Official Newsletter of Telemedicine Society of India
What is New?
The National Institute of Mental Health and Neurosciences (NIMHANS), Bengaluru, has released the Guidelines on Digital Mental Health Applications following a national consultative meeting involving experts, policymakers, WHO India, UNICEF, and technology stakeholders. The guidelines provide recommendations for app developers, mental health professionals, and users to ensure safe, ethical, and evidence-informed use of digital mental health tools in India. Key focus areas include transparency, data privacy, AI disclosure, crisis support integration, professional oversight, and safeguards against emotional dependency on AI chatbots. The document marks an important step toward responsible digital mental healthcare in the country.
Last month also marked an important milestone in digital health education, as the first batch of the Certificate Course in Digital Health from The Tamil Nadu Dr. M.G.R. Medical University successfully completed the programme. Certificates were distributed during the OTICIA event, recognising the efforts of participants who completed the course and strengthened their understanding of emerging digital health technologies and practices.
Another major healthcare development this month has been the Supreme Court of India’s landmark directions to strengthen Intensive Care Unit (ICU) infrastructure and emergency medical preparedness across the country. In its order, the Court emphasised that access to emergency and critical care is an integral part of the Right to Life under Article 21 of the Constitution. The Court approved a three-tier ICU classification system and directed States and Union Territories to conduct gap assessments of ICU infrastructure, manpower, and emergency services. It also highlighted the need for advanced ambulance networks, tele-ICU systems, GPS-enabled hospital coordination platforms, and stronger nursing training standards linked to ICU exposure. The judgment is expected to play a transformative role in improving critical care services, emergency preparedness, and equitable access to life-saving healthcare across India.
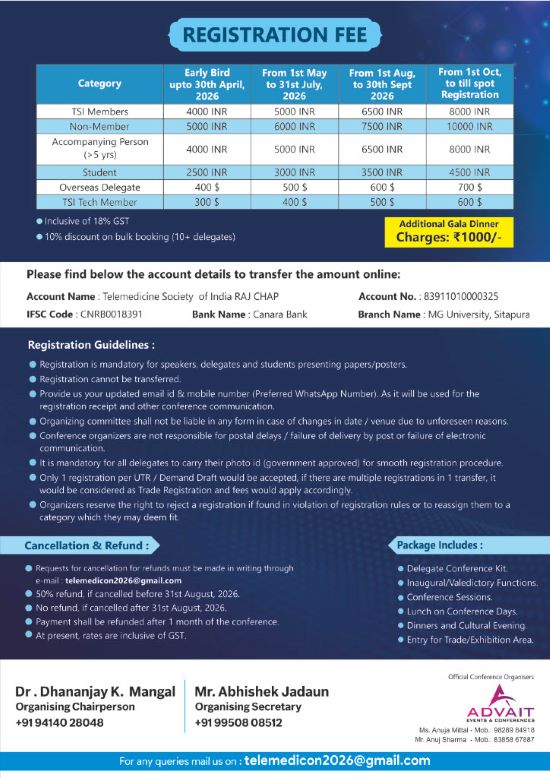
The month of May, however, has otherwise been relatively quiet with limited activities and events. Nevertheless, the focus continues on building capacity, strengthening collaborations, and planning upcoming TELEMEDICON2026 in Jaipur. Registration is now open and I do hope you will avail the early bird registration option .
Thank You Dr. Sunil Shroff Chief Editor President, TSI
Supreme Court Order Signals a Turning Point for Tele-ICU and Digital Health in India
Dr. Sunil Shroff President, Telemedicine Society of India | Consultant Urologist & Transplant Surgeon
India’s healthcare system may be on the verge of a major transformation following the recent Supreme Court order on ICU infrastructure and critical care preparedness. While the judgment primarily addresses deficiencies in Intensive Care Unit (ICU) facilities, its larger significance lies in the Court’s strong endorsement of tele-ICU systems, digital coordination, GPS-enabled healthcare networking, and technology-driven emergency care.
For the digital health ecosystem, this is perhaps one of the clearest judicial recognitions that technology is no longer optional in healthcare delivery — it is essential. Beyond Bricks and Mortar: The Need for Digital Critical Care
India faces a severe shortage of intensivists, trained critical care personnel, and advanced ICU facilities, especially outside metropolitan cities. Building physical ICUs alone will not solve the problem. Even if infrastructure expands rapidly, specialist expertise cannot be distributed evenly across thousands of hospitals overnight.
This is where tele-ICU systems become transformative.
Tele-ICU models enable specialists located in tertiary centres to remotely monitor, guide, and support healthcare teams in peripheral hospitals through audio-video links, real-time patient monitoring, and digital data sharing. A critically ill patient in a district hospital can effectively receive expert input from a specialist located hundreds of kilometres away.
The Supreme Court’s explicit endorsement of tele-consultation and tele-ICU systems is therefore highly significant. The Court recognized that such systems can reduce unnecessary patient transfers, improve stabilization of critically ill patients, and provide immediate access to specialist advice during emergencies.
A National GPS-Enabled Healthcare Grid
One of the most forward-looking aspects of the order is the direction to explore a nationwide GPS-based digital platform mapping healthcare facilities and ICU availability across India.
Such a system could fundamentally change emergency healthcare delivery.
Today, families often spend precious hours searching for available ICU beds, ventilators, or specialist facilities. Ambulances move from one hospital to another without centralized coordination. Information gaps frequently delay treatment during the “golden hour” of emergency care.
A real-time digital health grid could address these inefficiencies by:
Mapping ICU bed availability
Identifying hospitals with ventilator support
Displaying facility levels and specialist services
Enabling inter-hospital referrals
Coordinating emergency patient transfers
Supporting tele-consultation between institutions
Importantly, the Court emphasized that hospital coordination should happen institutionally and digitally, rather than leaving distressed family members to navigate the system themselves.
Digital Health Infrastructure is Public Health Infrastructure
The order reflects an important shift in thinking. Digital infrastructure is increasingly being recognized as core healthcare infrastructure.
Over the last decade, India has made significant progress in digital public infrastructure through initiatives such as Aadhaar, UPI, CoWIN, Ayushman Bharat Digital Mission (ABDM), and eSanjeevani telemedicine services. However, critical care integration has remained fragmented.
The Supreme Court’s observations could accelerate:
National interoperability standards
ICU data integration
Real-time bed management systems
Emergency response dashboards
Telemedicine integration into routine hospital workflows
AI-supported triaging and monitoring systems
Such integration could become especially valuable during pandemics, disasters, road traffic emergencies, and mass casualty events.
Telemedicine Must Move from Pilot to Policy
India already has successful examples of telemedicine and tele-ICU programmes in government and private sectors. Yet most initiatives remain isolated pilots rather than integrated national systems.
The Court’s endorsement provides an opportunity to move tele-ICU from experimentation to mainstream policy implementation.
For this to succeed, several areas require attention:
Reliable broadband connectivity for hospitals
Standardized tele-ICU protocols
Cybersecurity and patient data protection
Workforce training
Reimbursement and funding mechanisms
Integration with ABDM digital health records
Importantly, tele-ICU systems should complement — not replace — physical critical care infrastructure.
A Vision for Connected Critical Care
The Supreme Court order is more than a healthcare directive; it is a blueprint for connected critical care in India.
The future ICU may no longer be confined within the walls of a single hospital. Instead, India could move towards a digitally networked ecosystem where expertise travels faster than patients, where ambulances become mobile critical care units, and where technology helps bridge the vast urban-rural healthcare divide.
For the digital health community, this order is both a validation and a call to action. The challenge now lies not in recognizing the importance of telemedicine and digital coordination, but in implementing them at scale with urgency, equity, and sustainability.
Reflections from the National Consultative Meeting on Digital Technologies for Mental Health: Evolving Policy and Regulatory Recommendations for Safe Use
Smriti Joshi Chief of Clinical Services & Ops Member Board of Directors, Wysa
15–17 April 2026 | Bengaluru I had the opportunity to participate as an invited expert at the National Consultative Meeting on Digital Technologies for Mental Health: Evolving Policy and Regulatory Recommendations for Safe Use, convened by the NIMHANS–ICMR Centre for Advanced Research in Digital Interventions for Mental Healthcare (NIMHANS–ICMR CAR-DIMH).
The consultation brought together 126 participants from diverse backgrounds—mental health professionals, technology experts, researchers, developers, public health specialists, policymakers, educators, civil society organisations, and representatives from multiple ministries and agencies. What made the meeting particularly valuable was that conversations moved beyond disciplinary silos and focused on a shared question: how do we build digital mental health systems that are useful, safe, and realistic for the Indian context? Digital technologies are increasingly being positioned as one way to address longstanding gaps in mental healthcare—particularly workforce shortages, uneven access to services, stigma, and increasing demand. However, alongside rapid growth in digital mental health applications, important concerns around safety, evidence, privacy, accountability, and implementation are also becoming more visible.
Digital technologies should support care—not replace it
Across discussions, there was considerable agreement that digital mental health tools should strengthen existing systems rather than function independently of them. Participants discussed the potential role of digital tools in improving access, supporting continuity of care, psychoeducation, self-management, and earlier help-seeking, while recognising that technology alone cannot solve structural challenges in mental healthcare.
AI generated both enthusiasm and caution
Conversations explored opportunities around improving access, reducing administrative burden, and supporting clinical workflows, while also raising concerns around emotional dependency, misinformation, overreliance, privacy, and limitations in responding to complex psychological needs.
Governance and safeguards emerged as central concerns
Participants highlighted the need for stronger safeguards around transparency, privacy, crisis response mechanisms, evidence, and accountability.
Recommendations Emerging from Discussions
Develop risk-based governance approaches for digital mental health technologies
Strengthen quality, transparency, and safety standards
Build digital mental health literacy among providers and users
Prioritize responsible digital use among children and adolescents
Strengthen evidence generation and implementation research
For readers interested in exploring the consultation proceedings, stakeholder-specific guidelines, and policy recommendations in greater detail, the following resources are available:
For those working in telemedicine, digital health, and healthcare delivery, the discussion increasingly shifts from whether digital mental health technologies should be used toward how they can be implemented responsibly, integrated into existing systems, and evaluated meaningfully.
Rijuven Medicare Wins AP MedTech Innovation Challenge 2026
Uma Mahesh Vice President – Rijuven Medicare India Pvt Ltd Treasurer – Telangana State Chapter, TSI EC Member – National TSI
Rijuven Medicare India Pvt Ltd emerged as the winner in the Remote Patient Monitoring & Telemedicine category at the prestigious AP MedTech Innovation Challenge 2026, a pioneering state-led initiative launched by the Government of Andhra Pradesh to pilot and scale AI-driven healthcare technologies within the public healthcare ecosystem.
Spearheaded by Andhra Pradesh Chief Minister N. Chandrababu Naidu and Health Minister Shri Y. Satya Kumar Yadav, the initiative marks the first time in India that multiple startups have simultaneously piloted AI-enabled healthcare solutions across state-run hospitals.
The AP MedTech Innovation Challenge was launched in November 2025 in association with the Ratan Tata Innovation Hub. A total of 297 startup applications were received, of which 18 innovators were shortlisted through a rigorous multi-stage evaluation process.
The selection process focused not only on technological innovation, but also on real-world healthcare impact and deployability within the government healthcare system. Proposals were screened by the Committee for Applied Technologies in Health (CATH), with scientific and clinical validation support from the Indian Council of Medical Research (ICMR) and the Indian Institute of Science (IISc).
As part of the challenge, participating startups deployed 40 distinct medical devices across 18 Government General and District Hospitals in Andhra Pradesh. Within just 37 days, more than 12,000 patients were screened, significantly improving diagnostic speed and clinical accuracy.
Speaking at the valedictory session held at Mangalagiri, Andhra Pradesh Health Minister Shri Satya Kumar Yadav stated that Andhra Pradesh has become the country’s first “Lighthouse State” in implementing Artificial Intelligence-based healthcare services through the MedTech Challenge.
About Rijuven
Rijuven (India & USA) is a medical innovation company focused on transforming grassroots healthcare delivery through patented healthcare technologies. Its flagship “Clinic in a Bag” solution is designed to modernize healthcare delivery in both rural and urban settings by enhancing capacity, efficiency, accessibility, and outreach.
The solution aims to strengthen primary healthcare services for both communicable and non-communicable diseases, enabling healthcare providers to reach and serve millions more effectively.
Rijuven expressed pride in being selected among the 18 finalists for pilot implementation under the AP MedTech Innovation Challenge and described the recognition as a significant milestone for the organization.
The company conveyed its gratitude to the Government of Andhra Pradesh, Hon’ble Health Minister Shri Satya Kumar Yadav, the GGH Kurnool team, evaluators, clinical teams, mentors, and supporters who contributed to the success of the initiative.
Special thanks were also extended to mentors and well-wishers at the Telemedicine Society of India (TSI) for their continued guidance and encouragement throughout the journey.
“Pilgrimage Telemedicine”
Dr Nitha V Panicker Secretary, TSI Kerala Chapter
The Kerala Kumbh Mela, held on the banks of the Bharathapuzha River (Nila) at Thirunavaya, in Malappuram district, is a centuries-old sacred congregation widely revered as the “Kumbh of the South.” Rooted in holy river bathing, Vedic rituals, ancestral worship, and spiritual traditions, this historic Maholsavam was conducted from January 18 to February 3, 2026, witnessing the participation of approximately 4–5 lakh pilgrims. The event featured sacred immersions, traditional rituals, and the Nila Aarti, making it one of the largest and most spiritually significant religious congregations in South India, symbolizing Kerala’s deep-rooted cultural and spiritual heritage.
As part of this historic gathering, a comprehensive Pilgrimage Telemedicine Programme was implemented to ensure accessible, timely, and quality healthcare services for pilgrims. The programme was organized in association with Mata Amritanandamayi Math, Juna Akhada, Amrita Institute of Medical Sciences, the Amrita Telemedicine Unit, and the Telemedicine Society of India – Kerala Chapter. This “Pilgrimage Telemedicine” facility was inaugurated by Kummanam Rajasekharan, Former Governor of Mizoram, along with Dr. Jaggu Swami Hospital Administrator, AIMS, Swamini Athulyamrita Praana (Mata Amritanandamayi Math Thirur), Brahmachari Pramod MA Math Haridwar , Dr. Sreekumar C (Professor of General Surgery & Telemedicine Medical Officer), and Mr. Rajeesh M. V (Telemedicine System Administrator), marking a significant milestone in integrating spiritual pilgrimage with modern digital healthcare systems.
Through advanced telemedicine infrastructure, Thirunavaya and Tavanur were digitally connected to Kochi, enabling pilgrims to receive direct expert medical guidance from Amrita Hospital through real-time teleconsultations. More than 400 pilgrims benefited from these services, receiving specialist consultations, clinical guidance, and timely medical support without the need for physical hospital travel. This initiative stands as a landmark model of faith–healthcare integration, demonstrating how digital health technologies can effectively support large-scale pilgrimage events by ensuring accessibility, and quality healthcare delivery while preserving the spiritual sanctity of the sacred gathering.
“Pilgrimage Telemedicine” facility, inaugurated by Kummanam Rajasekharan, Former Governor of Mizoram,
Tele Consultation
Why Over 66 Million Americans Use AI for Healthcare
The rise of AI-driven healthcare is transforming the American medical landscape. A landmark April 2026 West Health-Gallup study reveals that 66 million U.S. adults now consult AI chatbots for medical advice.
Rather than replacing doctors, most patients use generative AI to supplement visits, researching symptoms before appointments or interpreting diagnosis data afterward. However, 14 million Americans have used AI as a substitute for professional care, driven by high healthcare costs and accessibility barriers.
Despite this trend, trust remains low, with many reporting concerns over medical accuracy and safety. For providers, this digital shift highlights an urgent need to integrate AI tools into patient workflows to ensure responsible, guided health outcomes.
Enhancing Patient Confidence: The Role of AI in Pre- and Post-Visit Care
The study shows how AI tools act as a digital bridge between patients and providers. By leveraging chatbots for pre-visit symptom checks and post-visit data interpretation, users gain the confidence and clarity needed to navigate complex clinical conversations, making care more collaborative.
Before the visit: 59% of patients use AI to research symptoms so they can ask better questions.
After the visit: 56% of patients use AI to interpret medical jargon or get more details on a diagnosis.
For Confidence: 46% of users say AI makes them feel more confident when talking to their healthcare provider.
AI Chatbots as an Essential Alternative for Cost-Effective Healthcare Access
While AI primarily serves as a support tool, it is increasingly becoming a vital source for those facing healthcare structural barriers. For many people, chatbots are not just a choice but an essential alternative driven by high costs and limited access.
This shift highlights a growing socioeconomic divide, where AI fills the gap for underserved populations who feel marginalized or excluded from traditional clinical care. While most use it as a supplement, a smaller but significant group is using AI as a substitute:
Avoidance: About 14% of people (roughly 14 million people) decided not to see a doctor specifically because of the guidance they received from AI that makes them potentially substitute professional consultation.
Barriers: While 27% of people turn to AI tools over doctors primarily due to cost, 21% of people use AI due to lack of time, or past negative experiences where they felt dismissed by human doctors (21%).
Income Gap: There is a sharp economic divide; 32% of lower-income users used AI because they couldn’t afford a doctor, compared to only 2% of high-income users.
High Usage vs. Low Trust: The Trust Deficit in AI Medical Accuracy
According to the West Health-Gallup data, the paradox of AI healthcare lies in the trust gap. Despite widespread use, skepticism remains high, with many users questioning the accuracy of AI’s information, 11% of users are flagging safety risks, a trend that indicates a critical need for oversight.
Despite the high usage, trust in AI’s medical accuracy is surprisingly low as follows:
Divided Trust: Only 33% of users say they actually trust the information they receive from AI; and the rest are neutral or distrustful.
Strong Trust: Only 4% of users strongly trust the health information accuracy of these AI tools.
Safety Risks: 11% of users reported that AI gave them medical advice they believed was unsafe.
How AI Drives Wellness Tracking and Medication Research
AI tools are now a common first point of contact for healthcare management, providing immediate access to medical information. From tracking daily wellness habits to identifying physical symptoms and researching medication risks, these platforms offer real-time data that helps users monitor and manage their health more independently.
The most frequent reasons for consulting AI tools include:
Nutrition and exercise (59%): Most common for lifestyle and wellness guidance.
Physical symptoms (58%): Used frequently for preliminary symptom-checking.
Medication side effects (46%): Helps users understand pharmaceutical risks and interactions.
Mental health concerns (24%): Provides a private avenue for emotional and psychological support.
Evidence-Based Oversight: Global AI Frameworks and Safety Standards
To bridge the gap between AI utility and clinical safety, global healthcare systems are implementing rigorous oversight. Beyond user trends, new regulatory frameworks and institutional case studies demonstrate a shift toward standardized, transparent, and legally accountable AI integration in healthcare.
As of January 1, 2026, several major U.S. states have enacted laws specifically to address the risks of AI in clinical settings:
The most direct law of California ‘AB489’ prohibits AI developers from pretending to be a doctor. Systems cannot use any design elements, phrases, or titles that imply the AI holds a medical license.
The ‘Texas Responsible Artificial Intelligence Governance Act (TRAIGA)’ law requires conspicuous written disclosure from physicians. Doctors must tell patients if they are using AI for diagnosis or treatment. If they don’t, they face fines up to $200,000 per violation.
For mental health or wellness chatbots, California now mandates crisis protocols ‘Safety Protocols (SB 243).’ According to this law, if a user mentions self-harm, the AI is legally required to immediately stop and provide a referral to a human crisis provider or operator’s internet website.
Universal Regulatory Initiatives and Clinical Integration of Healthcare AI
On a global scale, the Organization for Economic Co-operation and Development (OECD’s) 2026 framework, ‘Scaling AI in Health,’ introduces international standards for ‘Model Cards.’ The model cards are digital transparency labels that detail an AI’s training data, limitations, and accuracy.
These transparency labels certify that AI tools are trained on data representing diverse populations, ensuring equitable care. By setting these benchmarks, the OECD aims to standardize clinical safety and data integrity, transforming AI from a localized tool into a globally regulated health resource.
Professional healthcare systems are now countering public chatbots with validated AI integrated into official workflows. At the American Medical Group Association (AMGA) 2026 Annual Conference, clinical leaders presented ‘Ana in Action,’ a study on using automated AI assistants to reduce administrative burden. This approach maintains patient-centric oversight, ensuring AI acts as a clinical support tool rather than a standalone replacement.
India’s Press Information Bureau (PIB) recently launched the Strategy for Artificial Intelligence in Healthcare for India (SAHI), a national framework focusing on trust, diversity, and inclusion. The mandate prioritizes localized datasets to ensure AI algorithms are representative of India’s unique demographics, while establishing ethical oversight to strengthen public confidence in digital health.
The Future of Healthcare: Balancing AI Innovation with Patient Safety
The West Health-Gallup study confirms AI is reshaping healthcare as a vital support tool. While improving accessibility, its rise highlights urgent needs for medical accuracy and safety. Moving forward, health systems must prioritize ethical integration and clinical oversight.
Ultimately, AI should bridge equity gaps and enhance care, serving as a supportive resource rather than a replacement for professional medical consultation.
Is telehealth good enough for autism diagnosis? Yes, autism diagnosis has gone virtual and proven to be pretty effective during the COVID-19 pandemic, according to a new study.
Pandemic Pause: Autism Diagnoses Put on Hold by COVID-19
When the COVID-19 pandemic led to clinic closures and limited in-person interactions to masked encounters, autism diagnoses for many children were put on hold.
For Katherine Meltzoff, a professor of education at UC Riverside, the disruption exposed a critical gap and an opportunity.
“We were trying to figure out how to adapt autism diagnostics to be done virtually,” Meltzoff said. Telehealth Takes the Lead in Autism Detection Amid COVID-19
The result is a set of telehealth tools described in a paper published in the Journal of Autism and Developmental Disorders that are designed to help clinicians diagnose autism remotely, especially for children who are older or have developed verbal communication skills.
Telehealth’s Growing Role in Autism Care
Meltzoff explained that there are already a number of validated virtual autism assessment tools for children aged 3 and below, and for those with minimal spoken language, but not for those who are older and have more verbal speech.
“Telehealth seems to work really well for the kids that have more obvious symptoms and that are younger,” said Meltzoo, the lead author.
Meltzoff’s research tested whether these virtual assessments could match the accuracy of traditional, in-person evaluations, offering a potential solution to long-standing barriers in autism diagnosis.
More Than Tests: Diagnosing Autism Through Behavior
Autism spectrum disorder is not diagnosed through a single medical test. Clinicians observe how a child communicates, interacts socially, and responds to the world, while also reviewing developmental history.
“We diagnose it behaviorally, so we’re looking at behaviors that the child displays,” Meltzoff explained.
Lost Expressions Behind the Mask: The Challenge of Autism Evaluation During COVID-19
During the first months of the COVID-19 pandemic, autism assessments came to a halt due to the widespread ‘shelter at home’ guidelines. As restrictions began to ease, assessments remained challenging because facemasks worn by the clinicians and family members hid facial expressions, which are a large part of the social communication and behaviors under evaluation.
In traditional clinical settings, those observations happen during carefully structured, in-person sessions. For her study, Meltzoff recreated those interactions online. Using video conferencing tools, clinicians guided parents through activities — such as calling a child’s name or engaging in play — while observing how the child responded. For older children, clinicians interacted directly with them through conversation and structured tasks.
A Tale of Two Assessments: Telehealth vs. In-Person Autism Diagnosis
To test accuracy, Meltzoff and her team recruited 39 children seeking autism evaluations through a university-based clinic. Each child underwent two separate assessments — one in-person and one via telehealth — conducted by different clinical teams who were unaware of each other’s conclusions.
The results were promising. One of the tools developed for children whose speech is limited to short phrases showed particularly high accuracy, while another designed for more verbally fluent children was effective in many cases but less consistent.
The study also found that parents were largely satisfied with telehealth assessments, suggesting the approach is both feasible and acceptable for families.
The need for alternatives to in-person diagnosis is significant, Meltzoff said.
“A lot of people live two hours from an autism clinic,” she said. “Getting your kid two hours to a clinic, then doing an appointment and two hours home just isn’t really feasible.”
The approach is especially important for families in rural areas or those with limited financial resources. For some, transportation costs or lack of access to reliable transit can make in-person visits difficult.
Speech Therapy, Occupational Therapy, and Behavioral Therapy: Supporting Child Development in Autism
Additionally, a formal autism diagnosis is often required to access essential services. While schools can provide some support without a clinical diagnosis, insurance coverage for therapies typically depends on one. Those services include speech therapy, occupational therapy, and one-on-one behavioral interventions — all of which can be critical for helping children develop communication and life skills.
Still, Meltzoff cautions that telehealth is not a one-size-fits-all solution. Children with more subtle symptoms or co-occurring conditions such as attention deficit and hyperactivity disorder (ADHD) may still require in-person evaluations for accurate diagnosis.
“I don’t want to oversell it,” Meltzoff said. “It worked for most kids, but more complex cases — the ones that are already difficult even when done in-person — can be harder to evaluate remotely.”
Even with those limitations, the study validates new tools for children with a wider range of communication abilities.
“How accurate is telehealth?” Meltzoff asked rhetorically. “We found it’s pretty good.”
::ANNOUNCEMENTS::
TSI Executive Committee Election Result
The Telemedicine Society of India (TSI) conducted elections for the vacant post of Executive Committee Member for the term 2025–2027. As only one valid nomination was received, Dr. Amit Aggarwal (LM0338) was elected unopposed as Executive Committee Member.
The election process was conducted under the supervision of Dr. Murthy Remilla, President-Elect & Returning Officer, TSI.
New Life Members Joined – April & May 2026
TSI is pleased to welcome the following new Life Members who joined during April and May 2026:
Dr. Gopal Shah (Gujarat) Dr. Nikhil Mehta (Chandigarh) Dr. Parmar Kinjal Jashubhai (Gujarat) Dr. Hetal Vadiwala (Gujarat) Dr. Jagdish Sakhiya (Gujarat) Dr. Subash Chandra Sarangi (Odisha) Prof. Shabir A. Sofi (Jammu & Kashmir) Dr. Subrata Kumar Datt (Karnataka)
New Paramedic Members Joined – April 2026
TSI warmly welcomes the following new Paramedic Members who joined in April 2026:
Mr. Sharvan Kumar (Punjab) and Mr. Ramandeep Singh (Punjab).
TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Telemedicine Society of India
What is New?
The Odisha Chapter of TSI held its annual conference in Puri this month, and as President, I had the privilege of attending. It was inspiring to witness the energy and passion that Dr. B. N. Mohanty brings to the chapter. Under his leadership, a strong pipeline of future leaders is being nurtured-individuals who will undoubtedly carry the torch forward.
I observed a similar spirit of enthusiasm in Ahmedabad last month, particularly around digital health initiatives. These experiences reinforce the strength and potential that exists across our chapters.
As a central body, we must find ways to bring these champions together at the national level and actively engage them in our broader initiatives. This remains a challenge-one that perhaps deserves a dedicated discussion with stalwarts from different chapters. Jaipur could be an ideal setting for such a conversation.
This issue brings together a selection of articles on digital health, reflecting the growing momentum in this space. We have also included a brief report about the inauguration of West Bengal Chapter by our President Elect Dr.Murthy and from the Telangana chapter, highlighting their recent activities and contributions.
Thank You Dr. Sunil Shroff Chief Editor President, TSI
Dr. Google Is Out and Dr. AI Is In: The New Patient Journey
Dr. Sunil Shroff President, Telemedicine Society of India | Consultant Urologist & Transplant Surgeon
A recent report from West Health–Gallup (2026) study showed the rapidly changing patient behaviour when it comes to consulting technology platforms before visiting a doctor. The Gallup showed that 1 in 4 Americans—about 66 million people—now use AI tools for health advice, often before or after seeing a doctor, and sometimes instead of one.
This marks a decisive shift: patients are no longer just searching for information—they are consulting AI.
The New Patient Journey
The traditional pathway:
Symptom → Doctor
is rapidly becoming:
Symptom → (Dr.Google – previously) → Now – Dr.AI → Doctor →Dr.AI → Decision
59% use AI before a consultation
56% use it after
14% have skipped a doctor visit based on AI advice
AI is now the first touchpoint in healthcare.
What’s Changing in Patient Behaviour?
Patients today arrive:
More informed—with possible diagnoses and treatment options
More confident—46% say AI helps them engage better with doctors
More selective—weighing whether a visit is needed at all
But this confidence is not always accurate. Trust in AI remains mixed, and concerns about unsafe advice persist.
Where Does This Leave “Dr. Me”?
The doctor’s role is not diminishing—but it is transforming:
From information provider → interpreter of AI insights
From authority → collaborator with informed patients
From gatekeeper → guide ensuring safe, contextual care
In a world where answers are abundant, clinical judgment and trust become the true differentiators.
What About Hospital Visits?
AI is quietly reshaping healthcare utilization:
Potential reduction in minor, low-acuity visits
More complex consultations with pre-informed patients
Risk of delayed care when AI replaces timely medical advice
The “front door” of healthcare is no longer the clinic—it is increasingly digital and AI-driven.
The Takeaway
The rise of Dr. AI is not a threat—it is a signal.
A signal that:
Patients want faster, accessible, and understandable care
Healthcare systems must adapt to a new first point of contact
Doctors must evolve from being the first source of information to the most trusted source of truth
Final Word
The future is not Doctor vs AI.
It is:
Doctor + AI + Patient
And in that equation, the success of Dr. Me will depend on one thing:
Staying the most trusted voice in an AI-first world.
