I gave my scheduled talk on a mobile phone from the ICU. My younger colleague Aditi did a great job projecting the slides perfectly. This unscheduled virtual talk in 2008 was more effective than a normal talk.Telemedicine enabled Hospital on Wheels – In 2005 As part of the Distance Healthcare Advancement Project, along with Philips Medical Systems, ISRO, and the DHAN Foundation, a Hospital-on-Wheels (HoW) was made. The HoW would go to different villages and provide virtual teleconsults. Concentrating on the vehicle, its contents and satellite communication infrastructure. the low lying branches of trees and mud roads in villages was overlooked !! Subsequent VSAT receivers were made smaller and portable.Formation of TSI At the Telemedicine conference organized by ISRO at Bengaluru a few of us got together and decided to formalize the concept of TSI first mooted by Dr Saroj Mishra in 2001 at Lucknow. I became the first Treasurer ( and Joint Secretary) of TSI with the membership number of 001!!
2006- 2010
The next few years witnessed evangelisation of Telemedicine in India and overseas. Talks were given at Baghdad, Kosovo, Riyadh, USA and many other countries in the Middle East and Africa. Every opportunity was used to promote telemedicine. By this time, India has been placed on the world map in Telemedicine.Gradually VVIPs’ from other countries started to take notice of the work done here. The Prime Minister of Mauritius, the President of Nigeria and many, many other heads of states started visiting us to understand how we were making a difference. This resulted in setting up of telemedicine units in Lagos and Mauritius.Following visits from ministers from Uganda I received a “summons” from the First Lady of Uganda for a discussion to set up telemedicne units in Kampala. CII, FICCI and other organisations were pro actively contacted . Seminars, symposiums, workshops and conferences were conducted on a war footing throughout the length and breadth of India. Telemedicine became my second name. The audience were not convinced – ravings of another mad man ! . When The National Science Centre located at the National Science Museum New Delhi started a new gallery to showcase recent advances in science and technology a Telemedicine kiosk with facilities for live demos was set up. ATNF became a member of the Standards Committee on Telemedicine, the National Task Force on Telemedicine, the Working Group on Telemedicine of the Planning Commission, and the Working Group of the SARC Committee on Telemedicine.
International Conferences personally organised : In Nov 2007 the 3rd national conference of the TSI was held in conjunction with the 12th international conference of the International Society for Telemedicine and eHealth at Chennai. The conference was inaugurated by the Chief Minister of Tamilnadu. Over 300 Indian and 35 international delegates participated. In 2016 the ISfTeH conference was again held in Chennai along with the annual Conference of Transforming Health Care with IT Over 750 delegates participated. THCIT annual conference has been held regularly for the last decade.
mHealth – In August 2007 Ericsson requested me, to study for the first time in South Asia, the feasibility of remote clinical examinations through wireless connectivity. Special license was obtained to use 3G spectrum .We demonstrated that 12 lead ECG’s, blood pressure recordings, lung and heart sounds ,ultrasound studies and ECHO cardiograms could be transmitted wirelessly using 3G. For the trial demo availability of power for 10 hours in the outskirts of Madurai was organised. Backup generators with diesel for 4 hours as a standby was arranged. Due to an unexpected demise, staff of the Electricity Board left and there was no power !!. Getting additional diesel would take at least 4 hours. Diesel from two ambulances and a bus was removed and used. An example of how determination can solve any problem.This 3G trial was so successful that Ericcson requested us to showcase this in Bhutan and Bangla Desh. In July 2008 The Rockefeller Foundation organised a Making the eHealth Connection Conference at Bellagio Italy. I was invited for the 5 day brain storming session. The very term mHealth was conceptualised by mygroup.