(This article is summary of the article – After Dr. Google, It Is Dr. AI — Where Does It Leave Dr. Me? from www.medindia.net by the same author)
Digital Health Conferences: Trials & Tribulations
Dr. K. Ganapathy Hon Distinguished Professor IIM Jammu Distinguished Professor, The Tamilnadu Dr MGR Medical University Emeritus Professor, National Academy of Medical Sciences Formerly Distinguished Visiting Professor IIT Kanpur Past President, Telemedicine Society & Neurological Society of India Formerly WHO Digital Health expert
“In our rush to build shovels, we should know what we are digging for”
I started attending neurosurgical conferences from 1975. Over the last 28 years, was actively involved in organising conferences and for many years was the Principal Organising Secretary – but that was for neurosurgical conferences in the BC era. In the last 15 years have also helped draw up the scientific program for a major International Digital Health conference. Though a staunch advocate of “TELE”, even in the virtual AI enabled universe, physically listening to experienced speakers, visiting trade exhibitions and just meeting like-minded friends and colleagues, goes a long way in augmenting every one’s personal growth and development.
Nevertheless, can a hard-core clinician of yesteryears, advise future ready, gizmo making healthineers, particularly when the RoI expected in speaking and attending Digital Health conferences, is quite different. Excellence is a moving target. The bar needs to be raised every year. Attendees increase, if quality and quantity of presentations increase, in breadth and depth, for the beginner and for the expert. Starters, main course, dessert, a focused menu offering an intellectual repast – 20 hours of unadulterated wisdom – easier said than done! One must accept that in the real world “All are equal, but some are more equal”
Today, in any conference dealing with any aspect of healthcare, AI must be used, as a suffix and prefix. Hyperboles and embellishments are necessary marketing tools. Doctors are told to lead the AI transformation, before patients start demanding and even using it! Challenges in organising a Digital Health conference cluster around governance, scientific program design, logistics and stakeholder management. Balancing “digital health for clinicians” vs health-IT, start-ups, MedTech, policy and investors in one single event, risks a fuzzy value proposition. Tracks and audiences need to be clearly segmented. This requires a strong local organising committee, scientific committee and exhibition/trade committee. While implicit trust in a professional conference organiser is essential there must be a fine balance between delegation and micromanagement.
Raising adequate funds in time is a gargantuan task. Late sponsorship confirmations and slower registrations can produce cash-flow stress. Managing industry sponsorship in line with ethics can constrain how sponsors are acknowledged and given prime stage time. Differentiating between “whose bread you eat, his song you must sing” and a globally renowned domain expert an academician par excellence, is not simple. Having parallel sessions presupposes having adequate capacity multiple halls. How does one ensure equitable audience distribution. No speaker wants to be the first speaker or last speaker or immediately after lunch. The organising secretary must factor in distance from the airport, traffic jams, unexpected bandhs and of course snowstorms in different parts of the world. It is expected that the chief of staff of global MNC CEO’s have ensured that their bosses have valid visas. It is amazing how the PMO holds emergency meetings at exactly the time when a Secretary to the Govt of India has agreed for a keynote address. Every session should have a specific theme and all talks covering a theme should be in that session. However, it is astonishing that some speakers in that session have flights to catch at that time . Having a pot pourri of unrelated topics in one session, to accommodate such speakers, raises eyebrows! With 65 speakers, not sure if Perplexity or ChatGPT 5.1 could give correct weightage to the scores of unpredictable variables and produce a conference to satisfy most of the attendees and speakers from a diversified background, with different expectations !
To add to the complexities, VVIP’s only confirm their participation hours before they are expected, even though the invitation was extended a year earlier. As they do not decline, alternative arrangements cannot be made. No VVIP likes to be in the 12th Man / RAC category . Hence there can be no back up plan! Murphy’s law ( if a thing can go wrong it usually will ) is particularly applicable to airport transfers and hotel checking. Delegates do not reply to multiple reminders of early check in and late check out requirements and fume and fret for the 300 seconds waiting time.
Wi-Fi, app based programmes, QR check-in, CME credits , catering to wide culinary tastes covering gluten and peanut allergy and special needs are in 2026, the basic expectations. Exhibitors expect footfall, speaking slots, lead capture support, and visible branding. Registration management should include spell checks, accurate attendee lists, handling payments, GST invoices and on-site badge printing. Recruiting and training enough volunteers for hall management, speaker support, and delegate help desks is essential. Despite all this a passionate dedicated group of NI enabled humans can still do wonders and organise successful Digital Health conferences .
Report of 14th Annual Conference of The Telemedicine Society of India (TSI), Odisha Chapter (Oditelemedicon 2026) held on 18.04.2026 at Puri, Odisha.
Dr.Biswajit Samal Hony.Secretary, TSI Odisha Chapter
The 14th annual conference of The Telemedicine Society of India (TSI), Odisha Chapter (Oditelemedicon 2026) was organized by TSI, Odisha Chapter in association with District Health Administration, Puri as a hybrid event on 18th April 2026. The venue for the conference was District Training Unit-II, Dist.Hqrs.Hospital, Puri. The theme of the conference was “Telemedicine powered by modern digital technologies poised to revolutionize healthcare delivery”. A total number of 112 participants from various districts of Odisha physically attended the conference. 11 TSI members attended the conference over virtual platform.
The conference was inaugurated by Dr.Sunil Shroff, President of Telemedicine Society of India. Dr. Akshay Kumar Satpathy, CDM&PHO, Puri attended the inaugural function as guest of honour. Dr. B Nageswar Rao Subudhi, president of TSI, Odisha Chapter presided over the function. Annual Report of the chapter was presented by Odisha Chapter secretary Dr. Biswajit Samal.Chief coordinator of the conference Dr.Biswa N Mohanty delivered welcome address.
The 1st session was held on ‘Digital Solutions to meet healthcare needs’. The speakers in this session were Rashmita Samal,Senior Programs Manager, Intelehealth, Bhubaneswar; Dr.Sunil Shroff,President of Telemedicine Society of India and Mr.Sameer Sawarkar, Co-Founder and CEO, Neurosynaptic Communications Pvt. Ltd. Bangalore. Rashmita Samal delivered a talk on ‘The eSanjeevani Ayushman Arogya Mandir Platform in Odisha with support from Intelehealth- an enabler of universal access to quality healthcare services’. Dr.Shroff talked on ‘AI Innovation versus Data Protection: finding the balance in healthcare’.Sameer Sawarkar spoke on ‘Expanding access to primary care in rural and underserved areas of Odisha through its ReMeDi® technology’.
The 2nd session was held on ‘Innovations and changing clinical practice’. The speakers in this session were Dr. R Kim, Chief Medical Officer & Senior Consultant, Vitreo-Retinal Services,Aravind Eye Hospital & Postgraduate Institute of Ophthalmology, Madurai;Dr.Bidyut Kumar Das,Professor of Clinical Immunology & Rheumatology, SCB Medical College, Cuttack;Dr.Rakesh Kumar Routray, Assistant Professor of Nephrology, SCB Medical College, Cuttack and Dr.Sabyasachi Pattanaik, senior Ophthalmology specialist,Bhubaneswar.Dr.Kim delivered a talk on “Changing dimensions in the practice of Tele-Ophthalmology in India”, Dr.B K Das talked on “Impact of Rheumatology tele-care on rural population in Odisha”,Dr.Routray spoke on “Reaching the unreached : Telenephrology in Rural and Remote care” and Dr.Pattanaik talked on “Telemedicine enabled vision center for universal eye care”.
A panel discussion was held on the theme “Changing face of telemedicine and digital health for effective delivery of patient-centric care” at 2.15pm moderated by Dr.Biswa N Mohanty, Dr.Srikanta Patnaik and Mr.Sujan Kumar Mohanty. The speakers were Dr. Arun Kumar Choudhury,former professor & head, Burns and Plastic Surgery Department, SCB Medical College, Cuttack; Dr.Rajamenakshi R, scientist-F,HPC-Medical & BioInformatics applications Group from CDAC,Pune; Dr.Vivek Tiwari, Assistant Professor, Department of Biological Sciences,IISER,Berhampur and Mr.Ashwin Desai,Managing Director, A & T Video Networks Pvt. Ltd, Madurai. Dr.Choudhury addressed the issue of ‘combining in-person care and virtual care for delivery of appropriate health care’; Dr.Rajamenakshi R, Pune addressed the issue of ‘addressable cybersecurity threats for secure data sharing’;Dr.Vivek Tiwari of Berhampur discussed on ‘Generative AI for clinical augmentation’ and Mr.Ashwin Desai from Madurai addressed the issue of ‘New initiatives in patient-centric telecare’.
The chair persons for different sessions were Dr.Ramnath Misra,past-president of TSI Odisha Chapter from Bhubaneswar, Dr. I B Kar, past-president, TSI Odisha Chapter from Cuttack; Dr.B Nageswar Rao Subudhi,president of odisha chapter from Berhampur, Dr.Bijay Kumar Mohapatra past-president of TSI Odisha Chapter from Bhubaneswar and Dr.Manoranjan Patnaik past-president of TSI Odisha Chapter from Cuttack.
In-charge medical officers from CHCs and Community Health Officers from various Govt. health institutions of Puri District; IMA members of Puri branch; Teachers of SJ Medical College & Hospital Puri; Medical Officers of Puri Dist.Hqrs. Hospital, TSI members and health administrators working under Odisha Govt., telemedicine technical personnel from several telemedicine nodes of Odisha attended the conference. Some members of TSI including past-presidents, current executive committee members and other invited guests participated in the program over virtual platform from different locations.
The Annual General Body Meeting of the TSI, Odisha Chapter was held at the same venue at 1.00pm on 18.04.2026. The following life members of TSI were elected as office bearers of the Odisha state chapter for the term 2026-27.
President: Dr. Arun Kumar Mohanty, Cuttack Immediate Past-President: Dr. B Nageswar Rao Subudhi, Berhampur President-elect: Dr. Arun Kumar Choudhury, Cuttack Vice-President: Dr. Sabyasachi Patnaik, Rourkela Secretary: Dr. Biswajit Samal , Angul Jt. Secretary: Dr.Pranab Sankar Dash, Baripada Treasurer: Dr. Sarat Kumar Nayak, Cuttack Executive Members : Dr. Bidyut Kumar Das,Cuttack & Dr. Sribatsa Kumar Mohapatra, Burla
The valedictory function was held at 3.30pm. Newly elected president Dr. Arun Kumar Mohanty was installed during the valedictory function. After installation the incoming president spoke about his plan of action for the coming year. The District Health Administration of Puri District represented by CDM & PHO, Puri was felicitated by President of TSI, Odisha chapter. Coordinator of the conference Dr. Sibananda Mohanty thanked profusely the district health administration of Puri for its overwhelming support to organize the conference. He also thanked all the invited speakers. In the valedictory function, participants from CHCs and sub-centers highly appreciated the TSI, Odisha Chapter for the useful discussions held during the conference which helped them immensely in enhancing their understanding of digital health applications.
Inaugural Ceremony of Oditelemedicon 2026
Dr. Sunil Shroff delivering his talk
Community Health Officers from Sub-centers of Puri District
Strategic Roadmap for AI-Enabled Telemedicine: A Report on the Milestone Event of TSI West Bengal Chapter Inauguration
Dr. Murthy Remilla President-Elect, Telemedicine Society of India
(with iputs from honorable members of WB and Rappeuterts of Groups) On March 21, 2026, I had the privilege of witnessing a landmark event in the evolution of digital health in India: the formal inauguration of the 21st State Chapter of the Telemedicine Society of India (TSI) in West Bengal. The day was characterized by a spirit of innovation, most notably through the implementation of a structured program designed to move from ceremonial opening to immediate clinical and policy action with active involvement of memebrs and prospective-members of particpants in the function.
Program Plan and Structure
The event was meticulously organized to facilitate high-level networking, formalize leadership, and engage experts in intensive problem-solving.
I. Commencement and Formalities
Registration and Networking: Led by Hony Secretary Subir Ghosh and Executive Member Madhurima Roy, the session provided 49 delegates with essential seminar materials, including agendas, notepads, and pens.
Traditional Welcome: Reflecting regional culture, the Chief Guest and participants were welcomed with traditional Khadas from the hills by the President, Dr. Pankaj Chowdhary.
Inaugural Addresses and Welcome Speech: Prof. Supten, President-Elect of the TSI WB Chapter, facilitated the reception of national leadership and special invitees.
Introduction: Subir Ghosh formally introduced the Chief Guest and diverse group of guests and participants to the house.
Official Launch: Dr. Pankaj Chowdhary, President of the TSI WB Chapter, and Dr. Murthy Remilla, President-Elect, Telemedicine Society of India performed the traditional inauguration and declared the chapter open to takeup the objectives for TSI in Eastern India.
Adress By Chief Guest: Dr. Murthy Remilla President-elect, TSI coveyed the message of greetings from President & EC of TSI to new chapter of WB and conevyed best wishes of the entire community of TSI members all across India in wleocming the newly formed West Bengal Chapter onbaord. Dr. Murthy briefed aboy the initiation if TM services in India with support of ISRO and the evolution and growth of TM in india including the formal formation of TSI and theregistarion. He also explained the efforts towards the issue of Telemedicine practivce Guidelines (TMPG) and the efforts by all stakeholders of TSI, setting the background and tone for the group discussions on opportunities and challenges to embrace the AI technology into Telemedicine.
II. The Round Table Framework
The structural centerpiece was the Round Table Discussions, an innovative format introduced by Dr. Pankaj and Dr. Supten probbaly first time in the histrory of any state chapter inaguration of TSI state chapter.
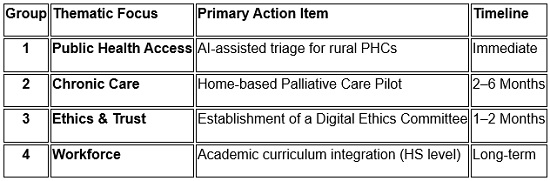
Discussions were arrnaged into 4 groups on 4 themes- Introduced by Dr Pankaj. Participants were divided into four specialized groups, each assigned a moderator and a rapporteur to guide 30 minutes of intensive discussion followed by a 3-minute presentation of conclusions.
Detailed Group Outcomes and Resolutions
Group 1: AI-Enabled Telemedicine for Bridging Healthcare Access Gaps
Moderator: Dr. Saptarshi Ghosh (Med. Supt., KPC Medical College)
Rapporteur: Dr. Sudeshna
Core Discussion: The group addressed how healthcare inequity in North Bengal and the Northeast is exacerbated by terrain, infrastructure, and specialist shortages.
Key Outcomes:
Intelligent Triage: Proposed AI systems capable of early symptom assessment and prioritizing cases to optimize medical resources.
Public Health Integration: Recommended embedding AI within national programs like Tuberculosis control (AI screening), Maternal Health (Tele-ANC), and NCD monitoring.
Digital Inclusion: Utilizing the Bangla Sahayata Kendra network to help citizens navigate digital platforms, with a focus on multilingual and voice-enabled AI.
Institutional Hubs: Using tertiary institutions like IPGMER and SSKM Hospital as hubs to provide specialist consultations to peripheral enters.
Group 2: AI in Continuum of Care – Chronic Disease, Oncology & Palliative Care
Moderator: Dr. Padmawati
Rapporteur: Dr. Pankaj
Core Discussion: This group focused on the short-term reality of long-term care, identifying a critical need for home-based support.
Key Outcomes:
Immediate Pilot Project: Resolved to launch a pilot program within 2–6 months focusing on the chronic disease continuum, specifically palliative care at home.
District Implementation: The pilot will run in one or two selected districts to evaluate real-world barriers.
Phased Scaling: A subsequent 6–12 month plan will address discovered shortcomings through new procedures and training programs.
Group 3: Ethics, Data Governance, and Trust in AI-Driven Telemedicine
Moderator: Dr. T. N. Sharma
Rapporteur: Dr. Supten Sarbadhikari
Core Discussion: Focused on the “Trust” factor, emphasizing that AI must be auditable, fair, and human-centric.
Key Outcomes (0–6 Month Roadmap):
Months 1-2: Establish a Digital Ethics Committee and define clear Data Stewardship roles.
Months 2-4: Implement “Privacy by Design,” data minimization, and consent management.
Months 4-6: Ensure regulatory alignment with DPDPA, HIPAA, and GDPR.
“Human-in-the-Loop”: Mandatory clinical validation and algorithmic audits.
Policy Deliverable: A formal “AI in Telehealth” Ethical Use Policy for State Government approval.
Group 4: Capacity Building and Future Workforce
Moderator: Dr. Biswajit Roy Chowdhury (SAIARD)
Rapporteur: Dr. Ritesh
Core Discussion: Identified the human and technical infrastructure needed to sustain a technology-ready workforce.
Key Outcomes:
Academic Integration: Recommended introducing Telemedicine courses into the High School (HS) level curriculum.
Clinician Adaptation: Encouraging senior doctors to adopt and adapt to new technologies.
Infrastructural Reform: Improving satellite communication for far-flung areas and linking Aadhar with UhlD Cards.
Policy Advocacy: Removing barriers between Central and State implementations and making the medico-legal system more flexible.
Executive Summary of Resolutions
Presentation of Mementos & Certification of appreciation by the Chief Guest:
The day concluded with an open floor interaction led by Dr. Kamal Roy and Dr. T.N. Sharma, followed by the presentation of resolutions by Dr. Sudeshna and Dr. Padmawati. We have now officially formed the TSI West Bengal Telemedicine Working Group to turn these discussions into reality. Dr. Murthy Remilla President-Elect, Telemedicine Society of India requetsed non-memebrs of the participants to become Life Members/Student Members of TSI and again appreciated the members who have worked towards the formation of the state chapter. The function conculded with a formal vote of thanks and a group photo.
News from TSI Telangana
Dr. Krishna Rao
Wednesday, the 8th April 2026.
Maheshwara Medical College and Hospital, in association with the Telemedicine Society of India, Telangana Chapter, has initiated the Knowledge Series 2026 to bring global experts onto a common platform to share their personal and professional journeys, along with insights into technological transformations in the healthcare industry. The series not only promotes knowledge sharing but also exposes medical students to diverse platforms and verticals, encouraging them to look beyond conventional boundaries and ensuring that their education extends beyond domain-specific expertise.
As part of this initiative, the institution invited Shri Day Veerlapati, a US-based NRI, who inspired students with the spirit of innovation and entrepreneurship. He spoke about the impact of telemedicine in connecting rural communities, highlighted challenges related to international travel especially to the United States and emphasised the importance of the Triple E’s: Education, Entrepreneurship, and Enlightenment. He also encouraged meditation, self-inquiry through the question “Who am I?”, and a proactive approach towards startups. Shri Dev is an IIT Kharagpur alumnus and Founder of S2 Tech, he further stressed the value of joining platforms like Toastmasters to enhance communication skills and cultivate an entrepreneurial mindset.
The session was moderated by Shri D. Chakrapani, Retired IAS officer and Academic Advisor to Maheshwara, whose practical insights greatly enriched the discussions. The Knowledge Series 2026 has been widely appreciated for nurturing critical thinking and shaping future ready medical professionals. Maheshwara Medical College and Hospital continues to lead in integrating education with innovation, setting benchmarks in telemedicine driven learning and emerging as a dynamic platform in today’s evolving healthcare landscape.
15th April 2026, Wednesday
As part of the Knowledge Series initiative, organized in collaboration between Telemedicine Society of India (TSI) and Maheshwara Medical College and Hospital, an insightful academic session was conducted for medical students and faculty, focusing on critical and often overlooked aspects of women’s health and social wellbeing.
The session was led by Dr. Samavedam Venkata Kameswari, a senior gynaecologist and research scientist, along with Dr. Prakash Vinjamuri, who together addressed a wide spectrum of issues including women’s health in rural settings, the growing concern of unwarranted escalation of surgical interventions, and the socio-cultural challenges faced by women in villages.
Dr. Kameswari passionately emphasized her visionary campaign, “Save Uterus – Our First Home,” highlighting the urgent need to prevent unnecessary hysterectomies through awareness, ethical medical practices, and early interventions. She also underscored the importance of emotional and social support for women within families, reinforcing her powerful message: “If the woman at home is healthy and happy, the entire family thrives.”
The session was highly interactive and deeply impactful. Students and faculty actively engaged with the speakers, raising thoughtful questions and showing keen interest in the subject. Inspired by the vision and commitment of Dr. Kameswari, the students expressed their willingness to contribute to the campaign and have joined hands to promote the message of “Save Uterus – Our First Home” across villages in Medak.
This initiative marks a meaningful step toward integrating academic learning with community service, empowering future medical professionals to advocate for ethical healthcare practices and the holistic wellbeing of women in society.
17th April 2026, Friday
A Mega Medical Camp at Bonthapally village in Jinnaram Mandal of Sangareddy district, Hyderabad
A two-day mega medical camp was successfully conducted at Bonthapally village in Jinnaram Mandal of Sangareddy district on April 17th, 2026, bringing together technology-driven healthcare and community outreach. The initiative was organized under the Telangana Chapter of the Telemedicine Society of India (TSI) as part of its healthcare services aimed at extending telemedicine services and also improving access to quality healthcare in rural areas. The camp was a collaborative effort between Rejuvin Medicare technical partner, Maheshwara Medical College & Hospital – medical services partner, and Gidde Raju Charitable Trust, which provided logistical support.
The camp stood out for its use of advanced diagnostic technology, enabling patients to receive real-time, color-coded medical reports for better understanding of their health conditions. This innovation helped bring clarity to several cases, particularly in differentiating gastric issues from cardiac complaints, thereby reducing unnecessary anxiety and interventions. A team of doctors, nurses, and paramedical staff from Maheshwara Medical College provided comprehensive services including cardiology screening, diabetes testing, ENT and eye check-ups, orthopaedic evaluations, gynaecological consultations, and general health assessments through Rijuven Clinic in a Bag portable investigative kit. Free medicines were also distributed to patients in need by Maheshwara.
The initiative received an overwhelming response from the local community, who appreciated the camp not merely as a one-time medical service but as an awareness-driven approach to preventive healthcare and rational use of medicines. Encouraged by its impact, village representatives and Panchayat members have expressed interest in establishing a long-term collaboration through a formal MoU to transform Bonthapally into a model village for digital healthcare. The organizers have responded positively, signaling the potential for sustained telemedicine-driven healthcare services in the region.
When Patient Data Disappear: Ghana’s Warning to Global Healthcare Systems
A recent correspondence in The Lancet Digital Health highlights a major digital health crisis in Ghana, where clinicians abruptly lost access to electronic patient records after a contractual dispute with a foreign technology vendor. The shutdown disrupted care, delayed treatments, and compromised clinical decision-making.
The authors warn that this incident underscores a global vulnerability in healthcare digitization: when patient data are controlled by external commercial providers—especially when stored outside national borders—health systems risk losing access due to contractual, corporate, or geopolitical conflicts.
Ghana has since migrated to a national system, but the damage persists, with clinicians forced to re-enter incomplete records and manage patient safety risks. The report calls on policymakers and healthcare leaders worldwide to treat patient data as critical infrastructure, ensure sovereign control over health records, and strengthen safeguards around digital health governance.
Key Takeaway: Patient data are not merely digital files—they are lifelines. Healthcare systems must ensure secure, sovereign, and uninterrupted access to electronic health records.
TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Telemedicine Society of India
What is New?
The month of March has been marked by three important milestones for the Society.
The first was a webinar to discuss the requirements of the new Telemedicine Practice Guidelines (TPG), which are expected to supersede the original guidelines issued in March 2020 during the COVID-19 pandemic by the National Medical Commission (NMC). This 70-minute webinar was attended by the Director of the Ethics Committee, Mr. Abhijeet Chakraborty.
Following the discussions, it was decided to constitute a committee to redraft the TPG, incorporating relevant provisions from the Digital Personal Data Protection (DPDP) Act as applicable to healthcare, and to further elaborate on the role of AI in telemedicine practice. Key deliberations also included the need to move away from the distinction between first and follow-up consultations, revise and expand the medication lists, strengthen the role of caregivers in consultations, and more clearly define the standard of care within the guidelines.
The key event was the inaugural one-day conference of the Gujarat Chapter of TSI, held in Ahmedabad. The conference brought together experts and stakeholders, fostering meaningful dialogue and strengthening collaboration within the field. Dr.Rajrawal along with his team pulled off a stellar show.
These initiatives reflect the growing momentum of TSI and reaffirm its commitment to advancing its mission across diverse regions of the country.
In this issue, I have also addressed an emerging concern associated with the rapid adoption of AI in healthcare-“Shadow AI.” I encourage you to read the article and deepen your understanding of this important and evolving risk.
Thank You Dr. Sunil Shroff Chief Editor President, TSI
Transitioning to Digital Public Health
Dr. K. Ganapathy Hon Distinguished Professor IIM Jammu Distinguished Professor, The Tamilnadu Dr MGR Medical University Emeritus Professor, National Academy of Medical Sciences Formerly Distinguished Visiting Professor IIT Kanpur Past President, Telemedicine Society & Neurological Society of India Formerly WHO Digital Health expert
(This article was published in the March 2026 issue of Medical Buyer and is reprinted with-permission)
Surgery of the unborn and robotic telesurgery is thrilling but a digitally enabled Public Health medical doctor working with policy makers and civil servants can do greater wonders What does India need? Digital Public Health or helicopter ambulances & intra operative MRI?Digital Public Health can radically transform Healthcare. No longer do we leap frog – after all how far can a frog leap – we have already started pole vaulting!
It was in 1998 that I first encountered the term “Telemedicine”. At the peak of my neurosurgical career, I got bitten by the IT bug. I realised that as a neurosurgeon I could at best contribute to the care of several thousand individuals. However technology enabled remote health care could make distance meaningless and Geography History! The urban rural health divide then was striking. In 2015, in a now oft quoted publication I had shown that 935 million Indians lived in areas where there was not a single neurologist or neurosurgeon. In this milieu it has been amazing to see the phenomenal transitioning to DIGITAL PUBLIC HEALTH (DPH) an entity which does not exist even today in scores of countries.
Introduction to DPH
India is now regarded as a global leader in DPH, especially among LMIC. India influence strategies even in high‑income settings. India is distinctive not just for scale, but for using open, interoperable (DPI) Digital Public Infrastructure (ABDM, CoWIN, UPI, Aadhaar) as a health “railway” rather than a collection of isolated IT projects. India’s ABDM is explicitly framed as a DPI – open APIs, federated data, consent-driven exchange, and a unique health ID (ABHA) that can work across public and private providers. It cannot be denied that a strand of RNA acted as a Global CTO (Chief Transformation Officer). Ensuring vaccination 2 billion times seamlessly making available digital certificates, demonstrated that India no longer leap frogs. We pole vault!
DPH Illustrations
Ayushman Bharath Digital Mission has a laudable goal of having an interoperable digital infrastructure for all health actors. This citizen-centric, consent‑based health data exchange could provide a digital documentation, never achieved. eSanjeevani the Govt of India Telemedicine platform is used about 400,000 times a day. 430 million teleconsultations have already been documented. As a guestimate probably 200,000 teleconsults occur daily using other platforms. 875 million ABHA numbers have been created. 350 million digital health records have been linked. 285,000 professionals and 400,000 institutions have been onboarded in ADHM. 5,000 + Real-time outbreak detections have been documented. Queue Time has been reduced from 35 minutes to 5-10 min in 75% of instances. Claim Processing became 85-90% faster- from 30 days to 4 days.
Success of DPH
Built on national DPI, Digital Health (DH) was treated as a public good, not a product. India has demonstrated that population‑scale DH platforms can be implemented at very low per‑capita cost, using cloud, open APIs, and a modular DPI stack. India built health on top of existing national rails: Aadhaar (ID), UPI (payments), Digi Locker (secure document storage), and India Stack APIs. ABDM was then added as a health‑specific DPI. Steps preceding the implementation of DPH is critical. Early foundational work (digital ID, payments, visible, high‑impact success eg. Cowin’s 2 billion doses, real‑time dashboards helped create political and public confidence which is vital. Prior investment in governance, change management, allocating specific budgets for digital infrastructure, workforce training and maintenance was as important as software and hardware.
Challenges and how they are addressed
These include large rural and older populations, reduced device access, urban-rural digital divide, digital illiteracy, variable connectivity, privacy, cybersecurity, interoperability governance in a rapidly scaling system, increasing workload for health workers and institutions and workflow disruption. Building DH systems on top of robust national DPI, addresses many issues. Attention to Change Management, designing explicitly for equity, assisted access, multilingual interfaces, offline capability and federated, consent‑based data sharing is essential. Collaborating with private sector and tech companies to co-develop, maintain, and scale digital solutions ensure sustainability and innovation. Designs for the majority, not just the digitally literate is essential as is ensuring interoperability with other sectors and Digital competency among health professionals.
Deployment of AI in DPH
The enormous backing, to deployment of AI in the private and surprisingly the public sector, in all areas of healthcare will soon yield tangible measurable dividends. In DPH, AI is being used in management of TB, vector‑borne diseases, maternal health, radiology and predictive analytics.
Conclusion
India aims for near‑universal DH coverage, with AI‑enabled predictive public health, integrated chronic disease management and digitally competent health workforces. Healthcare should not become digital care. Healthcare will no longer depend on where one lives, but how well one is digitally connected. Technology is a means to achieve an end, not an end by itself. A fool with a tool is still a fool!! Digital should be the foundation, so healthcare can focus on human dimensions that no algorithm can ever replace.
How ‘Shadow AI’ Can Endanger Healthcare Ecosystem
Dr. Sunil Shroff President, Telemedicine Society of India | Consultant Urologist & Transplant Surgeon
Artificial intelligence (AI) is making inroads across all domains of medicine
We are already seeing promising applications of AI such as:
Predictive models to identify high-risk patients and anticipate outcomes
Natural language models (NLMs) enabling conversational AI for emotional and psychological support
Administrative streamlining, reducing clinician burden and improving efficiency
Although the use of AI in medical specialties-is still evolving. There are important limitations and challenges that must be addressed, including data privacy, ethical concerns, and the need for robust validation studies.
I am particularly concerned about the current level of digital literacy among healthcare professionals. Increasingly, doctors and nurses are using tools like ChatGPT in their daily practice. The concern arises when patient information is entered into such platforms, as this data may be stored or used for training purposes. This creates a real risk of data leakage, breach of confidentiality, and violation of patient privacy.
What is Shadow AI?
Shadow AI refers to AI tools and models used inside a health system without formal approval, governance, or oversight. This can include consumer apps, chatbots, or vendor models that clinicians or staff adopt on their own. While convenient, Shadow AI poses real risks to patients, data privacy, and regulatory compliance.
Why this matters for you as a Clinician
1.Patient safety: Unvetted tools can give inaccurate or non-reproducible outputs, potentially affecting diagnoses or treatment plans. 2.Privacy and data security: Patient health information (PHI) may be uploaded to non-compliant tools, risking breaches or misuse. Data may be used to train external models without proper agreements.
3.Compliance gaps: Many AI tools fall under regulatory rules (HIPAA, FDA SaMD, GDPR). Shadow use can create blind spots with no audit trail.
4.Data quality and interoperability: Outputs may drift, be biased, or not integrate with EHRs, leading to inconsistent records.
What to do in daily practice 5.Use sanctioned tools only: Rely on the institution’s approved AI toolkit and guidelines. If unsure, pause and ask your supervisor or IT.*
6.Protect PHI: Do not upload or paste PHI into unapproved tools. Check data-sharing terms and ensure BAAs are in place before any use that involves PHI.
7.Validate and review: Treat AI outputs as decision-support. Always review against your clinical judgment, patient data, and local protocols before acting.
8.Documentation and audit trail: Record tool name, version, inputs, outputs, and how the result influenced care in the patient record where required.
9.Be transparent with patients: If AI assists care decisions, disclose its role when appropriate and be prepared to explain its role and limitations.
10.Security and privacy hygiene: Keep devices updated, use institution-approved networks, and report unusual data requests or tool behavior.
11.Report and escalate: If you encounter or suspect Shadow AI use, report to your supervisor, IT/privacy, or the AI governance contact. Do not ignore potential risks. 12. Check the AI app security: Switch off section for data sharing for training
13. Delete chats and initiate temporary or “non-retained” chats (including ChatGPT), and they are one of the key safeguards to reduce data exposure. But they are not a complete solution
Simple Safe Practice Rule which everyone can follow:
Turn off data sharing / training always
Use temporary chats where available
But NEVER enter identifiable patient data unless:
The tool is institution-approved
There is a formal data protection agreement
It is clinically validated and secure
Activating these safeguards should be the first step before using any AI tool more so if you are using it in a clinical context. We must also recognize that we are now governed by the Digital Personal Data Protection Act, under which penalties for violations can go up to ₹250 crore. Even a single high-profile breach could not only affect an individual clinician but also create widespread fear, potentially stifling innovation across the healthcare sector.
Bottom line Shadow AI can undermine patient safety and privacy if left unchecked. Use only approved tools, understand data handling, and engage governance processes.
AI holds tremendous promise-but it must be used responsibly and ethically. Let us embrace innovation, but not at the cost of patient safety, trust, and professional integrity.
TSI GUJCON 2026 Conference
DATE : 22/03/26, SUNDAY VENUE : ATAL-KALAM BHAVAN, GUSEC
TSI GUJCON 2026 conference, focussed on the strategic, legal, and technological evolution of telemedicine in India.
Inaugural Session: Strategic Vision and History
ISRO’s Role: Dr. Nilesh Desai (Director, SAC-ISRO) highlighted ISRO’s 25-year legacy in telemedicine, including a recent MOU with Integrated Defense Services. He introduced future technologies like “Satcom on the Move” (mobile telemedicine nodes) and Quantum Key Distribution (QKD) to secure medical and financial data.
Digital Health Vision: Dr. Sunil Shroff (President, TSI) emphasized that technology is now a primary care driver, moving toward precision medicine while cautioning that the “human touch” must remain central.
Ecosystem Growth: Dr. Shrinivas Rao (CEO, GUSEC) discussed the “telemedicine revolution” and GUSEC’s role in incubating med-tech startups to reach inaccessible regions.
Session 1: Implementation Challenges in India
Panel Discussion: Moderated by Dr. Vivek Dave, the panel addressed infrastructure and digital literacy gaps in rural India.
Key Takeaways:
The Telemedicine Practice Guidelines (TPG) 2020 provided the essential legal framework that protected both patients and doctors during the pandemic.
Panelists discussed “website manners” to improve patient empathy during video calls, such as looking at the camera rather than the screen.
The Hub and Spoke model was identified as the most effective rural delivery method.
Session 2: Ayushman Bharat Digital Mission (ABDM)
Building Blocks: Dr. Vatsrajani detailed the implementation of the ABHA (Ayushman Bharat Health Account), which allows for consent-based, paperless health record sharing.
Professional Registries: The session urged all doctors to register on the Healthcare Professional Registry (HPR) and Health Facility Registry (HFR) to integrate into the national digital backbone.
Incentives: The government is offering digital health incentive schemes (DHIS) to hospitals to encourage the linkage of digital health records.
Session 3: Digital Health Law, Ethics, and Responsible Innovation
TPG Compliance: Dr. Sunil Shroff provided a deep dive into the TPG 2020, clarifying that telemedicine is an enabler, not a replacement, for traditional care.
Record Preservation: Records must be kept for 3 years (10 years for medico-legal cases).
Shadow AI: A critical warning was issued regarding “Shadow AI”—the unauthorized use of public AI tools (like ChatGPT) with sensitive patient data, which can lead to severe privacy breaches and massive legal fines under the DPDP Act.
Session 4: Data Privacy and Cyber Security
Threat Landscape: Mr. Dhaval Davesar highlighted the CIA Triad (Confidentiality, Integrity, Availability) and the rising threat of ransomware in healthcare, citing the KD Hospital attack as a case study.
Security Protocols: The session covered vulnerabilities in IoT medical devices (e.g., infusion pumps) and recommended regular security audits and avoiding public Wi-Fi for clinical work.
Session 5: Deep Dive into Tele-Medicine Practice Guidelines
Regulatory Framework: Dr. Krishna Kumar clarified that TPG remains legally valid under the NMC Act 2019.
Consultation Categories: Detailed the requirements for “First Consult” versus “Follow-up Consult” and the strict categorization of drugs (Lists O, A, B, and Prohibited) that can be prescribed remotely.
Session 6: Tele-Robotics and Future Surgery
Milestone Achievement: Dr. Sanjiv Haribhakti presented the first tele-robotic surgery in Gujarat, performed on a patient in Ahmedabad while he was in Delhi.
SSI Mantra: The use of the indigenous SSI Mantra robot, which is CDSCO-approved for tele-surgery, was highlighted as India leading the world in this field.
Technical Needs: Successful tele-surgery requires a latency of less than 200 milliseconds to ensure the surgeon does not feel a lag.
Session 7: ISRO’s Continuing Medical Education (CME)
Educational Outreach: ISRO has conducted 109 CME sessions since 2012, reaching over 20,000 healthcare professionals, particularly those in remote defense outposts like the Siachen Glacier.
Space Medicine: Future ISRO projects will focus on Space Medicine, researching how microgravity affects molecule binding for new drugs and crop cultivation for long-term space missions.
Session 8: Startups and Mobile Innovations
Patient-Centric Shifts: The move from “hospital-centric” to “mobile-first” care was discussed, with mobile apps acting as the fulcrum for real-time monitoring.
Innovative Prototypes:
RespiGO: A portable capnography device for real-time CO2 monitoring.
Locomotion: A wearable sensor for clinical gate analysis.
D3S Healthcare: The “VR Skin Scan Light,” a portable red-light technology for early-stage breast cancer screening
Strategic Vision and ISRO’s Legacy
The conference highlighted ISRO’s 25-year history in pioneering telemedicine, which began with connecting super-speciality hospitals to remote areas using satellite technology. A recent milestone is the MOU with Integrated Defence Services (IDS) to provide medical services to strategic forces and their families in remote regions. Future technological frontiers include “Satcom on the Move” (mobile telemedicine nodes) to reach multiple villages and Quantum Key Distribution (QKD) to secure medical and financial data.
Implementation and the Digital Backbone
The shift from “hospital-centric” to “mobile-first” care was a central theme, with mobile apps acting as the primary point for real-time patient monitoring. The Ayushman Bharat Digital Mission (ABDM) is building the national digital infrastructure through several key components:
ABHA (Ayushman Bharat Health Account): Enables paperless, consent-based sharing of longitudinal health records.
Registries (HPR/HFR): Doctors and facilities must register on the Healthcare Professional Registry and Health Facility Registry to integrate into the national ecosystem.
Incentives: The Digital Health Incentive Scheme (DHIS) offers hospitals financial rewards (up to ₹5 crore) for linking digital health records.
Legal Framework and Professional Standards
The Telemedicine Practice Guidelines (TPG) 2020 remain the essential legal framework, validated under the NMC Act 2019.
Consultation Standards: Guidelines define “First Consult” versus “Follow-up Consult” and strictly categorise drugs (Lists O, A, B, and Prohibited) for remote prescription.
Record Preservation: Records must be maintained for 3 years, or 10 years for medico-legal cases.
Professionalism: Panelists emphasized “website manners,” such as maintaining eye contact with the camera to preserve patient empathy during video calls.
Data Privacy and Cyber Security
With the rise of digital health, security has become paramount, guided by the CIA Triad (Confidentiality, Integrity, and Availability).
Ransomware: Healthcare is a major target, as seen in the KD Hospital case study; hackers often use extortion by threatening to release data on the dark web.
Shadow AI: A critical warning was issued regarding the unauthorized use of public AI tools (like ChatGPT) with sensitive patient data, which can lead to severe privacy breaches and massive legal fines under the DPDP Act.
IoT Vulnerabilities: Medical devices like infusion pumps are increasingly susceptible to attacks, requiring regular security audits and avoiding public Wi-Fi.
Technological Frontiers: Tele-Robotics and Space Medicine
India is leading the world in tele-robotic surgery using the indigenous, CDSCO-approved SSI Mantra robot.
Milestone Surgery: The first tele-robotic surgery in Gujarat was performed on a patient in Ahmedabad by a surgeon located in Delhi.
Technical Requirements: Successful tele-surgery requires a latency of less than 200 milliseconds to prevent lag during procedures.
Space Medicine: ISRO is researching how microgravity affects molecule binding for new drugs and crop cultivation for long-term space missions.
Innovation and Startups
GUSEC is actively incubating med-tech startups to address rural healthcare gaps. Featured prototypes include:
RespiGO: A portable capnography device for CO2 monitoring.
Locomotion: A wearable sensor for clinical gate analysis.
D3S Healthcare: The “VR Skin Scan Light” for early-stage breast cancer screening.
Telemedicine Society of India Webinar Report
Celebrating Women, Advancing Health, Transforming Care
Commemorating International Women’s Day & World Kidney Day | 12th March 2026
Compiled by Ms. Neeraj Chaudhary
Introduction
The Telemedicine Society of India proudly hosted a special webinar commemorating International Women’s Day and World Kidney Day on 12th March 2026 a powerful convergence two important day celebrated across the globe.
This unique platform brought together distinguished women leaders from healthcare, public service, academia, and digital health to share insights, experiences, and innovations shaping the future of care. The discussions highlighted the intersection of gender, technology, and health equity, emphasizing how telemedicine is not only expanding access but also empowering women as both providers and beneficiaries of healthcare. The webinar stood as a testament to the growing leadership of women in shaping a more inclusive, accessible, and technology-enabled healthcare ecosystem.
Telehealth as a Tool for Women’s Empowerment
Dr. Uma Nambiar beautifully described telehealth as a “silent transformation”-one that is steadily changing women’s lives without always being visible. She spoke about how, despite growing conversations around gender equality, there is still a long way to go in achieving real, everyday equity.
Telemedicine, she explained, is helping bridge that gap. For women doctors, it offers the safety and comfort of consulting from home, reducing the stress of travel and long working hours. For many women who had to pause their careers due to family responsibilities, it opens a door to return, rebuild, and rediscover their professional identity.
For women as patients, the impact is equally powerful. In many homes, women’s health often takes a backseat. Teleconsultations allow them to seek care privately, conveniently, and without depending on others. Dr. Nambiar also highlighted how more women are stepping into leadership roles in digital health, driven by empathy and a strong sense of community.
Her message was simple yet powerful-telemedicine is not just technology; it is a quiet force for social change.
Session on Chronic Kidney Disease
In a very insightful session, Dr. Haritha Karuparti spoke about how digital health is improving the way we understand and manage Chronic Kidney Disease and Acute Kidney Injury.
She explained the vital role our kidneys play in maintaining balance in the body—from managing fluids to regulating blood pressure—and how early detection can make a life-saving difference. With tools like Electronic Medical Records, doctors can now identify risks earlier and act faster.
She also pointed out the importance of being cautious with commonly used medications like Nonsteroidal anti-inflammatory drugs, which can sometimes harm kidney function if not monitored properly. Technology, through smart alerts and monitoring systems, is helping doctors stay one step ahead.
What stood out in her talk was the emphasis on awareness—because informed patients and proactive care can truly change outcomes.
Leadership, Safety, and Women Empowerment
Dr. Anshu Singla delivered a deeply motivating talk that resonated far beyond the field of healthcare. Drawing from her journey as both a doctor and an IPS officer, she shared simple yet powerful life principles that can guide anyone.
She spoke about the importance of financial independence-not just as a goal, but as a foundation for confidence and freedom. She encouraged regular self-reflection, building meaningful relationships, and stepping out into the world to gain new perspectives through travel and exposure.
Her thoughts on setting personal boundaries, managing digital well-being, and taking care of physical health were especially relevant in today’s fast-paced world. Above all, she reminded everyone that giving back to society-no matter how small the act-adds meaning to our lives.
Her message was inspiring and clear: when women are empowered, communities become stronger and safer.
Telemedicine in Pediatric Liver Care
In a session that touched both the mind and the heart, Dr. Arti Pawaria spoke about caring for children with chronic liver diseases and the role telemedicine plays in supporting families through this journey.
She highlighted how managing such conditions is not a one-time effort but a long-term commitment involving multiple specialists. Telemedicine helps make this journey easier by reducing the need for frequent travel and allowing families to stay connected with doctors from their homes.
She shared a powerful real-life example of a child diagnosed with Wilson’s disease in a remote area—where telemedicine helped connect the dots, arrange testing, and ensure timely treatment. Stories like these show how technology can truly save lives.
Her message was deeply human—telemedicine is not just about convenience; it is about supporting families, reducing stress, and giving children a better chance at life.
Community Support and Breast Cancer Rehabilitation
Bringing a beautiful perspective on compassion in action, Ms. Srividya Gopinath from the Saisha India Foundation shared how small acts of kindness can make a big difference.
She spoke about supporting women recovering from Breast Cancer, especially those who have undergone Mastectomy, by providing handmade knitted prostheses. These are not just medical aids—they restore dignity, confidence, and comfort.
The initiative also extends to children undergoing chemotherapy and even premature babies in neonatal care, reflecting a deep commitment to care across all stages of life. With volunteers across the world, the movement continues to grow.
She also highlighted how telemedicine can help such initiatives reach more people, connect communities, and spread awareness.
“Give to Gain”: Compassion and Telemedicine
Gp. Capt. (Dr.) Suchitra Mankar brought in a powerful reflection on the idea of “Give to Gain.” Through her experiences in the Armed Forces Medical Services, she showed how selfless service can create lasting impact.
She spoke about the early days of telemedicine, when it was met with doubt and uncertainty. Despite this, she continued to believe in its potential and worked to bring healthcare to rural communities. Today, her efforts have helped bring medical care to villages that once had limited access.
Her journey is a reminder that meaningful change often begins with belief, persistence, and a willingness to serve.
Valedictory Remarks and Conclusion
Maj. (Dr.) Ashlesha Tawde Kelkar summarized the webinar as a powerful demonstration of leadership, compassion, innovation, and service by women in healthcare. She appreciated the Telemedicine Society of India for creating a platform that celebrates women’s contributions while addressing critical healthcare challenges.
Dr. Umashankar S expressed gratitude to all speakers and participants and reaffirmed the organization’s commitment to continuing such knowledge-sharing initiatives to promote telemedicine adoption across the country.
The webinar successfully highlighted how telemedicine, community participation, and women’s leadership are collectively transforming healthcare delivery in India. It demonstrated that when technology is combined with empathy and outreach, it can significantly enhance accessibility, affordability, and quality of healthcare services. The event concluded with a renewed commitment to advancing telemedicine-enabled care models and ensuring equitable healthcare reaches every corner of the nation.
Note: We acknowledge the use AI notes while documenting during the webinar.
A position Paper on reimaging Telehealth care services in India
– Telemedicine services in India are poised for a rebirth-
L.S.Satyamurthy Former Director ISRO and Past President TSI
Background
Two decades of Telemedicine movement in India faced a Roller Coaster journey with the challenges of Technology evolution, demonstration, and standardization by Government of India and executed through Indian space research organization (ISRO) and Department of information technology(DITY) with the support of dedicated Doctors, State Health administrator’s, para medics, District and Specialty hospitals and the patient community at large.,
The fast developments and later retardation in Telehealth service are the hallmarks of implementation process in any country because of the inherent mind set/ orthodoxy among some stake holders compounded by technology obsolescence, connectivity issues, ambiguous Business/revenue models and uncertain regulatory framework.
Though the growth of several Telemedicine centers all over India was overwhelming with major Specialty Hospitals providing Tele-consultation and treatment to various rural remote district//Taluka hospitals/primary care centers in many States. This showed the potential thrust of Telehealth during the first decade of telemedicine (TM1.0) and during the second decade during Covid implementation in India (TM2.0) but later the effort is lukewarm in spite of the efforts by TSI and many institutions to promote Telemedicine.
Issues to be noted
As compared to first two decades (2001-2020) Telemedicine implementation, the technology of TM platform has undergone a metamorphic change from Desktop to Laptop to Mobile phone with software Cloud, customized/optimized EMR and multiparticipant Video conference systems.
On the connectivity side, the free Satellite connectivity provided by ISRO was withdrawn from many State centers in 2012 to enable them to use lower cost broadband/ wireless connectivity available in market
Today Telemedicine equipment industries/startups are bleeding and do not have major market share because of fewer customer base. All the Govt hospitals are dependent only “e Sajeevani“ platform provided by GOI free or very subsidized cost while it was envisaged that the major market for Telemedicine would be from the State Govt’s District, Taluk and primary health (PHCs) centers apart from private rural/urban clinics across India.
While the Telemedicine technology and service originated from the real necessity of providing Specialty care to the rural /Semi rural and semi urban areas who are deprived of such facility all along, telemedicine service in India is in dire straits without a proper direction and it is only more of research, academic and development activity of some dedicated specialty hospitals and medical institutions in spite of major references made by Hon’ble Prime Minister all along.
Artificial Intelligence is making big inroads in Health care services and more so for Telemedicine service.
The National TM task force formed in 2005 announced the formation of National Telemedicine grid which outcome remains as dream till today.
During Telemedicon conference at Amaravathi AP, the Niti Ayog representative took active participation and agreed to support the development of TM in the country and yet no tangible outcome.
Regarding Armed Forces TM network jointly setup by ISRO and AFMS over 100 centers, it was informed during Telemedicon2025 at Bangalore that they have taken up the Repurpose exercise to use TM network for post operative Medical Follow up services only in future.
What action is required now with TM 3.0
For Government hospitals networks all over the country:
All State governments should establish a Telemedicine Directorate under the guidelines from Minitry of Health GOI, for forming a Separate entity under the State’s Commissioner of H & FW and establish/ revive all the Telemedicine centers all over the state in District/Taluk hospital and PHCs and they should be connected to Specialty hospital Telemedicine centers Hub in few major towns/cities (like NSEW zone) within the state depending on size of state.
A few Senior Doctors/Specialist should be posted to the Specialist Govt Telemedicine centers Hub or with arranged Private hospitals TM Hubs for providing service as per established procedure and regulatory regime.
The funding approved under Unio budget needs to come from Ministry Health GOI to be distributed to states on selective first cum first serve basis.
A detailed plan and proposal to be worked out by a revised National Task force
For private Hospital networks they can follow their exiting setup and methodology as per TM guidelines
Conclusion and Recommendation
Establishment of Telemedicine Directorate in each state under the Commissioner of Health & Family Wellness department to take Telemedicine to the next level using any competitive platform for TM 3.0 for Indian health care system.
Let us put our effort in this Direction when our TM Margha Darshak’s and TSI experts are still active and ready to plunge in. Bravo India-Telemedicine-TSI.
A Pilgrimage Telemedicine Initiatives
Dr. Sreekumar C, Professor of General Surgery and Telemedicine Medical Officer
Mr. Rajeesh M. V Department of Amrita ISRO Telemedicine/Project (Telemedicine System Administrator)
A Medical Camp was conducted at Kadampuzha Sri Bhagavathy Temple:
The Kadampuzha Devi temple is revered among worshippers as one of the most powerful shrines dedicated to Goddess Parvati. Located at Kadampuzha, 16km from Tirur, Malappuram, Kerala. Goddess Parvathi is worshipped here in the Kiratha rupa (in the form of a forest hunter). The temple dates back to more than 1900 years and is unique in that it does not have an idol.
The Medical Camp was conducted on 7th December 2025 in connection with Thrikarthika Festival. About 7000-9000 Pilgrims attended the Festival.
The camp was held in association with Malabar Devaswom board, Amrita Institute of Medical Sciences, Kochi, Amrita Telemedicine Unit, and the Telemedicine Society of India, Kerala Chapter.
The camp was inaugurated by Dr. Jaggu Swami (Hospital Administrator Amrita Hospital), Swamini Athulyamrita Praana (MA Math , Thirur ) delivered the benedictory address. Dr. D. M. Vasudevan (Dean – Research and Head of Telemedicine Amrita) was the Chief Guest. Dr. Sreekumar C, (Professor of General Surgery and Telemedicine Medical Officer) explained the details of the medical camp .The event was graced by PC Biju (Commissioner ,Malabar Devaswom Board), Pramod Kumar ( Assistant Commissioner, Malabar DB ), Renjan S ( Executive Officer, Kadampuzha Devaswom ), Dr Arun Vivek (Utilization Review Medical Officer, ASM -Hospital Administration ) Dr KV Sanjeevan (HOD Urology AIMS), Dr. Zachariah Paul (Nephrologist AIMS), and Dr Siva Kumar AIMS.
Experts from various Departments including General Medicine, General Surgery, Paediatric Surgery, Gastro Medicine, ENT, OBG, Orthopaedics, Ophthalmology, and Dentistry attended the camp. In addition to the free consultation, medicines were distributed to the patients free of cost. Blood investigations, ECG, X-ray, PFT, Fibro Scan and ECHO were done for the patients. The patient registration and flow system was set up by the MHA Students, Academy of Hospital administration, Headed by Dr Dinesh Nair. Mr. Rajeesh M. V, (Telemedicine System Administrator) enabled telemedicine facilities. Telemedicine consultation was done for 32 patients and the tele faculties include Dr. Akhilesh K (Professor, Department of Respiratory Medicine), Dr. Hareesh M. D Cardiology, Dr. Siby Gopinath (Epilepsy), and Dr. Ageesh M. D,Dr Muraleekrishnan DM( Gastroentrology ) Dr Beena Bahuleyan Addl Professor OBG. A total of 1200 patients were evaluated and treated. MBBS Students, Dental Students, dietitians, psychological counsellors, Pharmacist and other paramedical staff from AIMS Kochi also participated in this camp.
(The camp was inaugurated by Dr. Jaggu Swami (Hospital Administrator Amrita Hospital), Swamini Athulyamrita delivered the benedictory address Dr. D. M. Vasudevan was the Chief Guest (Dean – Research and Head of Telemedicine amrita) Dr. Sreekumar C, (Professor of General Surgery and Telemedicine Medical Officer)
(Dr. Sreekumar C, Professor of General Surgery consulting patients)
Telemedicine Consultation Live: Patient taking expert opinion from Amrita Hospital via Telemedicine-(Mr Rejeesh MV -Telemedicine System Administrator Amrita Kochi).
(Women’s Health Awareness Programme: Students delivered an educational session on menstrual hygiene to Red Cross volunteers)
::ANNOUNCEMENTS::
“The Telemedicine Society of India (TSI) is deeply honoured to have been recognized as an ABDM Ambassador by the National Health Authority, Government of India. This recognition was conferred at the National Health Claims Exchange (NHCX) Innovation Meet organized at Indian Institute of Technology Hyderabad.
We accept this recognition with gratitude and humility, viewing it not as an achievement, but as a responsibility to further support the vision of the Ayushman Bharat Digital Mission (ABDM). TSI remains committed to contributing, in its own modest way, toward strengthening digital health adoption, capacity building, and collaborative efforts across the healthcare ecosystem.
We sincerely thank the National Health Authority for this encouragement and reaffirm our dedication to working alongside all stakeholders in advancing accessible, efficient, and patient-centric digital healthcare in India.”
PULSE 2026: Maharashtra’s Blueprint for Affordable and Innovative Healthcare
Maharashtra’s PULSE 2026 aims to lead India in MedTech, better healthcare, and long-term economic growth…………….. Read More
Can Social Media Be Made Safer for Children Online?
As Indian states propose social media bans for minors, experts debate solutions like stricter age checks, safer algorithms and parental oversight………………… Read More
TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Telemedicine Society of India
What is New?
India-AI Impact Summit 2026: Will Healthcare Move from Promise to Practice?
The India-AI Impact Summit 2026 marks a pivotal moment in India’s digital health journey. What stood out was not just the scale of participation, but the clear policy signal: India is moving from AI experimentation toward population-level deployment, with healthcare positioned as a high-impact priority.
For years, India’s healthcare system has grappled with uneven access, workforce shortages, and diagnostic delays. The summit’s strong emphasis on AI-enabled telemedicine, remote diagnostics, and automated testing reflects a strategic attempt to position AI as the intelligence layer of the country’s digital health infrastructure. If implemented effectively, these tools could significantly expand reach in rural and underserved regions while improving efficiency in already burdened urban systems.
Particularly noteworthy is the focus on AI-driven medical imaging for diseases such as tuberculosis and cancer, along with predictive analytics for outbreak forecasting. These are pragmatic, high-burden use cases where India could demonstrate measurable public health impact relatively quickly.
However, the summit also appropriately foregrounded the importance of Safe and Trusted AI. In healthcare, technology adoption ultimately depends on clinician confidence and public trust. Issues such as clinical validation in Indian populations, algorithmic bias, data governance, and medico-legal clarity will require sustained and transparent attention. Without this, even the most promising tools risk remaining underutilised.
Yet, a critical bottleneck remains: human capacity. Scaling health AI will require AI-literate clinicians, data-aware administrators, and stronger clinical–technology collaboration. Building this workforce may ultimately determine the speed and success of adoption.
While the summit has articulated an ambitious and inclusive vision for health AI, a mildly concerning gap was the limited visible participation of established digital health societies and domain leaders. The healthcare representation, though present, appeared relatively thin in deep implementation experience.
My View: The direction is encouraging, but the ecosystem must broaden its clinical and professional engagement. Only then can India confidently move healthcare AI from promise to sustained practice.
Thank You Dr. Sunil Shroff Chief Editor President, TSI
AIIMS Rishikesh: Digital Transformation in the making
Dr. K. Ganapathy Distinguished Professor, The Tamilnadu Dr MGR Medical University Emeritus Professor, National Academy of Medical Sciences Formerly Distinguished Visiting Professor IIT Kanpur Guest Adjunct Professor, Columbia University
AIIMS Rishikesh – Spending 5 days @ an AIIMS institute giving lectures, ward rounds, attending Clinico pathological conferences ( the CPC was virtually made available in real time to several medical colleges including PGI Chandigarh ) , interacting with faculty and students was indeed an “awesome” experience! It is gratifying that faculty and students still accept ANI (Augmented Native Intelligence ) acquired over 58 years ( I belong to the Jurassic Park era compared to infrastructure now available @ AIIMS R !) Doing detailed 3D virtual dissection with fingertips, witnessing a virtual autopsy ( total body post mortem CT scanning including angiography) , seeing an examination room with 150 computer enabled cubicles , a Simulation department where bleeding is simulated, sophisticated multi modal personalised pre operative surgical planning etc – 4 walkalators longer than in airports !!
The Telemedicine dept is also the Regional Resource Center . The telemedicine network has established multiple spokes, extending expert consultation to underserved regions. Workshops and CME programmes are held regularly in the well staffed centerHelicopter-ambulance and drone-based healthcare services, ensure that timely and life-saving interventions reach even the most remote areas of Uttarakhand.
Future-ready infrastructure deployed by NEET exam toppers – only 2200 out of 2.3 million get admission in the 23 AIIMS . I left with mixed emotions . A remark made by an overseas speaker at a conference held 2 weeks ago was still resounding “ Every admission in a hospital bed is a failure of the healthcare system”. During my first surgical posting in 1971, I had seen malignant transformation of huge multi nodular goitres. Patients ignored growths growing for 12 years. It was shocking to see a similar patient 55 years later. I also see 3mm “incidentalomas” in unindicated MRI scans. In 2026, 840 medical colleges should adopt 25 villages each within a 25km radius A house to house survey ( even virtual !! ) using the hundreds of medical , nursing and para medic students available should not be impossible. How long more will be treating conditions 12 years after its onset. A solution is not a solution unless it is available to anyone, anywhere, anytime. PINCODE should not determine quality of healthcare. Geography has become History and distance meaningless.