Global telehealth initiatives of Govt of India – The Ministry of External Affairs, Govt. of India initiated the Pan Africa e-Network project for teleconsultations in 2009. ATNF was a major player in this project .Unfortunately the project was not sustainable. Again to advise the government on the Central Asia e-Network Project. I visited Uzbekistan, Kazakhstan and Turkmenistan and submitted a project report. This also did not materialise.Formation of ATHS . With increasing activities it was realised that we needed a full time CEO to head a regular company rather than a full time Neurosurgeon involved in Telemedicine as a passion . This suggestion was accepted and in October 2010 Apollo Telehealth Services was formed. An excellent team under the leadership of Vikram Thaploo has made use of the rich heritage. Being future ready the outstanding team have managed to operationalise what were originally concepts. My wish list is becoming real . It is also true that “ nothing can stop an idea whose time has come”. Today ATHS has one of the largest Call Centres and is the oldest and largest multi speciality Telemedicine Network in South Asia.
2011
eHome Visits Belonging to the BC era ( Before Computers, Before Christ & Before Covid are the same !!) I was keen on reviving house visits which were in vogue in the early seventies. Electronic house visits were initiated with a laptop/ dongle carrying attender connecting from the uninitiated patient’s home.Interestingly this simple innovation got the best poster award at the World Health summit at Washington in May 2011
2012
World’s largest number of Teleconsults from a HoW – In a first of its kind initiative, 527 patients in 13 different specialities were connected simultaneously to six tertiary Apollo hospitals, in different parts of India from a HoW at a mega health camp held at Ajmer in Northern India on 11th and 12th February 2012.Remote clinical evaluation was followed by ePrescriptions. Subsequently similar telecamps were held in different parts of Tamilnadu in southern India.
2014
Patient empowerment in rural India by promoting eHealth Literacy -Deploying multi point Videoconferencing, a knowledge empowerment programme, at the internet enabled Village Resource Centers of the MS Swaminathan Research Foundation, in rural Tamilnadu was started in 2014 . 115 talks have been given in Tamil so far attended on 25,000 occasions from 18 villages.
2015 ONWARDS
Virtual visits to ICU I-SEE-U® was a state of the art solution developed to enable virtual visits to ICU patients, from anywhere in the world, by authorised consultants, friends and relatives. The remotely enabled networked camera in the individual ICU cubicle can also focus on various monitors. The product got an award at an international conference at Singapore. Due to subsequent regulatory and privacy issues it was discontinued.
International Educational Activities : Columbia University , Wharton School of Business, the London School of Economics, Harvard Business school, Ross School of Business, Atlanta state University, Indian school of Business are some of the international organisations who have used Apollo Telemedicine as study material .Software An in house, custom built software “Medentegra” which in addition, to a user friendly EMR (facilitating uploading of images, investigations etc.) has inbuilt video conferencing capabilities started being used regularly.
eICU : eICU’s where smaller ICU’s are connected to highly trained experienced intensivists in larger ICU’s are now a reality. One of the largest such networks operates from Apollo Hospitals Hyderabad where 15 ICU’s are connected. 600 plus teleICU consults in subspecialoitries have already been given.
Public Private Partnerships – a few illustrations
a) Himachal Pradesh . The first Telehealth PPP project in India commenced 5 years ago . Over 18,500 teleconsultations were given at a height of 14,500 ft. The world’s first 24/7 Tele emergency Services has seen about 1300 patients. Today we have four different Telemedicine Centres in Himachal Pradesh
b) Over 1 million teleconsultations have been provided under the Mukhyamantri Arogya Kendram (e-UPHC)- project covering 182 Centres from October 2016.
c) Jharkhand Digital Dispensaries programme In the first 15 months alone 328,648 patients have attended these Digital Dispensaries
d) Uttar Pradesh Telemedicine programme in the first one year 141,793 patients visited 114 Government Community Health Centres
e) Uttar Pradesh Teleradiology PPP program – Systematic implementation of operational activities, beginning from site development and installation of IT equipment to training of human resource and trial testing for assessing functional status of Centres has led to commissioning of 127 teleradiology centres in rural UP – a mammoth undertaking by any standards. On an average 360 images are reported daily with a turn around time within 4 hours
f) Tele ophthalmology A major project is being carried out in 115 existing Community Health Centres / Vision Centres run by the Department of Health and Family Welfare, Government of Andhra Pradesh in 13 districts. Through this Mukhyamantri e-Eye Kendram or MeEK project 1,5 million patients have been screened in 2 years. 355,000 fundus examinations were done remotely by 30 Opthalmologists from Chennai .
g) National Thermal Power Corporation . Located in rural Assam 30 km from the China Border this Telemedicine enabled center has made a major difference.