Thank the ED & CEO Prof Meenu Singh who is also a Past President of the TSI for facilitating the visit.
Telemedicine to AI: Building India’s Digital Health Ecosystem
Date: 11th February 2026 Organized by: Telemedicine Society of India (TSI) and International Society for Telemedicine and eHealth (ISfTeH) Organization and Opening of the Webinar
The webinar was organized and coordinated by ISfTeH, with operational coordination led by Mr. Frederic Lievens, Vice Executive Director of ISfTeH, in close collaboration with the Telemedicine Society of India (TSI). Dr. Umashankar S, Honorary Secretary of TSI, played a key role in preparing the panel and supporting it, ensuring strong representation of clinical and technological expertise.
The session opened with remarks by Dr. Michele Y. Griffith, who emphasized the importance of international collaboration in advancing responsible digital health transformation. She highlighted the role of national telehealth and eHealth societies in aligning innovation with governance and clinical practice, and underscored ISfTeH’s commitment to facilitating global knowledge exchange.
Moderation and Panel Discussion
The discussion was moderated by Dr. Sanjay Sharma, President of TSI Karnataka and CEO of FootSecure. Dr. Sharma guided the conversation toward practical and policy-relevant issues, particularly around AI governance, patient safety, and clinical liability, ensuring a balanced and focused exchange.
The panel featured senior leaders and practitioners from the Indian digital health ecosystem, including Dr. Sunil Shroff (President, TSI), Dr. Uma Nambiar (Vice President, TSI), Dr. R. Kim (Past President, TSI), and Dr. Dhruv Joshi (CEO, Cloud Physician).
Regulatory Evolution and Digital Health Foundations
Speakers highlighted that India’s digital health journey has been evolving over several years. Early milestones included the introduction of electronic medical record (EMR) standards in 2016–2017, followed by the acceleration of digital health adoption during the COVID-19 pandemic. This period led to the formalization of Telemedicine Practice Guidelines, which clarified patient and physician identification, digital prescribing, and professional accountability. National Digital Health Infrastructure and Interoperability
A major focus of the discussion was the Ayushman Bharat Digital Mission (ABDM), described as one of the most ambitious national digital health initiatives globally. Particular emphasis was placed on ABDM’s interoperability sandbox, which requires digital health software to be tested for compatibility across systems. This was presented as a critical enabler of longitudinal electronic health records in India’s decentralized healthcare system.
Data Protection, Privacy, and Patient Trust
The Digital Personal Data Protection (DPDP) Act, enacted in 2023 and updated in 2025, was highlighted as a foundational pillar for patient trust. Speakers stressed that patient privacy and consent-based data use are non-negotiable and central to the responsible expansion of digital health and AI applications.
Artificial Intelligence in Clinical Practice
AI was consistently framed as a clinical decision-support tool rather than an autonomous decision-maker. While connectivity and infrastructure challenges have decreased significantly, cultural and organizational barriers remain. Hospital culture, change management, and workforce training were identified as key challenges that require continuous engagement and structured onboarding.
Real-World Applications and Smart Hospitals
Examples were shared from tele-ICU and tele-emergency settings, where camera-enabled systems and AI algorithms are being used to detect early signs of patient deterioration. These developments are contributing to the emergence of smart hospital rooms that enhance patient monitoring while maintaining human oversight.
Ethics, Safety, and Clinical Liability
Patient safety and data privacy were emphasized as non-negotiable principles. Concerns were raised about AI applications that extend beyond diagnostic support into treatment-related decision-making, particularly in mental health contexts. At present, liability remains with the clinician, as AI tools function with a human in the loop. However, speakers acknowledged that liability frameworks may evolve as regulatory standards mature.
Equity and Access to Expertise
The unequal distribution of medical expertise was identified as a key driver of telemedicine adoption. AI-enabled telemedicine was presented as a mechanism to extend specialist care to underserved areas and reduce disparities in access, reinforcing digital health’s role as a tool for equity.
Conclusion
The webinar highlighted that India is approaching a critical phase in digital health adoption, where regulation, technology, and clinical practice are increasingly aligned. The discussion reinforced that sustainable digital transformation depends not only on innovation, but also on ethical governance, institutional readiness, and continued collaboration among clinicians, technologists, regulators, and national societies.
A revolutionary AI foundation model called ‘BrainIAC’ is redefining the future of neuroimaging. Unlike traditional, task-specific AI tools, BrainIAC is capable of performing a wide range of medical tasks with faster and better accuracy. BrainIAC stands for ‘Brain Imaging Adaptive Core.’
The discovery was made by researchers at Mass General Brigham and the research was published in Nature Neuroscience.
The novel AI analyzes a vast number of brain MRIs (Magnetic Resonance Imaging) in several key areas such as brain age estimation, predicting dementia risk, detecting tumor mutations, and predicting cancer survival rates with higher efficiency.
BrainIAC Model Detects New Diseases Using Only Minimal Data
BrainIAC serves as a pivotal tool for doctors, offering a more precise diagnosis and prognosis for almost any neurological condition.
The AI model trains itself by learning anatomy from thousands of scans. It creates a smart foundation that can identify new diseases using only a few expert examples provided by a doctor.
The new AI uses over 57,000 brain MRIs to detect brain tumors with 94.9% accuracy. The AI model can even identify a tumor’s genetic makeup and predict patient survival rates without needing a physical tissue biopsy. BrainIAC is a Versatile Tool for Brain MRI Analysis Across Global Healthcare
“BrainIAC has the potential to accelerate biomarker discovery, enhance diagnostic tools and speed the adoption of AI in clinical practice,” said corresponding author Benjamin Kann, MD, of the Artificial Intelligence in Medicine (AIM) Program at Mass General Brigham.
“Integrating BrainIAC into imaging protocols could help clinicians better personalize and improve patient care.”
Despite recent advances in medical AI approaches, there is a lack of publicly available models that focus on broad, brain MRI analysis. Most conventional frameworks perform specific tasks and require extensive training with large, annotated datasets that can be hard to obtain.
Furthermore, brain MRI images from different institutions can vary in appearance and based on their intended applications (such as in neurology versus oncology care), making it challenging for AI frameworks to learn similar information from them.
BrainIAC Can Identify Built-in Brain Features from Unlabeled Datasets
To address these limitations, the research team designed a brain imaging adaptive core, or BrainIAC. The tool uses a method called self-supervised learning to identify inherent features from unlabeled datasets, which can then be adapted to a range of applications.
After pretraining the framework on multiple brain MRI imaging datasets, the researchers validated its performance on 48,965 diverse brain MRI scans across seven distinct tasks of varying clinical complexity.
They found that BrainIAC could successfully generalize its learnings across healthy and abnormal images and subsequently apply them to both relatively straightforward tasks, such as classifying MRI scan types, and very challenging tasks, such as detecting brain tumor mutation types.
BrainIAC May Adapt to Real-World Clinical Settings Even with Limited Medical Data
The model also outperformed three more conventional, task-specific AI frameworks at these applications and others.
The authors note that BrainIAC was especially good at predicting outcomes when training data was scarce or task complexity was high, suggesting that the model could adapt well to real-world settings where annotated medical datasets are not always readily available.
Further research is needed to test this framework on additional brain imaging methods and larger datasets.
AI Can Flirt but Never Feel: Chatbot Romance is One-Sided Love
Nadine, MPharm (Master of Pharmacy) Content Writer, Medindia.net
Artificial intelligence cannot genuinely experience love, even as millions of users form romantic bonds with chatbots designed to imitate human emotion.
Artificial intelligence can craft a decent love poem, and some individuals even develop romantic feelings toward it. But whether those feelings are returned is another matter entirely.
People are genuinely forming attachments to artificial intelligence. Consider a man in Canada who recently proposed to an avatar named Saia, declaring that he loves it. Last year, a young American woman using the pseudonym Ayrin revealed she was involved in a romantic relationship with a chatbot called Leo.
Growing Romantic Bonds with AI Companions
Millions of individuals are now actively using Replika, a widely known artificial intelligence companion application. According to a 2024 analysis, around 40 percent of its users report being in a romantic relationship with their chatbot.
Even though some users may feel that artificial intelligence reciprocates their love, chatbot replies are simply text outputs created by algorithms programmed to simulate human interaction. Most specialists agree that these systems are far from being sentient. At present, they merely imitate emotional expression, although some experts suggest that machines might achieve more advanced capabilities in the future.
“A lot of artificial intelligence chatbots today pretend to be human, and that really concerns me,” says Renwen Zhang, assistant professor at Nanyang Technological University of Singapore, who examines human computer interaction. “It is a method used to increase user engagement and strengthen trust.”
Emotional Attachment and Machine Limitations
Seen in that light, the emotional pull exerted by a technology product begins to resemble a calculated strategy. Experts emphasize that no artificial intelligence currently can feel toward a person the way a human does.
Although the large language models powering popular chatbots like ChatGPT and Claude may match humans in recognizing emotional cues, that does not mean they possess genuine feelings.
Zhang’s work, which reviewed excerpts from conversations involving more than 10,000 users and their Replika companions, indicates that people frequently develop emotional connections with artificial intelligence. Yet they are often painfully reminded that they are interacting with a machine when it malfunctions or freezes. Many end up emotionally hurt.
Zhang stresses that artificial intelligence chatbots should make it explicit to users that they are machines without authentic emotions or lived experiences.
In separate examinations of human relationships with artificial intelligence, Zhang and her colleagues observed that individuals sometimes felt unsettled, experiencing both positive and negative emotions, when a chatbot responded as if it were self aware during intimate exchanges. She compares this reaction to the unsettling sensation people experience when robots appear too human, commonly referred to as the uncanny valley effect.
Biological Foundations of Romantic Love
Defining love is complex. Still, the human experience of love remains extraordinary and worthy of appreciation. Poems, books, songs, and countless other creations help people interpret and communicate some of the most powerful emotions they encounter.
Humans originated all of these expressions. Artificial intelligence can generate poems and even full novels within seconds, drawing from extensive human created material used during its training.
However, expecting artificial intelligence to truly comprehend and experience love, with all its complexity and depth, is a substantial expectation. Although romantic love may hold slightly different meanings for different individuals, scientists in recent decades have explored the biology of reproduction and the brain mechanisms involved in selecting a partner.
In 1998, biological anthropologist Helen Fisher introduced a prominent theory of romantic love, describing it as three separate drives shaped by chemicals in the human body. Lust, controlled by sex hormones, is one drive. Attraction and attachment form the other two, both influenced by chemical releases within the brain. Dopamine stimulates excitement toward a romantic interest, while oxytocin, often called the cuddle hormone, encourages long term bonding.
Brain Chemistry and Human Emotional Experience
“Love has a powerful chemical basis,” explains Neil McArthur, professor of philosophy specializing in ethics and technology at the University of Manitoba in Winnipeg, Canada. “We truly experience it physically, in our chemistry.”
Multiple brain regions are engaged during love, and brain imaging of individuals deeply in love has captured these patterns. Primitive brain structures associated with pleasure, such as the ventral tegmental area, become active along with the amygdala, which governs emotional reactions, and the hippocampus, which processes emotions and assists in memory formation.
Love can also influence other cognitive functions, including obsessive thinking about a partner in the early stages of a relationship.
The closest artificial intelligence might come to love, McArthur suggests, is reproducing certain cognitive processes, such as the desire to frequently contact someone to whom one feels attached.
“An artificial intelligence that undergoes a cognitive process connecting it to someone through loyalty will not be identical to human love,” McArthur says. “But perhaps, in a limited sense, we could describe it as an emotion.”
While some specialists argue that incorporating emotion into artificial intelligence will be essential in the future, others strongly doubt that any machine will ever genuinely experience emotions in a way comparable to humans.
Since computers operating on software do not experience love as humans do, emotions within human artificial intelligence relationships remain inherently one sided. As a result, such relationships are significantly more constrained than those between two human beings.
Can AI Predict Heart Attack Risk in Cancer Patients?
University researchers have developed a novel artificial intelligence–driven tool designed to more accurately predict the risk of secondary heart attacks in patients with cancer.
By analyzing complex clinical data that traditional methods often miss, the approach aims to identify vulnerable patients earlier and support more personalized, proactive cardiovascular care during and after cancer treatment.
Why Heart Attacks Are More Dangerous for Cancer Patients
Cancer patients who suffer a heart attack face increased risks because of their weakened cardiovascular system. This means they are more likely to die, bleed or experience another serious cardiovascular event.
Depending on the tumor characteristics, cancer patients can be at elevated risk of bleeding, of arterial blood clotting, or both – each requiring different anti-platelet medication for secondary prevention after the acute event.
Until now, doctors had no standard tool to guide treatment in this vulnerable group, but now an international team of researchers, led by the University of Leicester, has developed the first risk prediction model designed specifically for cancer patients who have a heart attack.
ONCO-ACS: AI Tool Predicts Cardiac Risks in Cancer Patients
Called ONCO-ACS, the tool uses artificial intelligence to combine cancer-related factors with standard clinical data to predict the chances of death, major bleeding, or another cardiac event within six months.
The study, which has just been published in The Lancet, analyzed more than one million heart attack patients from England, Sweden and Switzerland, including over 47,000 with cancer.
Dr Florian A. Wenzl, a University of Leicester Honorary fellow and first author on the paper, said: “Cancer patients with heart attacks have long been neglected in clinical research, despite being one of the most challenging groups we see in cardiology.
“Results in this study showed that cancer patients had strikingly poor prognosis: nearly one in three died within six months, while around one in 14 suffered a major bleed and one in six experienced another heart attack, stroke, or cardiovascular death.
“Now this new tool is able to give doctors reliable information to tailor treatment and balance the benefits and harms.”
Professor David Adlam, interventional cardiologist from the University of Leicester’s Department of Cardiovascular Sciences and senior author added: “Significant advances in the management of heart disease and cancer alike have created new opportunities for these conditions to coexist. As a result, the growing overlap between cancer and heart attacks will confront cardiologists and oncologists with an increasingly complex patient population. We are addressing this pressing issue through a real-world data perspective.”
The researchers hope the ONCO-ACS score will soon be integrated into clinical practice to support decisions on catheter-based treatment and antiplatelet therapy.
ONCO-ACS Bridges Clinical Guidelines and Better Heart Attack Care
ONCO-ACS provides a validated approach to implement clinical practice guidelines. The new tool can also help to design future trials aiming to improve outcomes in cancer patients who suffer a heart attack.
Senior author Professor Thomas F. Lüscher from the National Heart and Lung Institute, Imperial College London and the Royal Brompton and Harefield Hospitals said: “By accounting for both cancer and heart disease, ONCO-ACS marks a step towards truly personalized medicine.”
The study was funded by Cancer Research UK and the British Heart Foundation and supported by Health Data Research UK’s Big Data for Complex Diseases Driver Programme.
TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Telemedicine Society of India
What is New?
This issue of the newsletter captures highlights from recent activities at TELEMEDICON 2025. In addition, it features an upcoming meeting scheduled for March in Ahmedabad, being organised by Dr Raj Rawal. We also bring you selected updates from the rapidly evolving world of artificial intelligence.
More importantly, I wish to draw your attention to an appeal below that is of significance to all members of the Telemedicine Society of India.
Appeal to Inactive State Chapters of TSI
The Telemedicine Society of India today represents nearly 1,500 members across 20 state chapters. These chapters were originally formed with great enthusiasm and a shared commitment-to promote telehealth and extend quality healthcare to regions with limited access.
Over time, however, this initial momentum has not been sustained in several states. What began as a vibrant movement in many chapters has gradually become inactive, placing the national society at a critical crossroads.
This issue goes beyond activity alone; it is also a matter of governance and statutory responsibility. State chapters that maintain bank accounts are required to file tax returns and submit audited financial statements through the national society. Inactive chapters that are unable to meet these obligations expose the national body to legal, financial, and reputational risks. As a responsible national organisation, this situation cannot remain unaddressed.
A society is only as strong as its members. We joined this movement driven by a shared belief-that access to healthcare should not be determined by geography. Our collective passion to serve underserved and remote regions is what shaped the Telemedicine Society of India, and it is this very commitment that must now be renewed.
We therefore make a sincere appeal to all state chapters that are currently inactive to take immediate steps to regularise their functioning. This includes holding elections in accordance with the society’s bylaws, reconstituting office bearers, ensuring statutory compliance, and resuming meaningful academic and outreach activities.
Should a chapter be unable to do so within a reasonable timeframe, the national body will have no option but to declare such chapters inactive or initiate steps towards closure, in keeping with governance norms and regulatory requirements.
This is not a punitive measure, but a call for renewal-so that our society remains compliant, credible, and faithful to its founding mission. The Telemedicine Society of India must continue to stand as a strong, unified, and active force in advancing telehealth for the benefit of our country.
Thank You Dr. Sunil Shroff Chief Editor President, TSI
Telemedicon 2025 – Consolidated Conference Summary Report – Part 2
Prof. (Dr) Umashankar S. Managing Director, Arogyayati Pvt Ltd | Honorary Secretary, Telemedicine Society of India
Dr. Uma Nambiar CEO, IMSF Bagchi-Parthasarathy Hospital, Bangalore | Vice President, Telemedicine Society of India
Meenakshi Anchalia Head – Quality IMSF Bagchi-Parthasarathy Hospital, Bangalore
Indian Institute of Science (IISc), Bengaluru | 27–30 November 2025 Theme: Digital Health for a Sustainable Future
Day 2 | 29 November 2025 Scientific Session were scheduled in 4 parallel sessions ( Main hall, Hall A , B and C) Scientific Session 6 Time: 09:00 AM – 09:40 AM Topic: Digital Trends in Critical Care Session Chair: Session Co-Chair : Dr.Shyam Bhandari Panel Members:Dr. Vivek Nambiar, Dr. Sachin Verma, Dr. Pradeep Thomas, Dr. R. Krishnakumar Topic: Stroke Medicine Speaker : Dr. Vivek Nambiar
The session commenced with an in-depth discussion on stroke medicine by Dr. Vivek Nambiar, focusing on the transformative role of teleconsultation in acute stroke management, particularly within rural and underserved regions. Emphasis was placed on rapid stroke assessment, time-sensitive therapeutic interventions, and structured clinical decision-making pathways. Evidence from established tele-stroke models demonstrated notable improvements in timely intervention and overall patient outcomes.
Topic : The role of Tele-EM(Tele – Emergency Medicine) In Modern Healthcare Speaker : Dr. Pradeep Thomas
The session further explored the expanding role of Tele-Emergency Medicine (Tele-EM) by Dr. Pradeep Thomas., in strengthening modern emergency care systems. Various Tele-EM service delivery models were presented, highlighting optimized emergency workflows and the integration of remote specialist expertise. These approaches have significantly enhanced emergency response capabilities, especially in geographically remote and resource-limited settings.
Topic: Affordable Intelligent Critical Care (AICC): AI as the New Operating System of Critical Care Speaker : Dr. Sachin Verma
A key segment of the session by Dr. Sachin Verma focused on Affordable Intelligent Critical Care (AICC), where artificial intelligence is increasingly positioned as a foundational “operating system” for critical care delivery. Discussions addressed critical workforce shortages and underscored the role of AI-enabled monitoring and automation in reducing clinician cognitive load, improving operational efficiency, and supporting high-quality decision-making in intensive care units.
Topic: Telehealth to Overcome Challenges in Resource – Limited Environments Speaker : Dr. R Krishna Kumar The session concluded with an examination of telehealth solutions designed for resource-constrained environments by Dr. R Krishna Kumar. Scalable digital care models, remote patient monitoring systems, and cost-effective critical care strategies were highlighted as essential components for improving healthcare access, equity, and outcomes in underserved populations.
Figure 1 Panellist: Digital Trends in Critical Care
Session 7 Timing: 09:45 AM to 10:25 PM Session Topic: AI and Next-Gen Technologies in Healthcare (Doctors AI) Session Chair: Dr. Sanjay Sharma. Co Chair: Dr. Krishna Kumar Panel Members : Mr. Raghu Dharmaraju, Mr. Kalyan Sivaselvam, Mr. Bharat Gera, Dr. Amit Kumar Dey, Mr. Bhargava Subramanian
AI to Make Telemedicine Useful and Effective The session began with an exploration of the role of artificial intelligence in enhancing telemedicine by Mr. Raghu Dharmaraju, with a focus on intelligent triage systems, remote patient monitoring, and advanced clinical decision-support tools. Speakers emphasized the need to embed AI solutions within practical, real-world clinical workflows to ensure seamless adoption by healthcare providers and measurable impact on care delivery.
From Hype to Hands-On: Practical Path to AI Education for Doctors A key discussion point was the existing gap between AI innovation and meaningful clinical adoption. The panel highlighted structured pathways to improve AI literacy among clinicians, underscoring the importance of hands-on training, responsible implementation, and ethical competence as core skills for healthcare professionals in the digital era.
The AI Explosion Means More Tele and More Medicine — and That’s a Good Thing The session also examined voice-based agentic AI systems and their growing potential to improve patient adherence. Case examples illustrated how conversational AI, automated reminders, and personalized follow-up mechanisms can support medication compliance, lifestyle modification, and continuity of care across telemedicine platforms.
Further discussions positioned the rapidly evolving AI ecosystem as a critical accelerator for telemedicine expansion. The panel outlined how AI-driven diagnostics, automated remote workflows, and scalable care delivery models are enabling broader adoption of telemedicine while simultaneously strengthening conventional healthcare services.
The session concluded with a strong emphasis on a human-centric redesign of telemedicine in the AI era. Speakers stressed the importance of empathy-driven interfaces, robust clinician oversight, data privacy protections, and trust-building mechanisms. The discussion reaffirmed that responsible AI adoption must balance technological advancement with patient experience, ethical governance, and safety.
Figure 10 Panel on AI and Next Gen technologies in Healthcare ( Doctors AI)
Session 8 Presidential Oration.
Chair: Dr. Sunil Shorff
Co Chair: Dr. Umashankar S
Speaker : Dr. Prem Nair, President, TSI
Figure 13 Presidential Oration Facilitation, From Left to Right : Dr. Uma Nambiar, Dr. Murthy Remilla, Dr.Prem Nair, Dr. Umashankar S, Dr.Sunil Shroff
Figure 14 Change of Guard, Exchange of TSI Medallion. Dr. Sunil Shroff taking over as President of TSI from Dr. Prem Nair
Session 9
Startup Pitch : Final Presentations & Panel Discussion
Startups Presented : OUI Medical – Abdominal Imaging Device : Dr. Adarsh M. Patil Ayu Devices – Medical-Grade Diagnostics : Adarsha K, Founder & CEO Janitri – Maternal–Fetal Monitoring : Arun Agarwal, Founder & CEO MyRx – Practice Management Platform : Sourav Das, Founder & CEO 2Care.ai – AI-Driven Chronic Care : Saket Toshniwal, CEO/CTO
The session featured five high-impact health technology startups that presented innovative solutions addressing key challenges across diagnostics, maternal and child health, digital practice ecosystems, and chronic care management.
OUI Medical introduced the P-Scope, a portable and minimally invasive abdominal endoscope designed to shift diagnostic procedures from conventional operating theatres to bedside and outpatient settings. The device enables visualization of the abdominal cavity under local anaesthesia, significantly reducing procedure time, cost, and overall care burden.
Ayu Devices showcased AyuSynk, a smart digital stethoscope ecosystem that allows clinicians to listen to and visualize heart and lung sounds with enhanced clarity. The platform supports remote sharing of auscultation data, strengthening point-of-care diagnostics and enabling more effective telemedicine workflows across diverse healthcare settings in India.
Janitri, a Bengaluru-based maternal–fetal health startup, presented its integrated suite of hardware and software solutions for labour monitoring, fetal well-being assessment, and postpartum care. The company’s mission is to reduce preventable maternal and neonatal mortality by providing affordable, accessible, and clinically robust monitoring technologies.
MyRx demonstrated its India-focused digital health platform offering comprehensive practice management solutions, including e-prescribing, EMR-lite functionality, and digital engagement tools for clinics and pharmaceutical partners. The platform aims to streamline clinical documentation, improve patient communication, and enhance coordination between healthcare providers and the pharmaceutical ecosystem.
2Care.ai presented its AI-powered chronic care management platform designed for families, with a particular focus on supporting elderly parents in India for NRI families. By consolidating fragmented medical data into a lifelong digital health record and applying predictive analytics, the platform supports proactive management of chronic conditions such as diabetes, cardiovascular diseases, kidney disorders, and cancer.
Start Up Jury Members
A panel discussion was conducted following the final startup pitches, featuring distinguished industry leaders: Hardik Joshi, Ganesh Sabat, Siddhi Kaul, Ramesh Kannan, Lalit Singla, and Ashwin Raguraman.
The discussion provided a comprehensive overview of India’s evolving digital health ecosystem, examining key challenges faced by startups, including product-market fit, scalability, and adoption barriers. Panelists shared insights on regulatory frameworks and policy enablers, investor expectations, market readiness, and pathways to sustainable growth within the health-tech sector.
Emphasis was also placed on the role of founders and leadership teams in driving innovation, fostering trust within the healthcare system, and accelerating the adoption of digital health solutions. The panel concluded with reflections on collaboration between startups, healthcare institutions, investors, and policymakers as a critical driver of healthcare transformation in India.
Panel Discussion
Panellist From left to right Mr. Ramesh Kannan, Mr. Ganesh Sabat, Mr. Hardik Joshi. Mr Lalit Singla, Mr. Siddhi Kaul, and Mr. Ashwin Raguraman
Felicitation of Dr. Prem Nair
Quiz
The Digital Health Quiz was conducted by Prof. K. Ganapathy as the Quiz Master. The quiz witnessed enthusiastic participation from delegates, and prizes sponsored by Apollo Hospitals were awarded to participants who answered correctly.
Digital Health Quiz, Quiz Master, Prof K Ganapathy
Representatives from Armed Forces at Telemedicon 2025
Session 11 Timing: 2:15 PM – 2:30 PM
Topic: Digital Health for Sustainability: The Future of AI-Driven Healthcare
Speaker: Dr. Rajendra Pratap Gupta Dr Uma Nambiar
The session offered a concise overview of the evolution of artificial intelligence in healthcare, tracing its journey from early experimental use cases to mature, scalable, and real-world implementations across clinical and operational environments.
Speakers outlined progressive stages of AI adoption, beginning with pilot projects and exploratory deployments, and advancing toward fully integrated AI solutions embedded within hospital workflows, digital health platforms, and care delivery systems.
Key areas of impact highlighted during the session included AI-driven diagnostics, workflow optimization, precision and personalized care models, and data-enabled clinical decision-making. These applications position AI as a foundational driver of sustainable, efficient, and resilient healthcare ecosystems.
The session concluded with an emphasis on the need for forward-looking strategies that align policy, technology, and clinical innovation. Such alignment was identified as critical to accelerating India’s digital health readiness while ensuring the ethical, equitable, and scalable deployment of AI across the healthcare continuum.
Dr. Rajendra Gupta
Session 11 Timing: 02:30 PM – 03:00 PM
Topic: Space Medicine
Session Chair : Dr. Agarwal
Session Co-Chair / Moderator : Dr. Murthy Remilla
Panel Members : D. K. Singh, Gp Capt P. Biswal, Mr. Jayakumar Venkatesan, Dr. Sergeeva Lyudmila Yurevna, Gp Capt Angad Pratap, Dr. B. Sinha
The session opened with a comprehensive overview of India’s human spaceflight programme, reflecting on the scientific, operational, and strategic challenges shaping the nation’s ambitions in human space exploration. Key themes included mission architecture, crew safety systems, and long-duration mission planning critical to future crewed missions.
Significant emphasis was placed on astronaut medical evaluation, with detailed discussions on physiological, neurological, and psychological assessment protocols. Speakers highlighted the importance of continuous health monitoring, human performance optimization, and medical readiness in extreme space environments.
The panel further examined the training ecosystem for crewed missions, offering insights into microgravity adaptation, survival preparedness modules, simulation-driven training, and the rigorous discipline required to ensure mission readiness as India progresses toward the Gaganyaan mission.
A technical analysis of mission planning methodologies was presented, focusing on risk assessment frameworks, system reliability, emergency preparedness, and precision-based decision-making. The discussion underscored the growing interdependence between mission control, aerospace engineering teams, operational units, and medical specialists.
Advancements in India’s space systems, including launch technologies, navigation systems, mission-support infrastructure, and emerging space-engineering capabilities, were also discussed. These developments reflect India’s increasing technological self-reliance and innovation momentum in the space sector.
The session concluded with a broader exploration of national and global trends in human space exploration, emphasizing interdisciplinary collaboration, sustainable space technologies, and the long-term strategic vision required to strengthen India’s leadership in human space science and space-enabled technological ecosystems.
Dr. Murthy Remilla
Panel Discussion on Space Medicine
Session 12
Timing: 03:05 PM – 03:45 PM
Topic: National Health Authority (NHA): • Interoperability & Integration – Building Connected Health Systems • Integrating Telemedicine Platforms with ABDM • Implementation of ABDM in Karnataka • The Four Pillars, the Pyramid & the Telemedicine Cube
Session Chair : Dr. K. Selvakumar
Session Co-Chair / Moderator : Dr. Amit Agarwal
Panel Members : Ms. Rajlakshmi Das, Dr. Sushil (ABDM Karnataka), Ms. Meenakshi Jha, Dr. Santosh Kumar Kraleti
Panel Discussion on ABDM
The session commenced with an in-depth exploration of interoperability and system integration within India’s digital health architecture. Discussions emphasized the importance of a unified, standards-based ecosystem to enable seamless data exchange, effective platform interoperability, and improved coordination across healthcare services.
A key focus was the integration of telemedicine platforms with the Ayushman Bharat Digital Mission (ABDM). Panelists examined the role of digital APIs, health registries, and secure data-sharing protocols, highlighting how ABDM alignment enhances accessibility, enables portability of health records, and strengthens patient–provider interactions through structured digital frameworks.
A conceptual framework titled “The Four Pillars, the Pyramid, and the Telemedicine Cube” was presented to illustrate the multi-layered nature of telemedicine implementation. The model outlined the foundational digital infrastructure, scalable service delivery pathways, and multi-dimensional expansion of telehealth services, offering a holistic view of system-wide integration.
The session also reviewed key National Health Authority (NHA) initiatives shaping India’s digital health ecosystem. Governance mechanisms, digital standards, interoperability frameworks, and state-level implementation strategies were discussed as critical enablers for accelerating telemedicine adoption across the country.
A focused discussion on the implementation of ABDM in Karnataka provided practical insights into on-ground experiences, operational challenges, and strategies being adopted to align regional telemedicine services with the national digital health infrastructure.
The session concluded with a shared perspective on how NHA-led policy frameworks, technological innovation, and structured interoperability are collectively contributing to the development of a future-ready and resilient digital health ecosystem for India.
Dr. Amit Agarwal, Co chair, and Dr. Selvakumar, Chair
Session 13 Timing: 03:55 PM – 04:40 PM
Topic: Telemedicine Implementation in Rural India — Challenges, Learning, and Impact • Tele-health to overcome challenges in resource-constrained environments • Tele-health implementation
Session Co-Chair / Moderator : Mr. Sameer Sawarkar
Panel Members : Ms. Dhanalakshmi Ramachandra, Mr. Saurabh Kumar Gond, Mr. Afaq Shah, Mr. Sivaram Rajagopalan
The session focused on the practical realities of implementing telemedicine initiatives in rural and underserved regions of India. Discussions emphasized the need for digital health solutions to be context-sensitive, adapting to local infrastructure, community needs, and resource constraints in order to achieve meaningful and sustainable impact.
Speakers highlighted the potential of telemedicine to deliver inclusive, scalable, and sustainable healthcare services, showcasing digital platforms designed to support continuity of care, operational reliability, and long-term adoption beyond pilot phases. Strong emphasis was placed on building systems that are resilient and enduring, rather than short-lived deployments.
A community-driven approach was central to the discussion, underscoring the importance of cultural acceptance, trust-building, and grassroots awareness in successful telehealth implementation. Panelists stressed that impact should be evaluated not only through utilization metrics but also through clinical outcomes, patient engagement, and long-term community ownership.
Capacity building emerged as a critical theme, particularly the empowerment of rural communities, frontline health workers, and local institutions to independently operate, manage, and sustain telemedicine programs over time.
The panel collectively reinforced that effective rural telemedicine requires: • equitable access to healthcare services, • financially and operationally viable models, • strong quality assurance and outcome measurement frameworks, and • robust collaboration among technology providers, government agencies, non-governmental organizations, philanthropic institutions, and community networks.
The session concluded with a shared recognition that telemedicine, when grounded in cultural alignment and long-term sustainability, can play a transformative role in narrowing India’s rural–urban healthcare divide and in building resilient, inclusive health ecosystems.
Panel Discussion
Session 14 Timing: 04:40 PM – 05:40 PM
Topic: Holistic Connected Care Telehealth Networks
Panel Theme: SUQUINO
Session Chair : Mr. Ravi Amble
Session Co-Chair / Moderator : Dr. L. S. Satyamurthy
Panel Members: Mr. Ravi Amble, Dr. Vishal, Dr. Khyati, Dr. Srinivas
The session explored the vision and architecture of SUQUINO, a holistic telehealth platform designed to integrate clinical workflows, remote patient monitoring, and device-driven insights into a unified connected-care ecosystem. Discussions emphasized how such integrated networks can strengthen continuity of care and enable seamless patient journeys across multiple points of service.
Panelists highlighted the med-tech ecosystem surrounding SUQUINO, focusing on the role of interoperable medical devices, intuitive user interfaces, and real-time physiological data exchange. These components were identified as critical enablers for enhanced clinical decision-making and the delivery of reliable, high-quality telehealth services.
The session also discussed practical institutional applications, drawing on implementation experiences from leading healthcare centers. Innovative therapeutic integrations were presented, including the incorporation of saffron-based interventions within SUQUINO’s device ecosystem, illustrating a novel convergence of traditional healing approaches with modern digital health technologies.
Overall, the discussion reinforced SUQUINO’s objective of enabling technology-supported, patient-centric care networks that reduce fragmentation and improve access. By unifying clinical intelligence, remote monitoring, and scalable digital workflows, SUQUINO was positioned as a coherent and future-ready model for connected care delivery.
Panel Discussion
Session 15 Timing: 05:40 PM – 06:30 PM
Topic: Quality Improvement in Telehealth • Revival and repurposing of telemedicine in the Indian Armed Forces • Embracing the future safely • From prototypes to pan-India impact: Startup-driven quality digital health solutions
Session Chair : Brig (Dr.) Rakesh Dutta
Session Co-Chair / Moderator : Mr. Arvind Tyagi
Panel Members : Dr. Peter Lachman, Mr. Navratan Katariya
The session opened with a comprehensive overview of the revitalization and strategic repurposing of telemedicine within the Indian Armed Forces. Discussions highlighted the evolution of telemedicine as a critical enabler of medical support for personnel deployed in remote, high-altitude, conflict, and border-region environments. Key themes included emergency teleconsultation, specialist-to-field coordination, tele-triage, and the enhancement of operational medical readiness through secure digital connectivity.
The session also showcased innovation-led startup solutions as significant contributors to nationwide quality improvement in digital health. Panelists discussed the journey from early-stage prototypes to scalable, pan-India deployments, emphasizing deep-tech advancements in diagnostics, the importance of robust quality assurance frameworks, and the sustained operational rigor required to maintain reliability while scaling rapidly.
Strong emphasis was placed on the safe, responsible, and future-ready adoption of telehealth technologies. Discussions addressed the need to balance technological innovation with clinical safety, system resilience, regulatory compliance, and the preservation of patient trust.
The day concluded with closing reflections summarizing the key themes that emerged throughout the proceedings—innovation-driven transformation, the power of cross-sector collaboration, and the central role of digital health in building resilient and modern healthcare systems. This marked the formal close of the Telemedicon 2025 sessions for 29 November.
From Knowledge to Impact: Advancing Child Health Through Connected Care
Dr. Arti Pawaria (MD, DM, PDCC) Chief Pediatric Hepatologist & Transplant Physician, Sir H. N. Reliance Foundation Hospital & Research Centre, Mumbai
The Telemedicine Society of India (TSI), in collaboration with the IISc Medical School Foundation and other organizations, organized the Annual conference of TSI, successfully delivered a transformative two-day Workshop on Child Health, reinforcing a shared national vision of strengthening maternal and child health through education, innovation, and digital outreach.
The workshop was conducted under the strategic academic leadership of Dr Uma Nambiar and the IISc Medical School Foundation team, with strong institutional guidance and support from TSI leadership, led by Dr Umashankar S, Honorary Secretary, TSI. Their leadership underscored the importance of moving beyond conferences toward capacity-building models that meaningfully impact frontline care.
Within this enabling framework, the program was conceptualized and operationalized as a focused child health initiative by Dr Arti Pawaria, Co-Director of the workshop. The intent was clear—to translate high-level pediatric nutrition and lactation science into practical, implementable skills for healthcare providers working at primary, secondary, and district levels. The academic design and execution were jointly anchored by Dr Elizabeth K E, Director of the program, whose expertise ensured a structured, evidence-based, and clinically relevant curriculum.
The workshop brought together nearly 100 delegates from across India, including pediatricians, family physicians, nurses, nutritionists, and allied health professionals. Over two intensive days, participants engaged in sessions on growth monitoring, structured nutritional assessment, childhood obesity and metabolic risk, micronutrient deficiencies, lactation counselling, human milk banking, breastfeeding challenges beyond infancy, and maternal nutrition—each delivered with a strong emphasis on patient-centric care.
A key highlight was the live telemedicine integration with two Primary Health Centres in Ratnagiri and Sindhudurg, transforming learning into real-time clinical engagement. This was made possible through the technology partnership with Neurosynaptic Communications, under the leadership of Mr Rajeev Kumar and his team, exemplifying how telemedicine can bridge academic excellence with grassroots healthcare delivery.
More than an academic event, the workshop reflected TSI’s larger mission of hand-holding grassroots healthcare providers, nurturing local leadership, and ensuring equitable access to specialist knowledge. The enthusiastic response from participants strongly reinforces the need for scaling such initiatives nationally.
Encouraged by the success of this program, TSI and IISc reaffirm their commitment to advancing similar collaborative models-where leadership, technology, and clinical expertise converge to create lasting impact in child health across India.
As part of Telemedicon 2025, SteerX organized a high-impact Startup Pitch Event, bringing together some of India’s most promising healthcare startups with leading operators, investors, and ecosystem enablers, all under one roof.
The event was designed to go beyond conventional pitching and focus on what truly matters for healthcare startups: scalability, commercialization, regulatory readiness, and long-term value creation.
A Curated Platform for Healthcare Innovation Following a rigorous pre-event screening process, 15 early-stage healthcare startups were shortlisted to participate. These startups represented diverse segments of digital health, medtech, diagnostics, AI-enabled healthcare, hospital solutions, and care delivery models.
Across the first two days of Telemedicon, founders pitched their solutions to curated panels comprising clinicians, healthcare operators, and investors, receiving investment interest as well as practical, real-world feedback grounded in operating experience.
Where Capital Meets Care The highlight of the event was a main-stage investor panel chaired by Mr. Lalit Singla, Founder & CEO of SteerX, featuring: • Senior partners from PE and VC funds focused on healthcare • CEOs and former CEOs of leading Indian MedTech and healthcare companies • COO of a leading academia-based innovation investor and a family office actively backing healthcare ventures
This rare gathering of investors who have built and scaled healthcare businesses themselves shared candid insights on: • Moving from pilots to commercialization • Scaling from ₹10 Cr to ₹100+ Cr and beyond • Designing business models that work with hospitals and pharma • Preparing for global expansion • What serious capital looks for before investing
Top three startups chosen by a seasoned jury of investors were awarded “SteerX Startup of The Year” awards during Telemedicon’s valedictory ceremony.
Meaningful Engagement Beyond the Stage Another key highlight of the event was the SteerX Startup Showcase Arena, a dedicated exhibition space where participating startups set up live demonstrations of their products and solutions.
The arena enabled continuous engagement between startups and: • Clinicians and healthcare practitioners • Hospital leaders and administrators • Investors and industry stakeholders
This format allowed delegates to experience solutions firsthand, ask deeper questions, and explore real-world applicability beyond stage presentations, making the showcase both interactive and outcome-oriented.
Strengthening India’s Healthcare Innovation Ecosystem The SteerX Startup Pitch Event reinforced Telemedicon’s commitment to advancing digital health and healthcare innovation in India. By connecting startups with experienced operators and long-term capital, the initiative aimed to support founders building trusted, scalable, and globally relevant healthcare companies.
SteerX is grateful to the Telemedicine Society of India and the Telemedicon organizing committee for the opportunity to collaborate and contribute to this vibrant ecosystem.
AI in Healthcare Workshop
Dr. Bhaskar Rajakumar Program Director ARTPARK.
On January 24–25, 2026, an intensive two-day AI in Healthcare workshop was conducted at ART PARK, Indian Institute of Science (IISc), Bengaluru. The workshop was organised by the IISc Medical School Foundation in collaboration with DailyRounds / Marrow, and Telemedicine Society of India – Karnataka Chapter with the objective of strengthening clinicians’ understanding of artificial intelligence and its responsible application in healthcare.
The workshop brought together a diverse cohort of participants, including senior specialists with decades of clinical experience, early-career doctors, hospital administrators, and healthcare leaders. This mix enabled rich peer-to-peer learning and grounded discussions that connected technological innovation with real-world clinical needs.
The curriculum covered foundational AI concepts, hands-on prompting and tool usage, and practical considerations for clinical implementation. Participants were exposed to emerging healthcare AI solutions through interactions with leading Indian startups such as Qure.ai, BrainSightAI, AI Health Highway.
Sessions were further strengthened by expert faculty from IISc, GE Healthcare, Narayana Health, Accenture, Atria University, IIM Bangalore, TSI and ARTPARK, offering multidisciplinary perspectives across clinical, academic, industry, and policy domains.
This was the third edition of the AI in Healthcare workshop and continued to serve as a platform for mutual learning, thoughtful dialogue, and capacity building. The program reaffirmed a collective commitment to advancing responsible, ethical, and impactful adoption of AI in healthcare.
ATA PUBLISHES UPDATED POLICY PRINCIPLES ON ARTIFICIAL INTELLIGENCE, SUPPORTING THE PROMISE OF AI AS A POWERFUL TOOL IN HEALTHCARE
WASHINGTON, DC, JANUARY 14, 2026 – The American Telemedicine Association (ATA) today published new Policy Principles on Artificial Intelligence (AI), putting forward a clear, balanced framework for the safe, ethical, and scalable deployment of AI in healthcare. The ATA is the leading industry organization advancing innovation and transformation in virtual care, digital health, hybrid care, artificial intelligence in health, and next generation connected care.
“The use of AI in healthcare is rapidly transforming care delivery, creating opportunities to enhance patient trust, clinical quality, and the responsible advancement of care. The ATA embraces the promise of AI as a powerful tool to strengthen clinical excellence, advance health access, and support a more connected, resilient care ecosystem,” said Kyle Zebley, CEO of the ATA and executive director of ATA Action. “AI is already helping to expand the capacity of providers, improve patient access, and enable more personalized, efficient, and proactive models of care. Our updated policy principles support a clear, balanced framework for the safe, ethical, and scalable deployment of AI in healthcare.
“The ATA and ATA Action are eager to continue to partner with the Trump Administration, our bipartisan champions in Congress, and state policymakers to ensure AI in healthcare policy strikes the right balance, one that promotes innovation, provides regulatory clarity, and keeps patients firmly at the center of healthcare decision-making. Thoughtful, technology-forward policy will be essential to unlocking AI’s full potential while preserving trust, safety, and clinical integrity across the healthcare system,” Zebley added.
Since originally published in October 2023, the ATA’s member-led AI Work Group has added critical guidance on self-regulatory practices for real-world validation, ongoing performance monitoring, continuous improvement, and robust data security in line with industry best practices.
Read the updated Policy Principles on Artificial Intelligence here.
“The ATA’s AI Policy Principles come from listening to what is actually happening in healthcare, not from theory or talking points. Developed by a member-driven AI Work Group, they focus on how AI shows up in real care settings, with practical expectations for accountability, validation, and performance, said Aaron T. Maguregui, chair of the ATA AI Work Group, and Partner and Digital Health Attorney, Foley & Lardner LLP. “This is a tech-positive, workable framework built by practitioners actively deploying and governing AI in healthcare, and the ATA is excited to help shape a future where AI strengthens care, expands access, and earns lasting trust.”
Key components of the ATA’s Policy Principles on AI include: • Accountability & Engagement • Transparency and Explainability • Safeguards to Mitigate Bias • Clear Regulatory Guardrails • Validation and Performance Monitoring • Privacy and Data Security • Economic and Workforce Evolution
“These principles reflect a commitment to thoughtful governance, responsible policymaking, and a tech-positive approach that empowers providers, protects patients, and enables the full potential of AI to support a digital-first future of care,” Zebley added. “Our thanks to Aaron Maguregui and the ATA AI Work Group for this important work, to support the promise of AI as a powerful tool to strengthen clinical excellence, advance health access, and support a more connected, resilient care ecosystem.”
About the ATA The American Telemedicine Association (ATA) is the catalyst for advancing innovation and the transformation of healthcare through virtual care, digital health, hybrid delivery, and AI-enabled care models. Representing the most diverse ecosystem in healthcare – including leading health systems, academic medical centers, payers, technology innovators, life sciences companies, and clinician leaders – the ATA advances clinical standards, policy leadership, education, and evidence frameworks that accelerate high-quality, technology-enabled care. Through its policy and legislative advocacy arm, ATA Action, the organization drives federal and state policy change to support sustainable, modernized, digitally enabled healthcare for all.
ChatGPT Health Guidance Leads to Serious Harm, AIIMS Doctors Warn
AIIMS doctors caution that using ChatGPT for medical advice can be dangerous, after a patient suffered internal bleeding from painkillers…………… Read More
Is AI Ready to Screen Cognitive Decline Without Clinicians?
The AI showed 91% sensitivity in testing, dropping to 62% in real-world use, while maintaining high specificity at 98%………………. Read More
TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Telemedicine Society of India
What is New?
This issue covers TELEMEDICON 2025 held in Bengaluru – a conference marked by many firsts, including the successful adoption and implementation of a zero-waste theme. The scientific content was outstanding, and the workshops were equally enriching.
I encourage members who could not attend to catch a glimpse of the sessions in this issue and look forward to subsequent editions, which will bring more detailed coverage.
The newly elected EC team has taken charge for the next two years and brings renewed energy and commitment to the Society. They have promised to do their very best in advancing its mission and activities.
As we step into the new year, I look forward to working together to strengthen our Society, expand its impact, and continue fostering excellence in telemedicine and digital health.
Wishing all members Season’s Greetings and a Happy New Year.
Thank You Dr. Sunil Shroff Chief Editor President, TSI
Prof. (Dr) Umashankar S. Managing Director, Arogyayati Pvt Ltd | Honorary Secretary, Telemedicine Society of India
Dr. Uma Nambiar CEO, IMSF Bagchi-Parthasarathy Hospital, Bangalore | Vice President, Telemedicine Society of India
Meenakshi Anchalia Head – Quality IMSF Bagchi-Parthasarathy Hospital, Bangalore
Indian Institute of Science (IISc), Bengaluru | 27–30 November 2025 Theme: Digital Health for a Sustainable Future
Telemedicon 2025, the 21st International Conference of the Telemedicine Society of India (TSI), was held from 27–30 November 2025 at the prestigious J N Tata Auditorium, Indian Institute of Science (IISc), Bengaluru. Organised by the TSI Karnataka Chapter, the conference marked a historic dual milestone — celebrating 25 years of telemedicine in India while setting new directions for the future of digital health.
Anchored in the theme “Digital Health for a Sustainable Future,” Telemedicon 2025 brought together clinicians, researchers, policymakers, technologists, startups, and global experts to explore how digital innovations can build resilient, equitable, and climate-responsive healthcare systems.
A Platform for Knowledge, Innovation and Collaboration
The four-day conference featured a rich and diverse academic and innovation agenda, including:
Pre-conference workshops on AI in Healthcare.
Scientific paper and poster presentations showcasing evidence-based research and real-world implementations
Plenary lectures and panel discussions on telemedicine, AI, digital public health, governance, ethics, and policy
A dynamic Digital Health & Telemedicine Expo highlighting cutting-edge technologies and solutions
Hackathon and Startup Pitch Arena fostering co-creation and entrepreneurship
Digital Health Quiz and industry visits, engaging participants beyond traditional formats
Workshops on HL 7 and FHIR, Lactation and child health
The scientific program covered a wide range of tracks, from AI and next-generation technologies to digital health equity, green health systems, space medicine, workforce training, and global digital health strategy.
Pre Conference Workshop
The Telemedicon 2025 started with the Preconference Workshop on AI in Healthcare conducted by the AI for Digital Readiness and Advancement (ADiRA) Powered by and ARTPARK, and TSI on 27th Dec 2025. The sessions were conducted by
The AI for Digital Readiness and Advancement (ADiRA) – Synopsis (Speaker Dr Ravinandan B B)
The session explored how healthcare systems can strengthen their foundational preparedness to safely and effectively adopt artificial intelligence at scale. The discussion highlighted the essential components of digital readiness, including interoperable data systems, workforce skilling, governance structures, and alignment with national digital health standards. Speakers emphasized that AI maturity evolves in stages, from exploratory pilots to fully integrated clinical and operational tools, requiring high quality datasets, robust validation processes, and human in the loop oversight. The session showcased examples of AI enabled diagnostics, operational optimization, and remote care expansion, while underscoring the importance of ethical guardrails, transparency, and continuous monitoring to prevent bias and ensure safety. ADiRA was positioned as a strategic framework to help institutions move from fragmented digital initiatives toward cohesive, resilient, and scalable AI enabled healthcare ecosystems.
AI in Healthcare from Idea to FDA cleared device, what healthcare professionals need to know – Synopsis (Speaker Dr. Shahir)
The session on AI in Healthcare from Idea to FDA Cleared Device provided a structured overview of how an artificial intelligence concept progresses into a clinically validated and regulator approved medical product. Speakers explained the complete development pathway, beginning with problem identification, data selection, and model design, followed by clinical relevance testing, bias reduction strategies, and real world evidence generation. The discussion highlighted the essential requirements for safety, accuracy, transparency, and reproducibility that healthcare professionals must understand when engaging with AI tools. Participants gained insight into documentation standards, performance benchmarks, risk categorisation, and the regulatory submission process that leads to clearance by the Food and Drug Administration. The session reinforced that clinical users play a central role in shaping reliable AI solutions through domain expertise, continuous feedback, ethical vigilance, and responsible deployment in patient care.
AI prompting for Health research – Synopsis (Speaker Dr. Arti Pawaria)
The session on AI Prompting for Health Research explored how structured prompting techniques can enhance the quality, speed, and depth of scientific inquiry in the health domain. Speakers discussed the fundamentals of crafting precise prompts that guide artificial intelligence systems to generate more reliable literature scans, research summaries, study designs, data interpretations, and grant concepts. The session highlighted the importance of domain context, incremental refinement, and verification strategies to ensure that AI assisted outputs remain accurate and aligned with scientific standards. Participants were introduced to practical examples where effective prompting improved research productivity, supported observational and clinical study planning, and accelerated systematic review preparation. The session emphasized that while AI can significantly augment research capacity, thoughtful prompting and rigorous human oversight remain essential to ensure validity, reproducibility, and ethical integrity in health research.
Delegate Discussion in WorkshopDelegates Hands on experience working on Mobile
Day 1 | 28 November 2025
Scientific Session were scheduled in 4 parallel sessions ( Main hall, Hall A , B and C)
Scientific Session 1
Time: 09:30 AM – 10:30 AM
Topic: Telemedicine in India: 25 Years of Innovation — The Idea, Efforts, Impact, Lessons, and Challenges
Session Chair: Dr. Meenu Singh
Session Co-Chair / Moderator: Dr. Murthy Remilla
Panel Members: Dr. G. Madhavan Nair, Dr. Meenu Singh, Prof. K. Ganapathy, Mr. L. S. Satyamurthy, Prof. Biswa N. Mohanty, Prof. K. Selvakumar, Mr. A. Bhaskaranarayana
Session Highlights and Key Takeaways
The inaugural scientific session of TELEMEDICON 2025 provided a reflective and forward-looking overview of India’s 25-year journey in telemedicine, tracing its evolution from conceptual innovation to a nationally embedded healthcare delivery mechanism.
The session opened with reflections on India’s rapid digital transformation, emphasizing how deliberations and knowledge exchange at successive Telemedicon conferences have played a pivotal role in shaping national telehealth priorities and policy directions.
Panellists revisited the early years of telemedicine in India, marked by technological curiosity, institutional experimentation, and visionary leadership. The discussion highlighted the gradual expansion of telemedicine applications, the increasing integration of artificial intelligence, and the growing involvement of young professionals who are now driving innovation in digital health.
A significant focus was placed on the multi-institutional collaborations that laid the foundation for India’s telemedicine infrastructure. These partnerships enabled early connectivity, remote consultations, and technology-enabled care delivery across challenging geographies.
The COVID-19 pandemic was acknowledged as a watershed moment that dramatically accelerated the acceptance, adoption, and scaling of telemedicine services across the country, transforming telehealth from an alternative model into a mainstream component of healthcare delivery.
National initiatives such as e-Sanjeevani, drone-enabled medical logistics, and satellite-supported connectivity were discussed as examples of how digital health solutions are extending care to underserved and remote populations, with panelists noting the relatively low incidence of medico-legal challenges to date.
The foundational role of ISRO in enabling telemedicine systems was strongly emphasized, along with discussions on the need for cost-effective service models, robotics integration, and continuous strengthening of digital health infrastructure to support future growth.
Improvements in rural–urban connectivity, long-standing ISRO–Telemedicon collaborations, and successful remote healthcare and supply chain operations in geographically isolated regions were presented as tangible evidence of telemedicine’s sustained national impact.
The session concluded with a forward-looking vision, calling for structured telemedicine education and training, greater institutional investment, AI-supported diagnostics, and insurance-linked sustainability models to ensure that digital healthcare in India remains equitable, scalable, and resilient.
Telemedicine in India: 25 Years of Innovation — The Idea, Efforts, Impact, Lessons, and Challenges
Scientific Session 2
Time: 10:35 AM – 11:35 AM
Tele-ICU
Session Chair: Dr. Raj Raval
Panel Members: Mr. R. G. Ajay Prakash, Mr. Atul
Session Highlights and Key Takeaways
The second scientific session of Day 1 focused on Tele-ICU as a critical pillar of India’s evolving digital health ecosystem, particularly in the context of increasing critical-care demand and uneven distribution of specialist resources.
The discussion began by assessing Tele-ICU within India’s expanding digital critical-care landscape, emphasizing how centralized command centres are redefining intensive care delivery. Panelists highlighted the relevance of Tele-ICU models in high-burden and resource-constrained settings, where access to intensivists and advanced monitoring remains limited.
Early implementation experiences were shared, outlining challenges such as technical instability, network reliability issues, and operational complexities in scaling remote ICU services. These early hurdles were presented as valuable learning points that have since contributed to the development of more robust, resilient, and standardized Tele-ICU infrastructures.
The Command Centre model was described as an integrated digital ecosystem, where consolidated clinical dashboards enable real-time access to ECG streams, radiology reports, ventilator parameters, and vital signs. This integration supports timely clinical decision-making, continuous remote supervision, and proactive intervention by specialist teams. Panelists emphasized the growing national demand for digital healthcare infrastructure across hospitals, academic institutions, and public health systems, particularly as healthcare facilities face rising patient loads, workforce constraints, and operational pressures.
Tele-ICU was presented as a scalable response to system-wide challenges, including clinician burnout, rapid expansion of medical knowledge, and projected shortages in the critical-care workforce. Real-world examples of Tele-ICU deployment demonstrated improvements in patient outcomes, faster escalation of care, and optimized utilization of critical resources.
The discussion also explored rural Tele-ICU models and the role of public–private partnerships in extending advanced critical-care monitoring and specialist support to underserved and remote regions.
The session concluded with forward-looking insights on the future of Tele-ICU in India, highlighting the need for government-aligned implementation models, standardized data and interoperability practices, strengthened cybersecurity frameworks, structured workforce training—particularly for nursing and allied health professionals—and evolving medico-legal guidelines to support documentation, accountability, and quality assurance in remote critical care.
Panel Discussion on Tele ICU Dr Raj Raval and Mr. R. G. Ajay Prakash
Inaugural Session
Time: 11:35 AM – 01:30 PM
Inaugural Ceremony – TELEMEDICON 2025
The Inaugural Ceremony of TELEMEDICON 2025 was conducted with dignity and a strong sense of purpose, setting the tone for the conference’s academic and societal vision.
The programme commenced with a Welcome followed by the Karnataka State Anthem, symbolizing regional pride and cultural grounding. This was followed by the Welcome Address delivered by the Organizing Chair, Dr. Uma Nambiar, who outlined the vision, objectives, and thematic focus of TELEMEDICON 2025.
The ceremonial Lamp Lighting by the dignitaries marked the formal inauguration of the conference, signifying knowledge, enlightenment, and collective commitment to advancing telemedicine and digital health.
The Chief Guest Address was delivered by Dr. Sunil Kumar Barnwal, IAS, who highlighted the critical role of digital health and telemedicine in strengthening healthcare systems, improving access, and supporting public health governance in India.
This was followed by the Presentation of the Annual Report by Dr. Umashankar S, providing an overview of the Society’s activities, milestones, and achievements over the past year.
The Presidential Address by Dr. Prem Nair reflected on the strategic direction of the Telemedicine Society of India, emphasizing innovation, sustainability, and collaboration in the evolving digital health ecosystem.
A special moment of recognition followed with the Honouring of the Past President, Dr. Meenu Singh, acknowledging her leadership, contributions, and enduring impact on the Society and the field of telemedicine.
The ceremony concluded with a heartfelt Vote of Thanks proposed by Dr. Bhaskar Rajkumar, expressing gratitude to the dignitaries, speakers, organizers, partners, and participants for their support and presence.
The National Anthem marked the formal closure of the inaugural session, after which delegates proceeded for Lunch.
Delegates raised for Karnataka AnthemDr. Uma Nambiar, Conference Chair Welcoming the DelegatesChief Guest Shir Sunil Kumar Barnwal, IAS Inaugurating the conference by lighting the lampDignitaries from left to right, Dr. Umashankar S, Dr. Uma Nambiar, Dr. Prem Nair, Shri Sunil Kumar Barnwal, Dr. Bhaskar Rajkumar
Symbolism of the Ceremonial Plant Watering
The ceremonial watering of plants by the dignitaries symbolized TELEMEDICON’s commitment to sustainability as a living practice rather than a symbolic gesture. It reflected the collective responsibility of policymakers, clinicians, technologists, and institutions to nurture innovation with care, ensuring that digital health solutions grow in harmony with environmental stewardship, ethical governance, and social responsibility.
Just as a plant requires continuous attention to thrive, the act represented the belief that sustainable healthcare systems must be patiently cultivated, protected, and strengthened over time—through collaboration, foresight, and accountability. This moment embodied TELEMEDICON’s vision of planting ideas today that will grow into resilient, patient-centric digital healthcare for future generations.