2019
Extra-terrestrial Telemedicine . The ultimate in Remote Health Care would be to assist in providing health care to India’s first Vyomanauts in Outer Space . After editing a special supplement on “ Extra Terrestrial Neurosciences” for Neurology India and presenting the only medical paper at the Human Spaceflight Programme organised by ISRO, I have even offered my services !! 2020 Academic contributions – The crusade for popularizing telemedicine has included the presentation of more than 400 papers in regional, national and international meetings in India and 105 overseas . Over 180 articles have been published, on Telehealth including 45 in peer-reviewed journals and chapters in textbooks
Conclusion:
The journey has been exhilarating . I have no regrets for taking the road less travelled by. Encomiums and accolades received on reaching the destination is only ephemeral. The greatest danger for most of us, is not that our aim is too high and we miss it, but that it is too low and we reach it. The TSI should not believe in following high standards. We should set them. We no longer should strive to achieve world class. The world should strive to achieve India class. Looking back, the growth of telehealth during the last 20 years has been rather slow – many of us are in a hurry, impatient, wanting to get things done yesterday !!. The first decade was spent in evangelising the product, developing the product and generally creating awareness . For a product to excite the masses it must elicit customer delight and cater to the consumer. A major stumbling block retarding the take off of telemedicine is WiiiFM ( What is in it For Me). Every member of the telehealth ecosystem needs to get a RoI ( Return on Investment) not necessarily monetarily alone. In the third decade of telehealth business models are mandatory. Revenue generation is a must for sustenance. Philanthropy and corporate social responsibility can initiate an activity not maintain it.
Epilogue: Not in my wildest imagination would I have ever expected the slow incremental annual growth to radically transform into an explosion. A strand of RNA has become the Global CTO ( Chief Transforming Officer) for Telehealth. Contactless Health care will be the new normal.Distance will become meaningless. Geography will become History!. Recognition of Telemedicine by Insurance companies augurs well. Formal recognition of importance of Telemedicine by the Govt of India and state governments will make all the difference, I once gain thank the TSI for bringing out a Newsletter . Hopefully the newsletter will bring our ever expanding family closer .
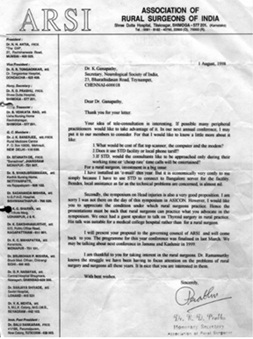
Fig 1 Earliest communication for starting Telemedicine
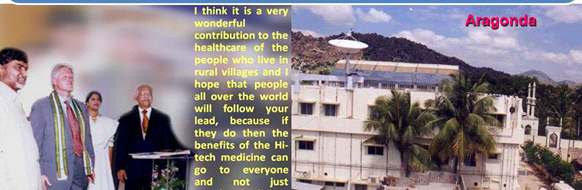
Fig 2 Inauguration of world’s first VSAT enabled village hospital for Telemedicine March 24th 2000 @Aragonda, Andhra Pradesh
 Tele-Ophthalmology – in a COVID world – Opportunities and Challenges
Tele-Ophthalmology – in a COVID world – Opportunities and Challenges
Dr. T. Senthil, MBBS DO FICO. Founder and CEO Welcare Health Systems Pvt ltd – Honorary Secretory, Telemedicine Society of India Tamil Nadu Chapter. Dr. Senthil is an Ophthalmologist and Healthcare Entrepreneur, He established Welcare Health Systems in 2014 which has grown to become Indias Largest Teleophthalmology Company. He can be reached at senthil@welcaretelemed.com.
COVID 19 has brought in a drastic change in adoption of Teleophthalmology among Ophthalmologists in India. Since patients were not able to reach hospitals, and social distancing became the norm, hospitals in Corporate, Govt and Non-Profit sector started looking for Teleophthalmology Solutions to reach out to their patients. In Ophthalmology Telemedicine was used primarily in three scenarios. 1) Screening for Diseases such as Diabetic Retinopathy, Retinopathy of Prematurity etc. 2) Diagnostic Consultations. 3) For Long term follow ups of patients.