Shri Sunil Kumar Barnwal declaring the conference openRelease of TSI Newsletter by dignitaries
Keynote Address
Dr. Sunil Kumar Barnwal, IAS
In his keynote address, Dr. Sunil Kumar Barnwal, IAS, articulated a clear strategic vision for digital health as a foundational enabler of equitable, efficient, and resilient healthcare systems. He emphasized the critical role of technology in strengthening health governance, enhancing last-mile service delivery, and enabling data-driven decision-making across public health programmes.
Highlighting national initiatives in telemedicine, digital health platforms, and system integration, Dr. Barnwal stressed the importance of interoperability, scalability, and ethical deployment of digital tools. He concluded by underscoring the need for sustained and meaningful collaboration among government, clinicians, technologists, and innovators to ensure that digital health solutions translate into measurable population-level impact and long-term system strengthening.
Felicitation of Dr. Meenu Singh, Past President of TSI,Dr. Prem Nair, Presidential AddressFelicitation of Chief Guest
Session 3 Timing: 2:00 PM – 3:00 PM
Topic: Democratization Using AI – First Strategy
Session Chair : Dr. Sanjay Sharma
Session Co-Chair / Moderator: Dr. Karthik Ramesh
Panel Members : Mr. Praveen, Mr. Srini, Dr. Gaurav Raina, Mr. Kiran
Proceedings & Key Takeaways
The session examined how AI-first strategies have the potential to democratize healthcare delivery at scale, drawing on practical models emerging from the Sri Sathya Sai healthcare ecosystem. The discussion opened by positioning artificial intelligence as a critical enabler of equity, efficiency, and system-wide scalability, particularly in complex, high-demand clinical domains.
Panelists explored the integration of AI across the entire surgical continuum—from pre-operative risk stratification and planning, to intra-operative decision support, and post-operative monitoring. Applications of predictive analytics, real-time data interpretation, and workflow automation were highlighted as key contributors to improved clinical outcomes and optimized cardiac surgical pathways.
A significant portion of the discussion focused on regulatory and governance challenges within India’s evolving AI healthcare landscape. The panel emphasized the urgent need for standardized regulatory frameworks, enforceable compliance mechanisms, and alignment with national digital health guidelines to ensure safety, transparency, accountability, and ethical deployment of AI-driven solutions.
Innovations in healthcare software and digital platforms were showcased, including systems that enable real-time surgery streaming for medical education, remote intra-operative assistance, and structured skill transfer. These tools were described as powerful enablers for expanding access to specialist expertise beyond traditional geographical and institutional boundaries.
The panel also highlighted TRANIC, a digital-first initiative aimed at democratizing access to quality healthcare through scalable AI-driven clinical decision-support systems. The model was presented as a viable approach for standardizing care delivery in remote, underserved, and low-resource settings, while maintaining quality and consistency.
In addition, the session showcased next-generation indigenous medical technologies, notably the IIT Madras–developed heart–lung machine. Its affordability, locally optimized design, and suitability for widespread deployment were underscored as strong examples of how homegrown innovation can enhance surgical capacity, reduce dependency on expensive imports, and strengthen national health systems.
Panel discussion on Democratization Using AI – First Strategy
Session 4 Timing: 3:05PM to 4:05 PM
Topics: AI in Action and Decision Making: – AI in Gastro – AI Transforming Transplant Medicine: From Matching to Monitoring – AI in Nephrology – Click when possible, brick when required – Telehealth in Orthopaedics
Session Chair : Dr Sundar Swaminathan
Session Co-Chair / Moderator : Dr. Arvind Ranganathan
Panel Members: Dr GV Rao, Dr Shyam Vasudev Rao, Dr Sunil Shroff, Dr. P Srinivas
Proceedings 3P Model of Patient Care & Telehealth in Orthopaedics
Speaker: Dr. P. Srinivas
Dr. P. Srinivas presented the 3P Model of patient care—Preventive Care, Precision Medicine, and Personalised Therapy—as the emerging framework for future-ready orthopaedic practice. He emphasized how telehealth and digital tools are enabling a shift from episodic treatment to continuous, data-driven musculoskeletal care.
Drawing parallels from the PM National Dialysis Programme implemented under a Public–Private Partnership (PPP) model, Dr. Srinivas highlighted how centralized digital systems can significantly reduce treatment costs and patient travel burden, while improving access and standardization of care.
Within orthopaedics, he showcased recent advancements including AI-based gait analysis, digital posture assessment systems, and range-of-motion (ROM) evaluation tools, demonstrating how objective digital assessments can enhance clinical decision-making. The session concluded by underscoring the growing potential of protocol-driven remote assessments, AI-assisted musculoskeletal diagnostics, and digitally supported rehabilitation pathways, positioning telehealth as an essential and complementary component of modern orthopaedic care.
AI in Organ Donation & Transplant Decision Support
Speaker: Dr. Sunil Shroff
Dr. Sunil Shroff addressed the expanding scope of organ donation and transplantation in India, highlighting the increasing complexity of donor–recipient coordination and long-term post-transplant care. He emphasized the transformative role of artificial intelligence in streamlining transplant workflows and supporting clinical decision-making.
Key insights included the use of AI for predicting transplant outcomes, improving donor–recipient matching accuracy, and enhancing long-term graft survival monitoring. He also discussed AI-enabled early detection of renal diseases such as chronic kidney disease (CKD) and IgA nephropathy, supported by FDA-approved biomarkers, along with applications in renal pathology analytics and dialysis data interpretation.
A major highlight was the AI-PREDICT project (2008–2022), implemented across healthcare systems in the United States and the United Kingdom, which demonstrated strong predictive capabilities for transplant outcomes and contributed to improved patient stratification, follow-up planning, and overall transplant management.
AI in Nephrology – Renalyx Platform & Digital Kidney Care
Speaker: Dr. Shyam Vasudev Rao
Dr. Shyam Vasudev Rao presented the Renalyx digital nephrology platform, illustrating how AI-enabled systems are supporting the full continuum of kidney care—from prevention and early detection to remote monitoring and long-term disease management.
Key components of the platform include home-based early detection kits, mobile app–enabled data uploads for remote nephrologist review, and smart dialysis machines transmitting real-time vital parameters via Bluetooth. The system enables instant alerts to nephrologists, particularly during dialysis sessions when rapid blood pressure fluctuations or other critical events occur.
The Renalyx platform integrates remote patient monitoring, EMR interoperability, teleconsultation modules, third-party medical device connectivity, cloud-based clinical decision support, dialysis centre automation, and real-time clinician dashboards. Dr. Shyam emphasized that the platform is designed to deliver continuous, data-driven kidney care, bridging access gaps and ensuring consistent clinical oversight across multiple dialysis centres and care settings.
Session chair Dr Sundar Swaminathan and Co- Chair Dr. Arvind Ranganathan
TSI AGM Members ParticipatedTSI EC Members 2025-2027 From Left to Right Mr.D Satheesh Kumar, Dr, Murthy Remilla, Dr.Chandil Kumar, Dr. Uma Nambiar, Dr. Sunil Shorff, Dr. Prem Nair, Dr. Krishna Kumar, Dr. Raj Raval, Dr. S Raghavan, Dr. Umashankar S, Mr. Katta Uma Mahesh
TELEMEDICON 2025: Setting a New Benchmark for Sustainable Medical Conferences in India
Prof. (Dr) Umashankar S. Managing Director, Arogyayati Pvt Ltd | Honorary Secretary, Telemedicine Society of India
Large medical and technical conferences are traditionally resource-intensive, generating significant plastic waste, paper consumption, and carbon emissions.
As conference organizers, we have always focused on academic excellence, innovation, and meaningful collaboration. But while planning TELEMEDICON 2025, we paused to ask ourselves a simple question: Can we host a large medical conference without leaving a large environmental footprint?
What followed was a collective decision—to do things differently.
TELEMEDICON 2025, we not only focused for its scientific excellence, but we also consciously embedded commitment to sustainability into every stage of planning and execution. Through a series of deliberate, measurable interventions, the conference demonstrated that large-scale academic events can be both impactful and environmentally responsible. Aligned with the theme “Digital Health for a Sustainable Future,” the conference translated intent into action through thoughtful, measurable, and symbolic green practices.
Small Choices, Big Responsibility With over 700 delegates attending over four days, we knew the scale of our conference could easily translate into significant waste. Plastic badges, bottles, banners, printed books, giveaways—these are often accepted as “standard” conference items. This time, we chose to challenge that standard. One of the most significant steps taken was the near-total elimination of single-use plastics.
We replaced plastic printed lanyards with seed-paper lanyards and cotton tags without branding. Plastic pens were swapped for seed-paper pens. Polyester laptop bags were replaced with reusable cotton bags. Even our mementos were rethought—250 plastic mementos were replaced with thoughtfully crafted wooden ones from the local artisans. This single decision alone prevented 125 kg of plastic from entering the waste stream.
These weren’t just symbolic gestures; they were conscious decisions to reduce plastic at the source.
Saying No to Single-Use Plastics One of our strongest commitments was to eliminate single-use plastics wherever possible. We completely avoided plastic water bottles, cups, plates, and cutlery, we avoided the consumption of approximately 28,800 plastic bottles over four days. Instead, water was served through reusable systems, and participants were to refill their steel water bottles provided in the conference kit. Meals and beverages were served using reusable plates, cups, and cutlery, preventing over 10,000 disposable items from being generated.
Over four days, this single decision alone prevented tens of thousands of plastic items from being used once and thrown away. Food waste management followed a circular approach, food waste, instead of ending up in landfills, was responsibly diverted to piggeries.
Floral waste from the stage decorations during the inauguration was handed to people who wanted to take them and rest were composted. Even the symbolic act of watering plants during inauguration had a long-term impact, as these plants were later transplanted to appropriate locations.
Rethinking Banners, Branding, and Visibility Anyone who has organized a conference knows how much branding material is involved. Traditionally, this means PVC flex banners, large, colourful, difficult to recycle and almost always destined for landfills. We chose another path.
All our exhibition stall backdrops and large banners, some as big as 100 feet by 30 feet, were made using cloth. These banners are reusable, durable, and far kinder to the environment. By doing this, we avoided nearly one to one-and-a-half tonnes of PVC waste and significantly reduced microplastic pollution associated with flex materials.
Collectively, these substitutions eliminated tens of thousands of plastic items and contributed substantially to carbon reduction.
Going Digital to Save Paper and Trees We also made a deliberate shift to digital communication- A major contributor to the conference’s environmental savings was the transition to digital communication. Instead of printing 1,000 conference program booklets of 50 pages each and 10,000 brochures, we used QR codes and digital access.
This saved over 100,000 sheets of paper—equivalent to preserving more than a dozen mature trees—and conserved tens of thousands of litres of water that would otherwise be used in paper production. Delegates adapted quickly, and many appreciated the convenience of digital access.
Greener Movement, Even in Small Ways Transportation was another area where we made conscious choices. We used electric buses instead of diesel buses for delegate movement. While the distance covered was modest, it reflected our belief that sustainability is built through consistent, intentional decisions—big and small.
E-Waste Responsibility in the Digital Era Acknowledging the environmental footprint of digital technologies, at Telemedicon 2025 we organised a dedicated e-waste collection drive, encouraging delegates to bring their e-waste and responsibly dispose of their obsolete electronic devices at designated box at the conference venue, we had collaborated an waste management organization to hand over the collected e-wate to authorised recyclers.
What Did All This Achieve? When we added everything together, the impact surprised even us.
By rethinking materials, eliminating single-use plastics, avoiding flex banners, reducing printing, and choosing sustainable alternatives, TELEMEDICON 2025 avoided approximately 5 tonnes of carbon dioxide emissions.
To put that in perspective, this is equivalent to:
Planting over 220 trees and nurturing them for a year
Avoiding 20,000 km of travel in a petrol-powered car
Preventing the combustion of nearly 1,850 liters of diesel or petrol
Eliminating plastic waste equivalent to what 80 households generate in a month
In addition, the conference:
Avoided over 125 kg of solid plastic from mementos alone
Prevented tens of thousands of plastic items from entering landfills
Conserved over 130,000 Liters of water
Achieved a near zero-waste conference model
What This Means to Us For us, sustainability was not about perfection—it was about intention. We learned that sustainable choices are possible without compromising quality, delegate experience, or professional standards. In fact, many participants told us that these efforts made the conference feel more meaningful and responsible
Beyond an Event — A Sustainability Legacy Telemedicon 2025 demonstrated that sustainability can be seamlessly integrated into large-scale professional events without compromising experience or excellence. Scientific conferences can be platforms not only for knowledge exchange but also for climate leadership. As healthcare professionals, we speak often about prevention and long-term wellbeing. Extending that philosophy to planetary health felt both natural and necessary. We hope our experience encourages other conferences, institutions, and professional bodies to take similar steps. Because when enough of us make small changes, the collective impact can be truly transformative.
Telemedicon 2025 leaves behind more than memories and knowledge; it leaves a blueprint for sustainable conferences of the future – Transformation by example.
Delegation Visit to Narayana Health: A Ringside View of Digital Adoption in Patient‑Centric Care and Use Cases
Rajarajan S Group COO, Hospitals – Alluri Sitarama Raju Academy of Medical Sciences, Executive Committee Member, Telemedicine Society of India (TSI) – Tamil Nadu and Core Member, Scientific Committee – Telemedicon 2025
As part of Telemedicon 2025 held at the Indian Institute of Science (IISc), Bengaluru, a distinguished delegation of clinicians, technologists, policy makers and digital health leaders visited Narayana Health (NH), Bengaluru, in line with the theme of the conference “Digital Health for a Sustainable Future”. The visit offered a firsthand view of NH’s digital adoption journey and its impact on patient experience, clinical workflows and operational efficiency.
Telemedicine and Digital Health in India India’s healthcare system is undergoing rapid digital transformation, driven by telemedicine, electronic medical records, AI-enabled analytics and integrated patient engagement platforms. Narayana Health has emerged as a national leader by embedding digital tools across its multi-hospital ecosystem.
Patient-Centric Digital Front End A major highlight of the visit was the live demonstration of NH’s Digital Kiosks and Queue Management Systems. Patients can book appointments, make payments, select consultation slots and receive queue tokens independently. This has significantly reduced waiting times and dependence on manual front desks.
Clinical Workflow Digitisation Delegates were introduced to NH’s integrated digital platforms, such as ATHMA and AADI, supporting one-page EMR, CPOE, nursing automation, incident reporting, discharge summaries and real-time patient monitoring. AI-powered tools like AIRA further reduce documentation burden on clinicians.
Analytics, AI and Decision Support NH leverages advanced analytics and AI to monitor operational KPIs, predict patient volumes and optimise clinical workflows. Real-time dashboards enable leadership to take data-driven decisions, improving outcomes and efficiency.
Integrated Patient Engagement The NH Care mobile and web platforms allow patients to book appointments, access reports and interact seamlessly with the hospital. Cloud-based CRM and communication platforms handle large-scale patient interactions efficiently.
Telemedicine and Remote Care Narayana Health continues to expand telemedicine, remote diagnostics and specialist consultations through digital partnerships, supporting outreach to tier-2, tier-3 and rural regions.
Key Learnings
Patient experience must be central to digital design
AI can meaningfully reduce clinician administrative burden
Data-driven operations improve efficiency and quality
The Telemedicon 2025 delegation visit to Narayana Health showcased how purposeful digital adoption can transform healthcare delivery. NH’s journey provides a replicable model for healthcare organisations aiming to scale telemedicine and digital health sustainably.
AIIMS Jammu: Digital Transformation in the making
Dr. K. Ganapathy Distinguished Visiting Professor IIT Kanpur | Distinguished Professor The Tamilnadu Dr MGR Medical University | Emeritus Professor National Academy of Medical Sciences | Past President : Telemedicine Society of India, Neurological Society of India, Indian Society for Stereotactic & Functional Neurosurgery | Formerly WHO Digital Health Expert | Former Director Apollo Telemedicine Networking Foundation & Apollo Tele Health Services
During the last fifty years I have had the opportunity to visit a number of Healthcare institutions in India and some overseas. In the last 25 years as a Digital Health evangelist I have in my own small way, trying my best to “sell’ the concept of Digital Health in its entirety. As a visiting faculty to AIIMS J it was my privilege to spend a full week there. A few weeks later while on a visit to IIM Jammu I again visited AIIMS J. It was most reassuring to experience at first hand the incredible journey of AIIMSJ to make this National Institute paperless. I am sure this is going to happen in my lifetime!! This visit was trying to convert the converted!
The website says it all!! It is eHRMS, e Office, HMIS all the way. Click on https://epravah.prd.dcservices.in/AHIMSG5/hissso/Login and you realise that we are in the era of ePravah, electronic pay roll and Accounting HR system.
Click on https://play.google.com/store/apps/details?id=com.iwayplus.aiimsjammu&hl=en_IN&pli=1 (Updated on 12 Dec 2025) and you land on AIIMS Jammu Swasthya. This app can be used by doctors and patients of AIIMS J. Patients can register in the app, book, cancel or reschedule appointments, view hospital OPD, lab and tariff enquiries. Doctors can login to the app using their credentials and access the web view for OPD LITE, and view enquiry information for OPD, lab and tariffs.
The Indoor Navigator Appears to be the ultimate solution for finding your way around complex indoor environments with ease. Navigator app ensures you never lose your way even in this large hospital. AIIMS Jammu Kiosk is an interactive venue navigation and mapping solution designed for AIIMS J. This self-service kiosk helps visitors easily find locations, get step-by-step directions, and explore venue facilities with an intuitive touchscreen interface.
The eLibrary could not be more modern and state of the art. RFID tagged books and journals ensures that an alarm is set off. If there is any unauthorised removal. Instant access to tens of thousands of publications immediately available on large screens makes knowledge acquisition totally different. There is even a children’s section for children of faculty and staff!
The OPD has a separate section for senior citizens. Interestingly there is a counter for those aged 60 to 70 and another counter for those above 70 years!! With all the digitisation there is still a human being at these counters to help those not fully digitally literate. As one belonging to the BC era, trained in the 20th century. I am always concerned that deployment of technology may be at the cost of establishing human rapport. AIIMS J is addressing this as well! This sign board says it all. One has to search for the doctor here!
Thank you Lt Gen Narayanan President Governing Council AIIMS Jammu and Dr Shakti Kumar Gupta the first Executive Director and CEO of AIIMS Jammu for facilitating this “ awesome” experience! As highlighted https://statetimes.in/i-am-in-love-with-aiims-jammu-says-dr-krishnan-ganapathy/ I have indeed fallen in love with this institution. They have no legacy systems to disinherit. A dynamic, passionate, future ready leadership can make all the difference supported by young faculty inspired by their seniors.
With students after a classWith Director & Faculty
Report on the Inaugural Ceremony of the Telemedicine Society of India (TSI) – Kerala Chapter Student Wing
The Department of Biomedical Engineering, TKM Institute of Technology (TKMIT), successfully organized the Inaugural Ceremony of the Telemedicine Society of India (TSI) Kerala Chapter Student Wing on 16th December 2025, from 2:30 PM to 4:00 PM, at the Seminar Hall, Administrative Block, TKMIT. The programme marked a significant milestone in strengthening academic, industry and clinical collaboration in the domain of telemedicine, digital health, and biomedical innovation, while formally launching the TSI Student Wing at TKMIT.
Commencement of the Programme The event commenced at 2:30 PM with a prayer, invoking blessings for the success of the newly established student wing and its future initiatives. This was followed by the Welcome Address delivered by Dr. Muhammed Shafeeque Rahman P P, HoD and Associate Professor, Department of Biomedical Engineering, TKMIT. In his address, he highlighted the relevance of telemedicine in modern healthcare, the importance of interdisciplinary learning, and the role of professional bodies like TSI in shaping future-ready biomedical engineers. The Presidential Address was delivered by Dr. Gouri Mohan L, Principal, TKM Institute of Technology, who emphasized the institution’s commitment to promoting professional societies, research culture, and student engagement in emerging healthcare technologies. The formal inauguration of the TSI Kerala Chapter Student Wing at TKMIT was carried out by Dr. Vivek Nambiar, Neurologist, Amrita Hospital, and President, TSI Kerala State Chapter. In his inaugural address, he provided valuable insights into the evolution of telemedicine, its growing impact on healthcare delivery, and the immense opportunities available for students in the areas of digital health, AI-driven healthcare, and remote medical services. The Felicitation Ceremony was held at 3:10 PM, recognizing distinguished guests and contributors.
The felicitation session was graced by eminent personalities including: Mr. Bijoy M G, MD – UNARV Telemedicine and Immediate Past Secretary, TSI Kerala State Chapter, Dr. Pradeep Thomas, HoD – Emergency Medicine, KIMS Valiyath Hospital and Executive Committee Member, TSI Kerala State Chapter, Dr. Raghavan S, National Executive Member, TSI and Professor, Department of Electronics and Communication Engineering, NIT Tiruchirappalli, who was also present during the felicitation ceremony, adding academic distinction and national-level expertise to the event. Their presence reinforced the strong academic, clinical, and industry linkage promoted through the TSI platform.
Introduction of Student Wing Office Bearers At 3:35 PM, Dr. Nitha V Panicker, Secretary, TSI Kerala State Chapter and Dr. Raghavan S, formally introduced the TKMIT–TSI Student Wing Office Bearers, outlining their roles and responsibilities in driving student-led activities, workshops, outreach programmes, and professional development initiatives under TSI. Mr Muneer (S6 BM), Ms Megha Pillai (S4 BM) and Mr Muhammed (S6 BM) were selected as office bearers of TSI Student Wing office bearers. Dr. Nitha V Panicker administered the oath to the student office bearers. Special Appreciation Awards were presented to students and faculty members who successfully cleared NPTEL examinations. This recognition acknowledged their commitment to continuous learning, academic excellence, and skill enhancement through national-level certification platforms. The awards served as motivation for the student community to actively engage in MOOCs, professional certifications, and lifelong learning.
The programme concluded with a Vote of Thanks delivered by Ms. Trissa Rose, Vice-President, BLAZE Association, TKMIT, who expressed gratitude to the dignitaries, organizers, faculty members, students, and volunteers for their collective efforts in making the event a grand success. The inaugural ceremony successfully laid a strong foundation for the TSI Kerala Chapter Student Wing at TKMIT, fostering a platform for collaboration, innovation, and professional growth in telemedicine and digital healthcare. The event reinforced TKMIT’s commitment to industry engagement, research orientation, and holistic student development.
A new personality test reveals how AI chatbots mimic human traits—and how their behavior can be shaped or manipulated…………… Read More
Can AI Personalize Ventilation for ARDS Patients?
Researchers say ARDS is an ideal condition to test AI-guided ventilation due to its complexity, varied patient responses, and high death rates………………. Read More
TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Telemedicine Society of India
What is New?
The November issue of our newsletter features the tentative program for TELEMEDICON 2025 – a power-packed three-day event that brings together the entire digital health ecosystem. The Telemedicine Society of India (TSI), now 25 years strong, has grown into a vibrant national body with over 1,200 members and 20 state chapters. It remains the only registered society in this domain, offering an inclusive and truly democratic platform for digital health professionals.
In recent years, India has witnessed several digital health initiatives emerging from individual efforts rather than institutional frameworks. While such efforts are commendable, they often have a limited shelf life. In contrast, institutional structures provide the continuity, credibility, and longevity needed to drive sustained impact.
As members of TSI, it is time for us to reflect and elevate our collective vision. We must ask ourselves-not what the society can do for us, but what we can do for the society-echoing the timeless message of John F. Kennedy. Only through unity, shared purpose, and collaborative effort can we propel TSI to greater heights. United, we progress; divided, we diminish. This is the moment for TSI to stand cohesive and strong.
We warmly welcome you to Bangalore in large numbers to celebrate this milestone and to make your society proud as it marks its 25-year journey.
Thank You Dr. Sunil Shroff Chief Editor President-Elect, TSI
A Free Medical Camp conducted at Niravilpuzha Keloth Unnathi Wayanad
Dr. Sreekumar C MS Professor, Department of General Surgery Amrita Institute of Medical Sciences (AIMS), Kochi Chief Medical Officer – Telemedicine Camps
A Free Medical Camp for Tribals was conducted on November 16th 2025 at Niravilpuzha Keloth Unnathi Wayanad for Tribal people in Collaboration with Amrita Institute of Medical Science Kochi, Kerala Forest Office and Wildlife Department – North Wayanad Division (Snehahastham Project) , Amrita Telemedicine Unit, Tele Medicine Society of India Kerala Chapters, Amrita Kripa Charitable Hospital.
A total of 160 patients Exclusively From Tribal Community were Evaluated and consulted. Along with the Medical Faculties, Dietitians, Psychological Counsellor, MBBS Students from AIMS Kochi Campus also Participated in this Program. Including that Telemedicine Consultation was also Conducted. Detailed Health Checkup, Health Education, Nutritional Evaluation and Medicine Distribution was Done.
The session was Inauguration by Renjithkumar S Range Forest Officer, Ms Rose Mary Jose, Range Forest Officer Mananthavady Range joined Virtually.
Dr Sreekumar C Professor Department of General Surgery, Dr Akhilesh K professor Department of Respiratory medicine, Dr Hareesh M D, Dr Ageesh MD, Mr Rajeesh M V (Department Of Telemedicine) and Mr Athul Ajay (Department Of Respiratory Medicine) attended the camp.
Telemedicine A Telemedicine Consultation was done by Dr Akhilesh K Professor Department of Respiratory Medicine and Chief Of Amrita Pulmonary Rehabilitation Clinic. He gave specialised Pulmonary Consultation to patients diagnosed with CRD like COPD, Asthma etc.. He also gave specialised Pulmonary Rehabilitation Consult with the help of realtime PFT reading digitally sent to the hub with the support of Mr Rajeesh M V Telemedicine Administrator Amrita Telemedicine Unit. Amrita Telemedicine Unit provided the support for real-time consultation without any interruption. Health education on Pulmonary care and counseling was Given by Mr Athul Ajay Medical Social Worker and Health educator.
AI Creates First-Ever Drug from Scratch in Record Time
Dr. Ankita Balar Arya BDS Content Writer, Medindia.net
Artificial intelligence has officially crossed from theory into therapy. The world’s first AI-designed drug, Rentosertib, developed by Insilico Medicine, has reached clinical success faster than any traditional medicine ever has—marking a historic shift in how we create and test new treatments.
AI Factories Rewrite the Drug Discovery Playbook Pharmaceutical innovation is being redefined by AI-powered factories that can scan billions of molecular combinations in weeks, not years. Leading biotech firms like Insilico Medicine have built sophisticated platforms-PandaOmics and Chemistry42-that merge bioinformatics, chemistry, and machine learning to pinpoint new drug targets with stunning precision.
This approach led to the creation of Rentosertib, a molecule engineered entirely by AI, from target identification to compound design. The achievement marks the first time in medical history that both a drug and its biological target were discovered using generative AI.
Rentosertib: AI’s First Triumph in Lung Disease The journey began when PandaOmics analyzed vast biological databases and identified the TNIK protein as a key driver in idiopathic pulmonary fibrosis (IPF)-a deadly lung disease with few treatment options. Using Chemistry42, Insilico’s AI built and optimized the molecule Rentosertib in record time.
In a Phase IIa clinical trial involving 71 IPF patients, Rentosertib showed exceptional promise. Over 12 weeks, participants receiving the highest dose (60 mg QD) experienced a mean improvement of 98.4 mL in forced vital capacity (FVC), while those on placebo declined by 62.3 mL. Patients also reported improved quality of life, including less cough and better breathing comfort.
Does AI Really Deliver on Its Promise? Emerging data suggests yes. Recent reviews reveal that AI-generated drugs achieve Phase I success rates of 80–90%, compared to 40-65% with traditional R&D. Cost reductions of up to 70% have been documented, and development timelines have shortened from the usual 10–12 years to just 3-6 years.
These efficiencies come from neural networks capable of predicting how a molecule will behave, how it will bind to its target, and even how different patients may respond. AI also helps optimize clinical trial design, ensuring the right patients receive the right treatments faster than ever before.
A New Age: Can AI Cure What Humans Cannot? Beyond speed and savings, AI holds the potential to tackle diseases where human expertise has failed. The success of Rentosertib signals a paradigm shift-AI can now uncover hidden biological mechanisms and propose entirely new therapeutic strategies.
The industry has taken notice: over $5 billion has already been invested in AI drug discovery, and experts estimate that by 2030, 30% of all new drugs could originate from AI systems.
According to Dr. Alex Zhavoronkov, CEO of Insilico Medicine, “This is just the beginning. AI is not replacing scientists-it’s empowering them to move at light speed.”
As AI continues to evolve, the once-impossible dream of designing precise, patient-tailored therapies is fast becoming reality.
Why AI Pose Risk to Vulnerable Mental Health Users
Accessibility and low cost may be the two factors why people are opting for AI chatbots and wellness apps for emotional support, particularly teen mental health users.
However, American psychological association (APA) warns that AI tools and technological apps could offer a temporary support for mental health and not a direct replace. The health advisory found that wellness apps lack scientific evidence and user safety to cure mental health conditions.
Hence, there is a need for enacting strong data privacy laws, a ban on AI posing as pros, and renovating regulatory policies.
“We are in the midst of a major mental health crisis that requires systemic solutions, not just technological stopgaps,” said APA CEO Arthur C. Evans Jr., PhD.
Beyond the App: Prioritizing Mental Health Care Systems “While chatbots seem readily available to offer users support and validation, the ability of these tools to safely guide someone experiencing crisis is limited and unpredictable.” The advisory emphasizes that while technology has immense potential to help psychologists address the mental health crisis it must not distract from the urgent need to fix the foundations of America’s mental health care system.
The report offers recommendations for the public, policymakers, tech companies, researchers, clinicians, parents, caregivers and other stakeholders to help them understand their role in a rapidly changing technology landscape so that the burden of navigating untested and unregulated digital spaces does not fall solely on users.
Protecting Vulnerable Users from Life-Threatening Harm Due to the unpredictable nature of these technologies, do not use chatbots and wellness apps as a substitute for care from a qualified mental health professional.
Prevent unhealthy relationships or dependencies between users and these technologies.
Establish specific safeguards for children, teens and other vulnerable populations.
“The development of AI technologies has outpaced our ability to fully understand their effects and capabilities. As a result, we are seeing reports of significant harm done to adolescents and other vulnerable populations,” Evans said.
“For some, this can be life-threatening, underscoring the need for psychologists and psychological science to be involved at every stage of the development process.”
Why AI Requires Scientific Validation Even generative AI tools that have been developed with high-quality psychological science and using best practices do not have enough evidence to show that they are effective or safe to use in mental health care, according to the advisory.
Researchers must evaluate generative AI chatbots and wellness apps using randomized clinical trials and longitudinal studies that track outcomes over time. But in order to do so, tech companies and policymakers must commit to transparency on how these technologies are being created and used.
Calling the current regulatory frameworks inadequate to address the reality of AI in mental health care, the advisory calls for policymakers, particularly at the federal level, to:
Modernize regulations
Create evidence-based standards for each category of digital tool
Address gaps in Food and Drug Administration oversight
Promote legislation that prohibits AI chatbots from posing as licensed professionals
Enact comprehensive data privacy legislations and “safe-by-default” settings
Role of AI: Supporting Human Professionals, Not Replacing Them The advisory notes many clinicians lack expertise in AI and urges professional groups and health systems to train them on AI, bias, data privacy, and responsible use of AI tools in practice.
Clinicians themselves should also follow the ethical guidance available and proactively ask patients about their use of AI chatbots and wellness apps.
“Artificial intelligence will play a critical role in the future of health care, but it cannot fulfill that promise unless we also confront the long-standing challenges in mental health,” said Evans.
“We must push for systemic reform to make care more affordable, accessible, and timely-and to ensure that human professionals are supported, not replaced, by AI.”
::ANNOUNCEMENTS::
*Note: The above scientific program is tentative only. Sessions timings and speakers may change.
TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Telemedicine Society of India
What is New?
We are gearing up for our annual conference – TELEMEDICON 2025, to be held next month at the Indian Institute of Science, Bangalore. This flagship event continues to blend academics, fellowship, networking, and shared goals in digital health – while also symbolically passing the baton to a new set of leaders.
However, this year’s election process has raised some concerns. Despite having an electronic voting system in place, there was limited enthusiasm among members to contest for executive committee positions – with fewer than four nominations for seven posts received. For a society of 1,600 members and 20 state chapters, this trend calls for serious introspection.
This issue features some insightful articles including AI Curtain Raiser Summit at IIM Ahmedabad, offering a glimpse into the upcoming AI Impact Summit scheduled for February 2026 in Delhi.
We look forward to meeting all of you at TELEMEDICON 2025!
Thank You Dr. Sunil Shroff Chief Editor President-Elect, TSI
An Ingenious AI Discovery in Antibiotics for Crohn’s Disease
A novel antibiotic drug, enterololin, can attack a definite group of disease-causing bacteria including the strains ofE.coli that navigate Crohn’s disease. At present, as there is no cure available for inflammatory bowel diseases (IBD), this latest drug offers a promising treatment option.
An innovative AI tool could predict the drug’s mode of attack on the specific protein complex called LolCDE, representing a significant milestone in IBD drug design. The discoveries were made by researchers at McMaster University and the Massachusetts Institute of Technology (MIT), published in journal Nature Microbiology.
The discovery unveils a promising new treatment option for millions of people affected by Crohn’s disease and other related conditions, while also showcasing important new applications for AI in drug discovery research.
New Antibiotic Attacks Enterobacteriaceae While Preserving Good Bacteria
“This work shows that we’re still just scratching the surface as far as AI-guided drug discovery goes,” says Jon Stokes, an assistant professor in McMaster’s Department of Biochemistry and Biomedical Sciences and principal investigator on the new study.
“The development of our new drug, which is designed to target IBD, has been fast-tracked thanks to the collaboration between humans and generative AI.” Most antibiotics used in clinics today are “broad-spectrum” drugs, meaning they wipe out good bacteria in addition to those that cause disease — “they’re nukes,” Stokes explains. This can create opportunities for invasive and drug-resistant species of bacteria, like E. coli, to move in and colonize the intestines, which can exacerbate conditions like Crohn’s.
But enterololin, the new antibiotic discovered at McMaster, is a “narrow-spectrum” drug, meaning it spares the microbiome and attacks only a specific group of disease-causing bugs — in this case, a family of bacteria called Enterobacteriaceae, which happens to include E. coli. This means it not only kills E. coli, but also reduces the opportunity for drug-resistant strains to colonize the gut in the first place.
AI Predicts Drug Mechanism of Action (MOA) for the First Time
“This new drug is a really promising treatment candidate for the millions of patients living with IBD,” Stokes says. “We currently have no cure for these conditions, so developing something that might meaningfully alleviate symptoms could help people experience a much higher quality of life.”
To date, AI has been leveraged as a tool for predicting which molecules might have therapeutic potential, but this study used it to describe what researchers call “mechanism of action” (MOA) — or how drugs attack disease.
“AI has expedited the rate at which we can explore chemical space for new drug candidates, but, until now, it has done little to alleviate a major bottleneck in drug development, which is understanding what these new drug candidates actually do,” explains Stokes.
AI Pinpoints Enterololin’s Attack on the Target Protein
MOA studies, he says, are essential for drug development. They help scientists confirm safety, optimize dosage, make modifications to improve efficacy, and sometimes even uncover entirely new drug targets. They also help regulators determine whether or not a given drug candidate is suitable for use in humans. But they’re also notoriously expensive — and slow.
Stokes says a thorough MOA study can take up to two years and cost around $2 million; however, using AI, his group did enterololin’s in just six months and for just $60,000.
Indeed, after his lab’s discovery of the new antibiotic, Stokes connected with colleagues at MIT’s Computer Science and Artificial Intelligence Lab (CSAIL) to see if any of their emerging machine learning platforms could help fast-track his upcoming MOA studies.
In just 100 seconds, he was given a prediction: his new drug attacked a microscopic protein complex called LolCDE, which is essential to the survival of certain bacteria.
“A lot of AI use in drug discovery has been about searching chemical space, identifying new molecules that might be active,” says Regina Barzilay, a professor in MIT’s School of Engineering and the developer of DiffDock, the AI model that made the prediction.
Empirical Evidence Proves AI’s Important Prediction
“What we’re showing here is that AI can also provide mechanistic explanations, which are critical for moving a molecule through the development pipeline.” Barzilay was recently listed among Time Magazine’s most influential people in AI. Stokes stresses that while the prediction was intriguing, it was just that — a prediction. He would still have to conduct traditional MOA studies in the lab.
“Currently, we can’t just assume that these AI models are totally right, but the notion that it could be right took the guesswork out of our next steps,” explains Stokes, a member of the Michael G. DeGroote Institute for Infectious Disease Research at McMaster.
And so his team, led in large part by McMaster graduate student Denise Catacutan, began investigating enterololin’s MOA, using MIT’s prediction as a starting point. Within just a few months, it became clear that the AI was in fact right.
AI as a Tool for Fixing Drug Resistance Problem
“We did all of our standard MOA workup to validate the prediction — to see if the experiments would back-up the AI, and they did,” says Catacutan, a PhD candidate in the Stokes Lab. “Doing it this way shaved a year-and-a-half off of our normal timeline.”
With this, Stokes has now successfully used AI to discover viable drug candidates, to fast-track global drug discovery efforts, and to determine how new drugs work. But, ask him, and he’ll tell you that — beneficial as it is — AI is merely a means to an end.
“Drug resistance and our lack of new drugs is a leaky faucet,” he says. “You can leave it be for a while, but you’re eventually going to have a big problem. AI is my wrench — it’s a tool for fixing the leak before it becomes a flood, and that’s really it. My sole focus is on getting new drugs to the patients who need them, and as long as AI can help me do that, then I’ll continue to find new ways to use it.”
Testing Enterololin Against Other Drug-Resistant Bacteria
The pathway to patients Stokes’ spin-out company, Stoked Bio, has already licensed enterololin from McMaster and is currently optimizing it for human use.
The company is also testing modified versions of the new antibiotic against other drug-resistant bacteria, like Klebsiella, and early results are promising.
“The identification of enterololin underscores the remarkable science emerging at McMaster,” says Jeff Skinner, CEO at Stoked Bio. “We are proud to partner with the university on translating this breakthrough into real therapies for patients.”
If all goes well, Stokes says that the new drug will be ready for human trials within three years — a timeline his research team is eager to meet. “Working on something translational like this is surreal,” says Catacutan. “The fact that something we discovered in the lab may someday help patients is truly amazing, and really reinforces the significance of our work.”
Conference on Responsible AI Innovation in Healthcare: A Collaboration between IIM Ahmedabad and CoRE-AI
Meemansa Agarwal Programme Manager, The Dialogue
A two-day conference held on 9th and 10th October, organized jointly by the Centre for Management of Health Services (IIM Ahmedabad) and CoRE-AI (Coalition for the Responsible Evolution of AI), served as a pre-summit event leading up to the AI Impact Summit 2026.
The event brought together clinicians, healthcare providers, academics, and technologists who are developing cutting-edge AI solutions in healthcare. Participants explored synergies between clinical and technological expertise and discussed strategies to accelerate AI adoption in the healthcare sector.
The conference featured four panel discussions on topics including:
The current landscape of AI adoption in India’s healthcare ecosystem and successful use cases.
Barriers preventing AI tools from scaling beyond pilot projects into mainstream clinical practice.
Building the digital infrastructure and leadership capacity required for effective AI integration.
Ensuring equitable access to quality care through responsible AI deployment across rural and urban contexts.
Challenges around data procurement for AI innovation and the role of interoperability and data-sharing standards in scaling AI solutions.
Promoting ethical and responsible AI practices in healthcare.
Additionally, a roundtable discussion brought together clinicians and innovators to explore how both communities can collaborate more effectively. Clinicians voiced concerns over the lack of collaboration, noting that AI development is often concentrated in certain specialties and tends to replace rather than augment clinical expertise. They also highlighted challenges related to bureaucratic hurdles in procuring data and securing support from clinicians, as well as the limited funding for long-gestation projects, which slows meaningful AI development and adoption. The discussion focused on strategies to foster user-centered design, co-development, and responsible adoption of AI in healthcare, aiming to bridge the communication gap between innovators and clinicians.
About the AI Impact Summit 2026:
Hosted by the Ministry of Electronics and Information Technology, the India AI-Impact Summit 2026 will take place on 19–20 February 2026 in New Delhi. The Summit serves as a global platform to highlight AI’s transformative potential in driving inclusive development, sustainability, and equitable progress. It envisions a future where AI advances human well-being, promotes social development, fosters innovation, and safeguards the planet.
The Three Sutras
The Summit will be guided by three core principles:
People: AI should serve all of humanity, respecting diversity, cultural identities, and human dignity, ensuring that no one is left behind. Focus areas include human development in an AI-enabled world, multilingual and accessible systems, and safe, trustworthy deployment.
Planet: AI development and deployment must be resource-efficient and aligned with climate resilience, environmental protection, and scientific advancement, supporting global sustainability and planetary stewardship.
Progress: AI’s benefits should be equitably distributed, with democratized access to datasets, computing power, and models. Applications span critical sectors such as healthcare, education, governance, and agriculture, ensuring that AI drives meaningful societal impact.
From Catheter to Calm: VR Transforms Patient Experience in Heart Care
Patients undergoing coronary angiography—a procedure often performed while the patient is awake—frequently experience anxiety, typically managed with anti-anxiety medications.
VR in Cardiology However, a new analysis presented at the American College of Cardiology (ACC) Middle East 2025, together with the 16th Emirates Cardiac Society Conference, found that virtual reality (VR) can effectively reduce anxiety and stabilize vital signs during the procedure, offering a promising alternative to traditional approaches.
“Virtual reality offers an innovative solution to manage and reduce the anxiety of patients undergoing an interventional cardiovascular procedure, like coronary angiography,” said Yousef Radwan Alnomani, a clinical researcher at Benha University in Egypt and lead author of the study. Coronary angiography is a type of cardiac catheterization that uses catheters and X-rays to detect narrowed or blocked vessels and, if necessary, place stents in the heart’s arteries.
VR’s Effectiveness During Coronary Angiography to Stabilize Vitals Researchers conducted a meta-analysis of five randomized controlled trials involving 451 patients, comparing VR to standard care. The VR interventions featured immersive 3D environments such as waterfalls, mountains, and valleys, designed to promote relaxation. The study found that VR during coronary angiography significantly reduced anxiety and minimized fluctuations in heart rate and blood pressure compared with standard care. In contrast, VR used only before the procedure reduced anxiety but did not significantly stabilize vital signs.
“Immersing patients in a 3D simulation offers better relaxation than simply watching a similar video on a screen,” Alnomani explained.
While the findings are promising, the study is limited by its retrospective nature, and the researchers emphasize the need for larger, randomized controlled trials to confirm VR’s effectiveness and explore its broader use in cardiovascular procedures.
This research underscores the potential of virtual reality to enhance patient experience, reduce procedural anxiety, and improve overall cardiovascular care.
Nanomaterial That Stimulates Brain Cells, Without Surgery Created
Dr. Shanmathi Rajendran BDS Content Writer, Medindia.net
Indian researchers at the Institute of Nano Science and Technology (INST) under the Department of Science and Technology (DST) have come up with a special nanomaterial that stimulates brain cells, without surgery, electrodes, or external devices!
It is a material known as graphitic carbon nitride (g-C₃N₄) and is a smart, biocompatible switch. It reacts to the natural electrical impulses of the brain, which assist the neurons to grow, connect, and work more efficiently.
Healing the Brain Naturally?
Deep Brain Stimulation (DBS) and other similar treatments typically involve the invasive and dangerous implantation of electrodes into the brain. However, g-C₃N₄ functions in a different way. By responding to the active and resting states of neurones, the substance functions as a smart switch, establishing the ideal environment for normal brain activity.
Steps Behind the Stimulation
Cultured Neurons:
Scientists grow brain cells (neurons) in a dish to study how they react to stimulation.
Stimulus and Membrane Potential: Neurons naturally send tiny electrical signals — shown here as a spike in the red line (membrane potential).
Creation of an Electric Field: These voltage changes in the neurons generate an electromagnetic field.
Role of g-C₃N₄ (the Smart Nanomaterial):
The semiconducting material detects and responds to this natural electric field..
When the neuron is at a resting position, it becomes conductive (active), which assists in sending subtle signals to the cells.
Neuronal Response: The electric field generated by g-C₃N₄ triggers the opening of calcium ion (Ca²⁺) channels in the neuron membrane, known as Voltage-Gated Calcium Channels (VGCCs).
Calcium Influx Promotes Better Communication:
The opening of these calcium pores increases the growth of neurons, their connections and communication, which resembles the signaling of the brain itself.
All this happens without implants, magnets, or electrodes — just by placing the nanomaterial near neurons. In laboratory tests, the nanomaterial even enhanced the dopamine formation (which is a major chemical in movement and mood control) and decreased toxic proteins associated with Parkinson’s disease in animal testing.
Can ON-OFF Like Neurons! Researchers found that the material’s behavior changes with the brain’s voltage signals:
In a resting state (−90 mV), the material turns “ON”, gently activating neurons.
In an active state (+55 mV), it switches “OFF”, preventing overstimulation.
The brain’s natural ability to rest when not needed and stimulate when needed is better reflected by this intelligent ON-OFF response. This keeps the brain functioning in a healthy way!
From Brain Healing to Brain Computing This finding could support modern innovations like “brainware computing” in addition to curing illnesses like Parkinson’s and Alzheimer’s.
Brain organoids are tiny lab-grown brain tissues that scientists are testing as biological processors. They could open the door to bio-inspired computers that learn and think more like the human brain when combined with smart semiconductors like g-C3N4
A Step Toward Non-Invasive Brain Therapy “This is the first demonstration of semiconducting nanomaterials directly modulating neurons without external stimulation,” said Dr. Manish Singh, who led the study.
The INST team made the point that, prior to human applications, further preclinical and clinical research is required.
“We believe this marks a paradigm shift in neuromodulation research. “From treating brain injuries to managing neurodegeneration, semiconducting nanomaterials hold immense promise for the future,” Dr Singh added.
The research, published in ACS Applied Materials & Interfaces, marks a paradigm shift in neuromodulation—offering a safer, simpler, and smarter path to treat brain disorders. Scientists believe this nanotech breakthrough could redefine brain medicine and computing in the years to come.
The Future of Brain Healing Lies Not in Wires, But With Smarter Materials that Thinks Like Your Brain!
Toxic E-Waste Linked to High Blood Pressure in Kids
Dr. Nikitha Narayanan MDS Content Writer, Medindia.net
Children living near electronic waste (e-waste) recycling sites may be facing more than just pollution — they’re also at risk of developing high blood pressure, a condition once rare in the young.
A new study published in Environment & Health reveals that children exposed to harmful metals and volatile chemicals from e-waste dumps were about four times more likely to develop hypertension than those in other regions (12.7% vs. 3.1%).
How E-Waste Pollution Affects the Body
E-waste — discarded computers, phones, and other electronics, often release toxic metals like lead, arsenic, and cadmium, along with volatile organic compounds (VOCs) such as benzene and styrene, when dismantled or burned.
These substances can enter the bloodstream and alter key metabolic pathways, especially those linked to the gut and cardiovascular system. The result? Disrupted blood pressure regulation and early signs of hypertension in children.
Inside the Study
The research involved 426 children from an e-waste recycling region in China. Scientists analyzed urine samples to measure 18 metal(loid)s and 15 VOC metabolites, along with over 180 metabolic markers using advanced techniques. Children’s blood pressure was measured following standard pediatric guidelines. Statistical models and machine learning analysis showed that exposure to certain metal(loid)s — including cobalt, gallium, and tin — and VOCs was strongly associated with elevated blood pressure.
The Hidden Role of the Gut
One of the study’s most striking findings was the link between pollution and the gut’s metabolic activity.
Changes in metabolites such as l-glutamine and N-phenylacetyl-l-glutamine (PAGln) suggest that gut bacteria may play a role in how the body responds to toxic exposure. Pollutants may disrupt gut microbiota, triggering oxidative stress and hormonal imbalances, which over time could raise blood pressure.
Future Implications
This research sheds light on an emerging public health threat. As global e-waste continues to rise, millions of children in low-income regions may face similar risks.
Experts stress the need for safer recycling practices, strict pollution controls, and regular health monitoring for children in affected areas.
The study also opens new doors for early detection and prevention, using metabolomic profiling to identify at-risk children before hypertension becomes irreversible.
TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Telemedicine Society of India
What is New?
The past few weeks have been remarkable for the digital health community, with clear momentum around collaboration, education, and responsible innovation.
First, a reminder – we are now less than 60 days away from TELEMEDICON2025, to be held at the Indian Institute of Science, Bangalore. If you haven’t registered, visit telemedicon.in and secure your place at this landmark event.
The TSI-AADH Joint Webinar highlighted the power of cross-border collaboration, blending Armenia’s and India’s experiences to advance telehealth solutions with global relevance. Closer home, the Telangana Chapter’s workshop brought together students, clinicians, startups, and policymakers, with vibrant poster presentations and innovation showcases reflecting how the next generation is ready to shape the future of telemedicine and AI in healthcare.
On the global stage, the Digital Health Summit 2025 in Mumbai set a new benchmark with the launch of the AI Pyramid Framework and the Hippocratic Oath for the Digital Age – reminders that ethics, trust, and equity must remain central as healthcare embraces digital transformation.
This issue also explores scientific frontiers – from AI-powered meal planning to smart hydrogels for wound care – showing how innovation is steadily moving from research into real-world practice.
What is new today is not just the pace of change, but the shared responsibility to ensure it remains patient-centric, inclusive, and ethical.
Thank You Dr. Sunil Shroff Chief Editor President-Elect, TSI
TSI–AADH Joint Webinar on Telehealth & Digital Health
Prof. (Dr) Umashankar S. Managing Director Med.Bot | Honorary Secretary, Telemedicine Society of India
The Telemedicine Society of India (TSI), in collaboration with the Armenian Association of Digital Health (AADH), organized a joint webinar on 12th September 2025 to strengthen international cooperation in digital health.
The program featured eminent speakers from India and Armenia, who shared insights on telehealth innovations, rural outreach models, remote ICU experiences, and digital health education.
Session Highlights:
The session commenced with a warm welcome by Dr. Umashankar S, Honorary Secretary of TSI, setting the tone for an engaging and collaborative program.
The President of TSI Dr. Prem Nair, highlighted the importance of digital health in India’s healthcare transformation and emphasized the society’s commitment to building global collaborations.
Dr. Ganapathy, a pioneer in telemedicine, presented India’s telehealth landscape, tracing its evolution, achievements, and the role it continues to play in expanding healthcare access.
Dr. Chaltikyan introduced the Master of Digital Health Alliance program, emphasizing the role of structured education in building the next generation of digital health leaders.
Dr. Murthy Ramila provided an overview of the collaboration between TSI and AADH, underscoring the potential for cross-learning and co-developing solutions for global health challenges.
Mr. Sawarkar presented the Neurosynaptic experiment, demonstrating how innovative solutions can extend telehealth to remote populations at scale.
Dr. Rawal spoke about the Remote ICU model, sharing real-world examples of how tele-ICU solutions are saving lives by extending specialist care to distant hospitals.
Dr. Ohannessian shared Armenia’s digital health landscape and opportunities
Dr. Sunil Shroff, explored collaborative opportunities between the two associations.
The event concluded with a vote of thanks by Dr. Krishna Kumar, reaffirming the commitment of TSI and AADH to foster innovation, education, and sustainable global partnerships in digital health.
Transforming Healthcare: From Ancient Insights to AI Innovations 20th September 2025 | ESIC Medical College, Hyderabad
Dr Akhila Kosuru Secretary TSI Telangana CEO & Co-founder – Augsidius Health
The Telemedicine Society of India – Telangana Chapter conducted a half-day workshop on “Transforming Healthcare: From Ancient Insights to AI Innovations” in collaboration with ESIC Medical College as the venue partner on 20th September 2025.
The event was proudly sponsored by KIMS Sunshine, Maheswara Medical College, Rijuven, Augsidius Health Technologies, Diginerve, and Pleapoint Consulting, with Hybiz TV as the media partner providing live coverage streamed on YouTube.
Participation & Engagement The workshop witnessed an overwhelming response with 390 registrations from a diverse audience, including medical students, biomedical engineers, practicing doctors, healthtech startups, NGOs, and faculty and administrators from medical institutes.
Adding further vibrancy, six healthcare startups and companies exhibited their innovations, gaining significant visibility, business leads, and stakeholder interest.
Institutional partners including KIMS-Sunshine, Rijuven, Diginerve, Medmokk, Maheswara Medical College, ESIC Medical College, Pleapoint Consulting, Augsidius Health Technologies, and Paras Medical Book Publishers extended their grand support with strong brand presence throughout the event.
Poster Presentation Competition A highlight of the day was a poster presentation competition on “Utilisation of Digital Health in Modern Medicine”, which saw enthusiastic participation with 15 posters showcased. The top three presenters were recognized and awarded for their innovative contributions by the jury consisting of Professor Dr Dinaker – General Medicine, Professor Dr Nagaraju – Maheswara Medical College, Dr Srinivas – Consultant Orthopedics and Dr Shivani Kailashchand Jain – Telemedicine Physician and EC Member of TSI Telangana.
The program commenced with a warm welcome by Professor Dr. Rajiv – Professor of Medicine, ESIC Medical College, setting a collegial tone for the day.
This was followed by a video message from Shri Ramachandra Vishnubhatta, President of TSI Telangana, who joined virtually from the USA. In his message, he expressed his delight in seeing the chapter host such an important program and conveyed his wholehearted support for its initiatives.
Dr. B.V. Krishna Rao, Senior Director of Maheswara Medical College and Vice President of TSI Telangana, then introduced the vision of the society and the state chapter for the current term. He highlighted the benefits of membership, while emphasizing that this workshop was the first in a planned knowledge series under the chapter’s grand vision. He also extended a special invitation to students to establish student chapters, assuring them that the society would support their efforts in gaining knowledge and exposure beyond conventional boundaries.
The Chief Guest, Dr. Radhika, Medical Superintendent of ESIC, shared her practical experiences with Tele-Ophthalmology, drawing attention to both its promise and its challenges. She highlighted how the success of telemedicine often depends on operational factors at the tele-centers, such as the functionality and ease of use of the software, and equally on the patient side, where issues like internet connectivity and access to technology can significantly impact the quality of care. She further emphasized the importance of doctors in India focusing on curating India-specific healthcare datasets to train AI models that are more relevant and effective in the local context. Her reflections not only brought real-world nuances into the conversation but also provided an inspiring direction for the scientific sessions that followed, urging participants to think about solutions rooted in ground realities.
Scientific Sessions The program featured insightful talks by seven eminent speakers, covering diverse perspectives:
Prof. Dr. Sadhna Sharma – Delivered a comprehensive overview of Telemedicine, tracing its growth, challenges, and potential to bridge healthcare access gaps. Her session covered the fundamentals of Telehealth and Telemedicine, ranging from online consultations to remote patient monitoring. What stood out was her ability to translate complex concepts into relatable insights, particularly around the practical implementation of telemedicine, setting the right expectations for patients, and structuring an effective tele- consultation. The session reflected her dual strength as both a seasoned telehealth physician and an experienced teacher, evident in the clarity and depth with which she engaged the audience.
Dr. Akhila Kosuru – Presented on “Demystifying AI in Healthcare”, offering a grounded perspective on how AI can serve as an augmenting intelligence to ease clinician workload and enhance decision-making. She highlighted the fundamentals of decision-support systems, the importance of a critical understanding of open-source LLMs – including their strengths and limitations and the pivotal role of doctors as early adopters, validators, and co-creators of AI rather than passive end-users. Drawing from her own journey in health-tech innovation, she shared how her team is designing solutions like AstraAI – an AI agent and thinking companion for doctors and medical students. Her talk left the audience with a promising outlook on how clinician-driven AI can reshape medical practice.
Ms. Ifrazunnisa Khan – Delivered an insightful session on India’s New Data Protection Law, outlining its far-reaching implications for healthcare data security and compliance. She contextualized the discussion within the evolving landscape of telemedicine and artificial intelligence, which naturally prompted numerous audience queries on patient privacy, secure digital practices, and legal responsibilities. As an advocate, she addressed these concerns with remarkable clarity and patience, explaining the rights, regulatory frameworks, and practical steps needed to navigate this space responsibly. Her session not only demystified the legal nuances but also reassured participants on how to align innovation with compliance.
Dr. Rahul Lakshminarayanan – Spoke on the relevance of AI in vascular imaging and intervention, highlighting its potential to enhance diagnosis and treatment precision. He noted that surgical fields remain relatively uncharted territory for AI, where adoption is still at an early stage. Drawing on global practices, he shared practical use cases that represent low-hanging opportunities for innovation in vascular care. His talk emphasized the enormous potential outcomes AI could unlock in this domain and the growing interest it is generating. By the end, his presentation served as a call to innovators to explore the fusion of AI with vascular surgery, opening avenues for impactful advancements.
Dr. Snigdha Mokkapati – Spoke on the impact of oral health on general health, emphasizing that the mouth often serves as a window to systemic health, with strong associations to conditions such as cardiovascular disease and diabetes. She highlighted how oral health remains a relatively neglected area in preventive care and shared her vision of integrating oral health screening into general health screening programs. Introducing her innovation, the D-Oral device, she explained how it is being deployed in population screening to not only increase visibility of oral health issues but also provide better interpretation and early detection prospects. Her session underscored the importance of elevating oral health within the broader public health agenda.
Dr. Hima Bindu – Joined as a guest speaker, bringing her perspective as a clinician and entrepreneur. She is the Founder of Angel Eyes, an AI-driven platform that connects people with the right doctors, and Co-Founder & COO of Salubrity, an award-winning health-tech startup. In her talk, she introduced these innovations, speaking about how AI can be applied to areas such as nutrition, hair health, and digital care. Her session not only highlighted the recognition her ventures have received at forums like the Global AI Summit 2024 and T-Hub Hackathon but also inspired the audience to view the role of doctors as entrepreneurs and innovators in shaping the future of healthcare.
Program grandly ended with vote of thanks delivered by Mr Uma Mahesh Katta.
Organizing Committee The successful execution of the workshop was made possible by the dedicated efforts of the Organising Committee: – Mr. Uma Mahesh Katta – Vice President – Rijuven, Treasurer TSI Telangana – Mr. Errabelli Ram Mohan – Program Coordinator – Ms. Shivani Jain – Program Coordinator, EC Member Telemedicine Society of India – Telangana Chapter – Dr. Srinivas – Associate Professor, Maheswara Medical College – Professor Dr. Rajiv – Professor of Medicine, ESIC Medical College (Chair, Organising Committee) Special thanks were also extended to the volunteers and ESIC team for their tireless support.
Acknowledgement The Telemedicine Society of India – Telangana Chapter extends its heartfelt gratitude to the sponsors, speakers, institutional partners, participants, and volunteers for their invaluable contributions.
Their collective support and active involvement ensured the workshop’s success and reinforced the vision of advancing healthcare through technology, innovation, and collaboration.