Screening for Diseases through Teleophthalmology has been the most successful of the above three models. There are many successful Screening projects in Teleophthalmology world over which has reached out to millions of patients. However, Challenges faced by Screening model providers are cost of the Technology such as fundus cameras, Internet connectivity, Paying capacity of patients etc.
 |
|
The Diagnostic Consultation approach started getting traction during the COVID lockdown, since patients were not able to reach hospitals- they wanted to connect to Ophthalmologists from their homes. There was a huge spike in Teleconsultations during the initial lockdown periods. Hospitals and Clinics started teleconsultation services to reach patients. Many platform companies were able to generate patients to Ophthalmologists for consultation. The teleconsultation slowly started decreasing as Hospitals / clinics opened.
Challenges in Ophthalmic Teleconsultation
a) Ophthalmology diagnosis includes a few basic tests such as Examination of Eye on a Slit Lamp, Fundus Examination, Refractory error examination etc which cannot be done in the patients’ homes since the equipment’s are not available for these tests.
b) The willingness of Patients to pay for a online consultation was very poor.
c) The Ophthalmologists also have a lot of apprehension on missing Diagnosis using a Teleconsultation mode.
 The most effective model during the COVID time for Ophthalmology was for follow up of patients such as Postoperative patients where advise was given on Medication changes, or Tele triage wherein patients were seen online and decision was taken if they have to come to Hospital or can be advised online, or even if they come to hospital which specialist they had to see and so on.
The most effective model during the COVID time for Ophthalmology was for follow up of patients such as Postoperative patients where advise was given on Medication changes, or Tele triage wherein patients were seen online and decision was taken if they have to come to Hospital or can be advised online, or even if they come to hospital which specialist they had to see and so on.
For Teleophthalmology to Succeed
1) Low cost Diagnostic Devices such a Fundus Cameras and ROP cameras to be available in the market.
2) At Home Screening devices for Intra Ocular Pressure Measurements, Refraction and Visual acuity Measurements, Fundus / Anterior Segment Imaging to be innovated and made available.
3) Medico Legal Clarity and Data Protection Clarity to be brought in so that Doctors will be more comfortable in doing Teleconsultations.
 Mobile Teleopthalmology
Mobile Teleopthalmology
Dr. Sheila John, Consultant Ophthalmologist, Head of Teleophthalmology and E-Learning, Sankara Nethralaya, Chennai.
Mobile Tele-ophthalmology is evolving into an integral clinical tool in the Indian health care system. In a developing country like India, the ophthalmologist-patient ratio stands at a dismal 1:10,000. What makes this wide gap between demand and availability of eye care even more critical is its inequitable spread, 70% of the nation’s citizens live in rural areas while 70% of its eye care professionals live in urban areas.
Mobile Tele-ophthalmology BUS may potentially provide health services to underserve and remote rural populations who otherwise may not have access to specialized eyecare. Eye screenings are conducted within the community, often in schools, community halls, and places of workship.Bringing the facility directly to the patients allows health professionals to diagnose and prevent vision threatening diseases such as diabetic retinopathy, glaucoma, age-related macular degeneration and others By detecting causative blinding disease early on mobile, teleophthalmology allows for timely referral to appropriate experts and consequently, earlier treatment. However, on-site screenings may utilize the state of art equipment including an automated refractor, slit lamp with Applanation tonometer, Non-mydriatic retinal camera and others. An ophthalmologist is available in person at the hospital to do teleconsultations with the patient and develop an assessment and treatment plan for the screened patients. The ‘Mobile Refraction Van ‘accompanies the teleophthalmology van to the villages, addresses the refractive error, and dispense spectacles to rural people at campsite.