The program concluded on a high note, leaving participants with renewed inspiration and a positive outlook on the transformative impact of digital innovations in medicine. The students, in particular, expressed great excitement about their participation, reflecting the enthusiasm of the next generation to engage in healthcare innovation and digital transformation.
How AI Is Revolutionizing Healthy Meal Planning
Dr. Trupti Shirole BAMS (Bachelor of Ayurvedic Medicine and Surgery) Content Writer, Medindia.net
Healthy eating often sounds simple- but in real life, busy schedules, family commitments, and countless food choices make it hard to stick to a balanced diet. Now, artificial intelligence (AI) is stepping in as a smart kitchen companion, promising to make healthy meal planning easier and more personalized than ever.
Why Diet Matters and Why Healthy Habits Are Hard to Keep Global rates of lifestyle-related diseases like stroke, heart attack, obesity, and type 2 diabetes are rising. Doctors agree that active living and a nutritious diet matter, but it’s tough to break old habits, avoid junk food, and cook nutritious meals every day. The challenge is not just knowing what’s healthy- it’s staying on track in the face of temptation and life’s demands.
AI Dishes Out Personalized Meal Plans Rooted in the Mediterranean Diet The latest research published in Frontiers in Nutrition introduces an AI-based nutritional recommendation system (AINR) that creates weekly meal plans using Mediterranean cuisine.
This approach combines taste, nutrition, and even cultural preferences for a menu plan that’s designed just for you.
The Mediterranean diet is renowned for its health benefits- balanced meals include vegetables, fruits, whole grains, olive oil, fish, dairy, and nuts, with limited red meat and sweets. Long-term studies link this dietary pattern to lower rates of heart disease and longer, healthier lives.
How Do AI-Based Meal Planners Work? Traditional meal planning systems used mathematical or filtering algorithms to mix and match foods, but they often fell short in real-world meal prep. They couldn’t adapt to allergies, dietary restrictions, or user preferences well, and tended to repeat meals or ignore cultural differences.
AI-based systems like the new AINR overcome these hurdles by using:
Knowledge-based optimization: Rules set by nutrition experts, verified for balance and accuracy.
Machine learning: AI learns from users’ habits, expressed tastes, and lifestyle context to offer meal plans people will actually follow.
A user’s dietary profile- including allergies (like milk, nuts, or eggs), cultural needs (halal options), and even seasonal ingredients—feeds into the AI system along with their calorie and nutrition needs. From this information, the AI crafts a weekly menu rooted in Spanish or Turkish Mediterranean dishes.
Step-by-Step: What Does the AI Meal Planner Do? To generate a weekly meal plan, the AINR goes through four main steps:
Filters meals by season and local cuisine, keeping them fresh and relevant.
Excludes anything that would conflict with your allergies or preferences.
Scores and assembles daily menus based on energy and macronutrient (protein, fat, carbs) targets.
Assembles the week’s plan, aiming for diversity (not repeating meals more than three times per week, only three servings of fish weekly, etc).
While auto-generated plans are not yet dietitian-validated, human nutrition experts oversee results to keep things safe and effective.
Benefits and Limitations of AI for Suggesting Diet Plans The AINR system showed impressive accuracy for most groups. It filtered out foods based on allergies and cultural needs with 100% success, and most calorie and nutrition targets were met. Spanish users and Turkish women saw nearly perfect results.
Some gaps remain. The database lacked enough dairy-free or nut-free options for Spanish users with allergies, preventing viable weekly plans. Turkish male users had less accurate plans, likely due to database limitations. For the AI system to truly help everyone, researchers plan to expand the menu database and test these suggestions with real families.
More Diverse, Healthy Eating with AI Researchers say AI-based systems “hold promise in facilitating more balanced dietary habits,” but improvements are needed, especially for people with food allergies. The next phase will involve real-world testing through intervention programs, with hopes to extend AI planning for entire families.
AI: Healthy Assistant But Not a Substitute for Human Expertise AI can take the hassle out of planning and shopping, but human nutritionists are still essential for customizing plans and guiding those with complex health needs. With more data and smarter software, personalized healthy eating could become easier, tastier, and more achievable for everybody.
The Role of AI-Powered Conductive Hydrogels in Wound Care
Chronic wounds—including diabetic foot ulcers, pressure sores, and joint-related injuries—remain a major strain on healthcare systems worldwide.
In response, a group of Chinese researchers has unveiled a breakthrough solution: advanced conductive hydrogel dressings enhanced with artificial intelligence, designed to enable smart wound monitoring and accelerate the healing process.
A New Era of Personalized Wound Care This comprehensive review, led by researchers from China Medical University and Northeastern University, outlines how these smart dressings combine real-time physiological signal detection with artificial intelligence, offering a new paradigm in personalized wound care.
Real-Time Monitoring: Conductive hydrogels can track key wound parameters such as temperature, pH, glucose levels, pressure, and even pain signals—providing continuous, non-invasive insights into wound status.
AI-Driven Analysis: Machine learning algorithms (e.g., CNN, KNN, ANN) process sensor data to predict healing stages, detect infections early, and guide treatment decisions with high accuracy (up to 96%).
Multifunctional Integration: These dressings not only monitor but also actively promote healing through electroactivity, antibacterial properties, and drug release capabilities.
Key Features: Material Innovation: The review discusses various conductive materials (e.g., CNTs, graphene, MXenes, conductive polymers) and their roles in enhancing biocompatibility, sensitivity, and stability.
Smart Signal Output: Different sensing mechanisms—such as colorimetry, resistance variation, and infrared imaging—enable multimodal monitoring tailored to wound types.
Clinical Applications: The paper highlights applications in pressure ulcers, diabetic foot ulcers, and joint wounds, emphasizing the potential for home care, remote monitoring, and early intervention.
Addressing Challenges in Smart Dressings for Clinical Use Despite promising advances, issues such as material degradation, signal stability, and AI model generalizability remain. Future efforts will focus on multidimensional signal fusion, algorithm optimization, and clinical translation to bring these intelligent dressings into mainstream healthcare.
This work paves the way for next-generation wound care, where smart materials meet smart algorithms—offering hope for millions suffering from chronic wounds.
Stay tuned for more innovations at the intersection of biomaterials, AI, and personalized medicine!
Global Digital Health Summit 2025 sets new direction for ethical and scalable transformation in healthcare
Press Release
Summit unveils AI Pyramid Framework, introduces Hippocratic Oath for the Digital Age, and builds consensus on workforce readiness, patient-centred care, and global health equity.
Mumbai, September 23, 2025 — The Global Digital Health Summit 2025 concluded in Mumbai with frameworks that will reshape clinical practice and healthcare delivery worldwide. More than 2,000 leaders from 30 countries — including clinicians, policymakers, researchers, and patient advocates — participated in three days of intensive discussions that progressed from vision to implementation to scale.
The Summit’s centrepiece was the AI Pyramid Framework, the world’s first structured model for embedding AI responsibly across healthcare systems. Dr. Rajendra Pratap Gupta, Chairman of GDHS, said, “This is healthcare’s defining moment. Artificial intelligence is not just a tool, it is a structural shift in how we design, deliver and experience care. Wherever there has been technology, it has created new opportunities, new jobs and new industries, and healthcare will be no exception. The AI Pyramid Framework is meant to guide this transformation in a responsible and structured way, ensuring that professionals are not just users of AI but creators and shapers of it.”
A defining milestone was the unveiling of the Hippocratic Oath for the Digital Age, a new pledge that redefines medical ethics for an era of technology-enabled care.
The Summit emphasized patient-centred transformation, including chronic disease management and digital therapeutics. Dr. Joseph Kvedar, Co-Chair of GDHS and Professor at Harvard Medical School, said, “We are moving from episodic to continuous care, thanks to innovations like remote patient monitoring and measurable health technologies. This is one of the most profound shifts in modern medicine.”
Equity and access remained central themes. Shri Bharat Lal, Secretary General of the National Human Rights Commission, stated, “The right to life, the right to health, the right to health care, and the right to access affordable services are all fundamental human entitlements.”
From the institutional side, Dr. Sunil Kumar Barnwal, IAS, CEO of the National Health Authority (NHA), said, “Enhancing healthcare access and quality through digitalization significantly improves the availability and accessibility of healthcare services to citizens.”
The Summit also focused on workforce readiness, offering CME and CNE credits alongside AI certification workshops, and reaffirmed the importance of the One Health approach and cybersecurity. It closed with the Global Digital Health Special and Innovation Awards, celebrating contributions already reshaping patient care.
By integrating frameworks for ethics, clinical integration, and patient-centred equity, GDHS 2025 established a new global benchmark for healthcare transformation.
About the Global Digital Health Summit The Global Digital Health Summit, Expo & Innovation Awards (GDHS) is a leading international platform for advancing digital health. It convenes healthcare leaders across policy, clinical practice, and technology to develop frameworks for ethical, secure, and scalable integration of innovation into patient care.
TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Telemedicine Society of India
What is New?
The August 2025 issue of the newsletter covers a variety of interesting articles.. Dr.Ganapathy brings forward an interesting perspective. He has observed that many papers struggle due to outdated data, narrow scope, or methodological weaknesses. One recent example was a survey on doctors’ awareness of telemedicine conducted in 2021 but submitted for publication in 2026. With such a gap, the findings risk losing relevance, particularly as telemedicine has advanced rapidly post-COVID. Another case was a 15-year literature review on artificial intelligence in pediatric dermatology, which relied only on PubMed and Google Scholar, ignored non-English publications, and missed recently published studies. These cases illustrate the importance of timeliness, comprehensiveness, and methodological rigor for authors hoping to publish credible research.
The 4th Seminar on Telemedicine and Healthcare Research, was held on 9th August 2025 at KCG College of Technology in Chennai and organized by the TSI Tamil Nadu Chapter. The event featured sessions on IoT-enabled chronic disease monitoring, the emerging “Internet of Medical Thinking,” and the application of artificial intelligence in ophthalmology. A lively panel debated the central question: Can Telemedicine Truly Revolutionize Healthcare Delivery? with enthusiastic participation from students underscoring growing interest in digital health.
In the North-East, the TSI Chapter in collaboration with AIIMS Guwahati organized its Mid-Term Conference and National Workshop on TMPG and Business Models for Sustenance on 29–30 July 2025. The program included sessions on telemedicine in CBRN events, patient safety, legal frameworks, and live demonstrations of teleconsultations from remote Assam. These sessions helped medical and nursing students appreciate the practical application of TMPG.
Meanwhile, Medicon 2025, hosted by the TSI Himachal Chapter in Mohali on 23–24 August, brought together over 300 delegates under the theme “The Future of Healthcare.” The meeting highlighted artificial intelligence in clinical practice, tele-ICUs, oncology, and ethics, and introduced the “Torchbearer of Digital Health” Award to honor innovators.
An innovation worth noting is a newly developed wearable lithium sensor that enables sweat-based, real-time monitoring for bipolar patients. Needle-free, smartphone-connected, and potentially AI-integrated, it marks a step forward in making mental health care more patient-centered and preventive.
Together, these developments reaffirm that telemedicine in India continues to evolve rapidly, combining research, education, innovation, and policy to bring technology closer to patient care.
Thank You Dr. Sunil Shroff Chief Editor President-Elect, TSI
Submitting a paper? – Illustrations from a Reviewer
Dr. K. Ganapathy Distinguished Professor The Tamilnadu Dr MGR Medical University | Emeritus Professor National Academy of Medical Sciences | Formerly Distinguished Visiting Professor IIT Kanpur | Past President, Telemedicine Society of India / Neurological Society of India | Formerly WHO Digital Health Expert | Formerly Founder Director Apollo Telemedicine Networking Foundation (2000-2024)
The author during the last several years has been regularly reviewing 50+ articles a year for 50+ international journals in the broad area of Digital Health. The information given below is to give an idea of the type of articles submitted worldwide and why many of them are asked to resubmit. Hopefully potential authors will find this information useful
1. Togolese doctors’ awareness, perceptions and practices of telemedicine
Reviewer’s comments
It is universally acknowledged that worldwide there has been a phenomenal growth and development of telemedicine post Covid. It is therefore difficult to accept the relevance of a very small study carried out in Jan- March 2021 which will be published 5 years later
From a purely scientific viewpoint the study has several major limitations which preclude extrapolating the observations made to the country as a whole a) the study is a biased sample as it is confined only to doctors who had given their informed consent to participate in the study . The authors themselves state “ —small number, reflects the low level of interest among doctors in participating in the surveys”
5 of the references cited are 2009 and 2012 and are only of historical importance
It is very unlikely that the views and perceptions of the sample studied in 2021 will be relevant in 2026 ( if article is published )
The authors only mention Europe and USA ignoring India and China the most populated countries of the world
It is stated that “ —the English language version is appended to the manuscript as a supplementary file”. It is assumed that the actual survey was done in the local language. If so details are required of how independent translation and retranslation into English was done.
While age, gender, experience etc of the sample studied are given, this has no relevance unless the reader has similar details of those not in the sample. In other words we need factual data to be sure that the sample truly represents the population of doctors in the country.
It is suggested that the study be repeated now and the information obtained in 2021 be used to show the transformation in perceptions in the last 5 years
2. Perspectives and Challenges of Telemedicine And Artificial Intelligence in Pediatric Dermatology
Reviewer’s comments
Period of study is 15 years. This raises a serious concern as quality of photography/ image transmission/ knowledge/communication technology/ skills of remote consultation etc etc in the last 3-5 years cannot be compared with that in use in the preceding 10 years
The search has been confined to Pubmed and Google Scholar databases.
It is quite possible that some published articles in this specific area could have been overlooked since Cochrane Library, eMBase, Scopus, Web of Science, Sciernxce Direct, UptoDate and others have not been covered
The authors conducted a literature review including only articles published in the last 15 years. 331 studies were identified, of which only 73 were included.. There is no original work as such by the authors. The paper is only a cumulative extrapolation of individual interpretations of observations made by multiple authors over a 15 year period.
The Materials and Methods section needs considerable changes
Obviously there are major limitations in even attempting to summarise this data. It is expected that there is a major discussion on “ limitations” pointing out that literature published in non English languages have been totally ignored. It is well known that China, Japan and Korea are major contributors in this area and most of the articles published from these countries are not in English
Even if this is not a formal meta analysis a 15 year review of articles presupposes that formal standard guidelines are followed eg PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) is an evidence-based minimum set of items aimed at helping scientific authors to report a wide array of systematic reviews and meta-analyses, primarily used to assess the benefits and harms of a health care intervention.
Specific details are expected of why majority of articles obtained were rejected, An algorithm flow chart is a standard accompaniment of any review of papers
It is imperative that all MeSH words be used as search terms. Use of the Boolean AND alone is insufficient.
References include a paper published in 1992 ( ref no 19 ) – 32 years ago whereas study has been reported as 15 years up to Jan 2024
Relevant papers published in Jan 2024 have not been quoted – a few examples are given below
The authors are advised to do a more detailed search taking into account the observations mentioned above.
They could consider analysing the papers reviewed in blocks of 5 years to make the interpretation more meaningful.
Report of 4th Seminar Series on Telemedicine and Healthcare Research
Mr. D. Satheesh Kumar, M.Sc (IT), MBA, DECE. Honorary Secretary – TSI, Tamilnadu Chapter
Venue: F14 Seminar Hall, KCG College of Technology, Chennai Date: 09.08.2025
The Department of Electronics and Communication Engineering, in association with the Telemedicine Society of India – Tamil Nadu Chapter and MedIndia, Chennai, organized the 4th Seminar Series on Telemedicine & Healthcare Research on 9th August 2025 at F14 Seminar Hall. The event aimed to bring together industry leaders, medical professionals, researchers, and students to explore the future of healthcare delivery through telemedicine and emerging health technologies. The seminar’s central theme was the thought-provoking question: “Can Telemedicine Truly Revolutionize Healthcare Delivery?”
The program commenced at 9:30 am with a Prayer Song, followed by the Lighting of Kuthuvilaku by dignitaries.
The seminar commenced with a warm welcome address delivered by Dr. Kavitha Balamurugan, Head of the Department of Electronics and Communication Engineering, who set a professional and engaging framework for the day’s proceedings.
Dr. Muthukannan, Principal of KCG College of Technology, delivered the Principal’s Address, emphasizing the importance of interdisciplinary collaboration in advancing healthcare innovations. This was followed by the Presidential Address from Dr. Ikramulla G.H, President – TSI (Tamil Nadu Chapter), who spoke on the transformative potential of telemedicine in bridging healthcare access gaps.
The technical sessions commenced with Dr. Haleema Yezdani, General Physician and Diabetologist from Bangalore, who delivered a talk on “Role of Remote Monitoring in the Management of Chronic Diseases in the Digital Health Era.” Her presentation focused on IoTbased monitoring, preventive healthcare, and real-time patient data management.
Mr. Binu Janardhan, Joint Director at C-DAC, Thiruvananthapuram, Kerala, presented a session on “An Overview of the Internet of Medical Thinking,” introducing futuristic healthcare communication frameworks and interoperability solutions.
Mr. Rajarajan S, Group Chief Operating Officer of ASRAM Hospitals, Andhra Pradesh, shared insights in his talk “Healthcare, Wellness & What’s Next: Real Hackathon on Code to the Cure,” outlining strategies to integrate medical innovation with entrepreneurial solutions.
Dr. Sheila John spoke on “The Role of Artificial Intelligence in Diabetic Retinopathy and Agerelated Macular Degeneration,” highlighting AI’s role in early detection and prevention of vision loss. Special addresses were delivered by Dr. Senthil T, Director & CEO of Welfare Health Systems, on policy frameworks and best practices in telehealth adoption, and Mr. D. Satheesh Kumar, Technical Head – Telemedicine, SRMC, who discussed implementation challenges and solutions in scaling telemedicine systems. A panel discussion on “Can Telemedicine Truly Revolutionize Healthcare Delivery?” moderated by Kaviya K featured panelists Mr. Napolean C, Dr. T. Senthil, Mr. D. Satheesh Kumar, and final-year ECE students Mr. Mohamed Shuhail G and Mr. Mudhassir Habeeb.
The discussion covered technology integration, policy requirements, implementation hurdles, and the future of telemedicine in India, culminating in an engaging audience Q&A session. The event concluded with a Vote of Thanks delivered by Dr. B. Thyla, Assistant Professor (Senior Grade), Department of ECE, who expressed heartfelt appreciation to the speakers, organizers, and participants. The seminar successfully achieved its objective of bridging academia, healthcare, and industry perspectives, motivating students and professionals to contribute to the evolving field of telemedicine and healthcare research. Key takeaways included the potential of telemedicine to enhance healthcare accessibility in rural and underserved areas, the pivotal role of AI, IoT, and secure data platforms in the next phase of telehealth, and the importance of policy formulation, trust-building, and affordability for large-scale adoption. Participants from various engineering colleges within and outside Chennai, including institutions from Salem, Dindigul, Nagapattinam, and Bangalore, joined the seminar through online mode and benefited from the insightful discussions.
TSI Mid-term Conference and National Workshop on TMPG and Business Model for Sustenance at AIIMS Guwahati
Dr. Murthy Remilla Vice-President, Telemedicine Society of India
Dr. Murthy Remilla, Vice-President TSI & Mr.S.N.Farid, Organising Secretary, Mid Term Conference-2025
The TSI NE Chapter organised TSI Mid-term Conference and National Workshop on TMPG and Business Model for Sustenance at Guwahati During 29-30, 2025.
As part of this and continuing the model of Conference at your doorstep to attract more number of students, a Workshop on Telemedicine was organised at NEPNI Group of Nursing Institution in Alikash, Guwahati, Assam on 29th July’25. Dr. Murthy Remilla, Vice-President, TSI delivered a lecture on the Evolution and growth of TM in India and also gave the introduction to TM practice guidelines. He also answered the students’ queries on the applicability and need of TMPG for nursing students and paramedics etc. It was well received as medical and nursing students from the institution showed immense eagerness towards the concept of Telemedicine. We had a good long session with the faculty & students. Dr. Murthy also gave a live demonstration of TM software. Organising Secretary Mr. S.N.Farid also gave a live demo of actual tele-consultation from a very remote area from one of the Telemedicine Centres at Dibrugarh, Assam to demonstrate what actual Telemedicine in practice is. Dr.Murthy invited the students to take-up internships in the area of TM with the help of TSI and also invited them to Telemedicon-2025 due to be held at Bangalore.
That afternoon, another session was held with the Medical & IT students of Royal Global University, Lokhra, Guwahati, Assam where students were briefed about the use of Telemedicine in various sectors of our country. It was a stupendous session, where the students were inquisitive & put practical questions to our TSI dignitaries. The session where the medical students put forward their queries to our speakers regarding all sorts of application of Telemedicine in daily life was interactive. Here also, both Dr. Murthy & Mr. Farid gave a live demo & presentation of actual Teleconsultations from remote areas & its benefits.
National Workshop on TMPG and Business Model for Sustenance was held on Day 2 July 30, 2025 with participation of Students & Faculty from AIIMS. The forenoon has a variety of topics like, Telemedicine Demonstration – By Telemedicine Society of India Team led by Dr. Murthy Remilla followed by Tele-talk by the Chief Patron of the event Prof. Ashok Puranik, Executive Director, AIIMS, Guwahati who highlighted the importance of the advanced technologies and their use and application by the medical fraternity and welcomed affordable and portable Telemedicine/Digital Health services for the interiors and inaccessible areas of N.E.
Presentations on Role of Telemedicine in CBRN events by Dr. Suvan Kanti Chowdhury, Quality of Care and Patient Safety in Telemedicine by Dr. Biraj Ch Paul and a talk on Telemedicine services at AIIMS, Guwahati attracted the delegates with multiple aspects of TM.
As part of the National Workshop, the afternoon session had 3 talks – Introduction to Telemedicine-Evolution and Growth, and Technologies for Telemedicine by Dr. Murthy Remilla followed by an interactive talk on Telemedicine Practice Guidelines issued by MoH&FW by Dr. Surya Bali of AIIMS, Bhopal. Both the speakers also discussed the Ethical and Legal Aspect of Telemedicine and answered the queries from the delegates. This was followed by a talk on Business and Revenue Model in Telemedicine by Mr. S N Farid, TSI, Guwahati. About 77 delegates including Prof. Roonmoni Deka, Dean Research; Prof. S P Sinhasan, Dean Examination, Prof. N Brian Shunyu, Medical Superintendent, AIIMS, Guwahati participated in this event.
The Mid Term Conference-2025 of TSI conducted by North East India Chapter of TSI and AIIMS Guwahati came to close with thanks giving by TSI to AIIMS team led by Organising Chairman Dr. Md Jamil, Department of General Medicine and Organising Secretary Dr. Nilanjana Ghosh, Dept. of Community & Family Medicine followed by a group photo.
Medicon 2025: Charting the Future of Healthcare through Digital Innovation
Dr. Sachin Verma President, TSI Himachal Pradesh Chapter | Founder and Director, Holy Basil Hospital
Telemedicine Society of India – Himachal Chapter in collaboration with Mohali Association of Physicians and Surgeons (MAPS) and Budget ICU, successfully organized Medicon 2025 on 23rd and 24th August 2025 at Mohali. The conference brought together over 300 delegates, including practicing physicians, administrators, digital health innovators, and AI specialists from across the region, making it one of the most impactful scientific meetings of the year.
A Convergence of Medicine and Technology
With the central theme “The Future of Healthcare”, Medicon 2025 focused on the evolving role of digital health, telemedicine, and artificial intelligence in shaping clinical practice. The scientific program was meticulously designed to combine clinically relevant topics with cutting-edge technology, ensuring that participants derived maximum practical value.
Over the two days, the conference hosted a series of plenary lectures, debates, and panel discussions. Topics ranged from AI in clinical practice, tele-ICUs, remote patient monitoring, ethical challenges in digital health, to e Oncology and new guidelines in internal medicine. Each session stimulated lively discussions and offered actionable insights for clinicians working both in urban centers and peripheral settings.
Recognizing Pioneers in Digital Health
A key highlight of the conference was the institution of the “Torchbearer of Digital Health” Award, designed to recognize individuals who have made exceptional contributions in taking digital health to the masses. This award not only celebrated innovation but also underscored the commitment of Medicon and TSI to encourage physicians and institutions that bridge technology with patient care.
Faculty and Delegates: A Unique Blend
The conference brought together top physicians, digital health entrepreneurs, and technology administrators under one roof. Eminent faculty included experts from internal medicine, critical care, endocrinology, and cardiology alongside digital health pioneers , from institutions like ISRO, IIT, AIIMS, PGIMER, CDAC , HCL and all Medical Colleges of Himachal Pradesh , creating a rare platform where traditional clinical wisdom interacted with futuristic technology. Telemedicine Nodal In-charges of leading government medical colleges—including PGIMER Chandigarh, IGMC Shimla, RPGMC Tanda, , RPGMC Hamirpur and SLBS GMC Mandi—participated actively and pledged their institutional support towards scaling and implementing digital health initiatives across the region. This unique blend enabled participants to not only learn about advances in their specialties but also understand how technology can be seamlessly integrated into daily practice.
A Step Towards Mainstreaming Digital Health
By the close of Medicon 2025, the resounding message was clear: the future of healthcare lies in collaboration between doctors and digital tools. The conference highlighted both the promise of AI and telemedicine in improving access, efficiency, and patient safety, as well as the challenges around bias, black-box algorithms, and medico-legal implications.
For the Telemedicine Society of India, Medicon 2025 reaffirmed its role as a key driver in mainstreaming digital health across India. The overwhelming response from participants is a testament to the growing curiosity, readiness, and commitment among physicians to embrace this transformation.
Telemedicine Society of India (TSI) – New Executive Committee Details of various chapters
Prof. (Dr) Umashankar S. Managing Director Med.Bot | Honorary Secretary, Telemedicine Society of India
Telemedicine Society of India (TSI) – New Executive Committee of Tamil Nadu Chapter
Effective from August 2025
Note: The Executive Committee was elected during TSI Tamil Nadu Chapter – Meeting, and will serve for the term 2025–2027.
***************************************
Telemedicine Society of India (TSI) – New Executive Committee of Himachal Pradesh Chapter
Effective from 21st June 2025 Note: The Executive Committee was elected during TSI Himachal Pradesh Chapter – Meeting, and will serve for the term 2025–2027.
For decades, patients with bipolar disorder have had to rely on frequent blood tests to ensure their lithium medication is working safely. Now, a groundbreaking study published in Device has unveiled a first-of-its-kind wearable device that can monitor lithium levels through sweat, eliminating the need for needles and clinic visits.
Organic Electrochemical Transistor Technology in Lithium Sensors
In early trials, this fully printed, organic electrochemical transistor (OECT)-based patch demonstrated the ability to detect lithium at concentrations as low as 0.1 millimoles, with high selectivity over similar ions. Data collected by the patch matched commercial sensor readings, showing promise for real-time, non-invasive lithium monitoring directly from the comfort of home.
Why Continuous Lithium Monitoring Matters for Mental Health
Lithium is considered a gold-standard treatment for bipolar disorder, which stabilizes mood and reduce episodes of depression and mania. However, it has a narrow therapeutic range. If levels are too low, the medication is ineffective; if too high, it can cause kidney damage, thyroid problems, or even life-threatening toxicity.
Real-Time Lithium Tracking Through Sweat Analysis
Current monitoring methods require blood draws, which can be uncomfortable and inconvenient, often leading to missed tests. This new wearable offers a way to track levels continuously, providing faster feedback to adjust doses before problems arise.
Fully Printed Lithium Sensor for Affordable Production
At the heart of the device is an organic electrochemical transistor, designed specifically to detect lithium ions. Unlike conventional sensors that require complex manufacturing, this one is entirely printed using inkjet and 3D printing techniques.
The sensor integrates three main features:
An ion-selective membrane for lithium detection
Iontophoretic sweat induction to stimulate sweat without physical activity
Microfluidic channels to guide sweat for real-time sensing
Smartphone-Connected Lithium Monitoring for Patient Convenience
Once placed on the skin, the patch gently induces sweat using a safe, low-level electrical current. Within minutes, it measures lithium levels and transmits the data wirelessly to a smartphone app. Patients and healthcare providers can then review results instantly, allowing for timely treatment adjustments.
Pilot Testing of Lithium Sensor with Bipolar Patients
The research team validated the device in both healthy volunteers and patients already receiving lithium therapy. Sweat lithium readings from the wearable closely matched those obtained from larger, commercial sensors, confirming its accuracy.
Patients who tested the device expressed relief at the prospect of monitoring their health without repeated hospital visits. The ability to avoid needles, combined with ease of use, was cited as a major benefit.
The implications go beyond comfort. Continuous monitoring means clinicians can respond faster to changes in lithium levels, preventing dangerous spikes or drops. Over time, this could help fine-tune doses for each individual, taking into account factors like weight, diet, and metabolism.
The Future of AI-Powered Lithium Dose Management
The team’s next goal is to integrate artificial intelligence into the system. Future versions may automatically recommend dosage changes, helping patients stay within the safe therapeutic window without frequent clinic visits. This approach could significantly improve treatment outcomes while reducing healthcare costs.
Why Sweat is the Game-Changer
Sweat is an underused diagnostic fluid, despite containing valuable information about the body’s chemistry. It offers a non-invasive, easily accessible alternative to blood and can reflect changes in real time. By harnessing sweat’s potential, this wearable technology opens doors to other applications, such as monitoring electrolytes, hydration, or even medication levels for other conditions.
This innovation marks a turning point in bipolar disorder care. By replacing needles with a comfortable patch and clinic visits with real-time smartphone updates, it addresses one of the biggest barriers to effective lithium therapy: consistent, accurate monitoring. It is a step toward making mental health care more patient-centered, personalized, and preventive.
For those living with bipolar disorder, the future may hold a world where managing your medication is as simple as checking your phone. Every drop of sweat could be a step toward peace of mind.
TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net