As an institution committed to its founding principle of cost free service with a personal touch to those who cannot afford to pay, Sankara Nethralaya realized right from the time of its inception that for every single indigent patient who visited its centers seeking cost free eye care there were two such patients outside needing such care. It also realized that patients in rural areas may not avail eye care dispensed at a base hospital in the city owing to several socio-economic factors and the only way to dispense preventive and curative eye care to this segment would be through outreach programs. ‘Mobile Teleophthalmology’ holds great potential to improve the quality, access and affordability in eye care especially for patients in rural areas by reducing the need for travel and providing virtual access to a super-specialist right at their doorstep.
 Best practices!
Best practices!
Indiritta Singh Dmello, Director, Hospital Guide Foundation (An Oxford graduate in Politics, Philosophy & Economics with a PG Diploma in Medical Law & Ethics-National Law School, Bangalore)
“The developed India will not be a nation of cities. It will be a network of prosperous villages empowered by telemedicine, tele-education & e-commerce”-Dr. A.P.J. Abdul Kalam.
It is paradoxical that even though India has emerged as a hub for medical tourism, we are unable make healthcare accessible and affordable to the masses in India. As per the WHO statistics, India is far below the recommended Doctor Patient Ratio (recommended ratio 1:1000 & India1:1700). Further compounding the problem is that only 26% of these Doctors are present for 70 percent of the population in rural areas.
This is where Telemedicine plays a pivotal role in addressing this gap. Telemedicine is a tool that makes healthcare accessible and cost effective by engaging the Doctors and patients remotely through an integrated technology platform. This platform could be as basic as a simple Audio Visual with a software for patient details or as advanced as integrated diagnostic equipment, remote monitoring of Intensive Care Unit Patients or even remotely conducting a surgery.
Hospital Guide Foundation (HGF) has been running a Telemedicine project with the Govt of Uttar Pradesh in the rural area of Western UP, supported by the Doctors of National Heart Institute & Sita Ram Bhartia Institute of Research & Technology at New Delhi. While it is a Telemedicine project, the objective is to provide comprehensive healthcare with Telemedicine being an enabler. At HGF the following key factors were observed for making a Telemedicine project successful.
Holistic Approach: Telemedicine delivers significant advantages for the patients only with a complete treatment and support mechanism – ensuring tests & medicines, setting right expectations, counseling (about the process, disease & treatment), driving awareness, ensuring compliance with (tests, medicines & life style) and pro-active follow ups, which helps gain patient confidence & cooperation therefore delivering much better results.
Seemless process: Multiple touch points have to be managed seamlessly between patients, nurses,Doctors and telemedicine specialists for enabling a great healthcare experience. This makes it even more challenging in rural areas where we grapple with basic problems like electricity. Coordination to perfection is key for a sustainable telemedicine project, specially when the Doctor’s limited time should be well spent on communicating with patients rather than waiting for them.
Optimal technology: is also essential for a superior Doctor & patient experience. For eg the quality of internet bandwidth, audio visual can affect the dialogue between patients and Doctors who are trying to communicate remotely on sensitive health issues. The quality of communication will have a direct impact on the diagnosis, prognosis and treatment.
Quality diagnostics: Similarly, well calibrated high tech diagnostics is essential for the patients to get the right diagnosis, prognosis and treatment.
With the onset of the Pandemic COVID 19, Telemedicine has gained the much needed impetus that it has been yearning for. As it has become an important enabler in Healthcare delivery, not only for reasons of accessibility, affordability but for reasons of safety. In a country where there are several Telemedicine projects running in silos, it is important to continuously share best practices , for which Telemedicine Society of India (TSI) is a great platform & this newsletter a great initiative. With the astute leadership of TSI, I have no doubt that Telemedicine will be on a trajectory it so deserves!
 Train to Practice Telemedicine Guidelines
Train to Practice Telemedicine Guidelines
Ms. Bagamishika Puhan, Advocate, Legal Advisor and EC Member, Telemedicine Society of India, Member, Indian Society for Clinical Research.
On April 04, 2020, after a tumultuous yet short ride, a group of TSI members came together to unfurl the Train to Practice project. This was the culmination of an informal mandate received from a benefactor to train and educate as many registered medical practitioners (RMPs) about the nuances of the Telemedicine Practice Guidelines (TPG) in particular and telemedicine in general.
The Society pioneered work in the field of telemedicine over the past many years, and now, is at the helm of inculcating the best practices in the field and has been successful in training over 3500+ RMPs directly under the project, and about 15000+ RMPs through the volunteers.
In this exercise, the focus has been to ensure that the participants take away an acute understanding of the legal aspects of telemedicine (TPGand allied laws), how to marry the legal concepts to their clinical practice, and also a basic understanding of how and when to triage a patient by means of telemedicine. As we continued with the project, we added another module which lends a helping hand to the practitioners who want to get started right after the discussion, with their own kit of telemedicine.
The project has witnessed roaring applause from various factions including the much revered Armed Forces Medical Services for the volunteering efforts and the dynamism of the project and the team. We have also sought support from entities who believe in this social and evolving practice of telemedicine. As the awareness amongst the user increases, we will continue to ensure that safety is not compromised, and we will continue to impart the necessary education concerning safe and convenient practices around telemedicine.
We welcome participation of volunteers to train, to learn, and to contribute to this endeavor of the Society in any manner and capacity that they wish to associate with the Society. Learn more at https://tsi.org.in/learn
 History and Evolution of Telemedicine – Samuel Morse and Telegraph
History and Evolution of Telemedicine – Samuel Morse and Telegraph
Dr. Sunil Shroff, President, Tamil Nadu Telemedicine Society of India, Consultant Urologist & Transplant Surgeon.
History and Evolution of Telemedicine – Samuel Morse and Telegraph (First of Ten important milestones). “The Past supplies the key to the Present and Future“ ~ Ancient Historian. The history of telemedicine is the history of evolution of distance communication. If it was not for the legacy laid down by many of the scientists, telemedicine may have never evolved as it has done currently.The start of this was the invention of the public telegraph system set up by Samuel Morse. Why did Samuel who had developed a reputation as a portrait painter go on to invent the telegraph system?
This is an interesting piece in the history of communication. Apparently he was hired to paint a portrait of a famous person and travelled out of his town. Back at home his wife fell ill and died of heart attack and it took Samuel days to reach back home and when he did return the wife’s funeral had already taken place.He was so upset with this episode in his life that he left his art career and started looking at ways to establish a way to communicate information at a distance. His pursuit lead him to become interested in the telegraph system.
 He went on to invent a single-wire telegraph system and the first Intercity public telegraph services were set up between Washington and Baltimore in 1844. In almost all the wars that followed the telegraph was used by the military to order medical supplies, transmit list of casualty and it is probable that some use of the telegraph in its early decades involved medical consultations.He was also the co-developer of Morse code that helped the commercial use of telegraphy. One of such codes was the internationally recognized distress signal SOS. The SOS letters were chosen because they are easy to transmit in Morse code: “S” is three dots, and “O” is three dashes.
He went on to invent a single-wire telegraph system and the first Intercity public telegraph services were set up between Washington and Baltimore in 1844. In almost all the wars that followed the telegraph was used by the military to order medical supplies, transmit list of casualty and it is probable that some use of the telegraph in its early decades involved medical consultations.He was also the co-developer of Morse code that helped the commercial use of telegraphy. One of such codes was the internationally recognized distress signal SOS. The SOS letters were chosen because they are easy to transmit in Morse code: “S” is three dots, and “O” is three dashes.
Telemedicine – News from India & AbroadIndia500% rise in healthcare teleconsultation in India, 80% are first-time users: Report Digital Care: The Way Forward for Management of Chronic Conditions Telemedicine is the roadmap to improve medical Care in rural areas : Ayush Mishra Today technology can make physicians available to patients: Sunil Wadhwani Telemedicine Guidelines Released in India Notified and Gazetted InternationalTelehealth Services: A Post COVID-19 Reality? Heart Failure Assessment Via Telemedicine Digital Health Unplugged: August news team debrief Telemedicine Market- Growth Insight, Rising Demand, Share and Healthy CAGR in the Upcoming Forecast 2024 |
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter. |
Submission may be sent to – tsigrouptn@gmail.com
Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff
Editors – Dr. Senthil Tamilarasan & Dr. Sheila John
Design – Sankara Nethralaya
Technical Partner- www.medindia.net
