17th Annual International Conference (TELEMEDICON2021) of Telemedicine Society of India
The 17th Annual International Conference (TELEMEDCICON2021) of Telemedicine Society of India to be held on 12th-14th November, 2021. The theme of the conference is – ‘Tele-health Trends in the 21st Century.’ This issue of the newsletter carries the program for your perusal. Due to COVID the number of participants who would be physically attending are limited, however it is expected that like the last year there will be an overwhelming response. The sessions for free papers and posters are still open. Do make your submission to make the meeting a success.
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
This issue does not cover any activity and one reason is that next month we have our annual TELEMEDICON conference coming up at Lucknow in the Hybrid mode. The program is listed in this issue to highlight the conference.
We are carrying our usual monthly features – the medico-legal section, history of telemedicine in India and the popular news items.
We wish all our readers a very happy Diwali. Be safe and be healthy.
Thank You Dr. Sunil Shroff Chief Editor President – TN Chapter – TSI
Informed Consent for Telemedicine
Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist Law Firm Eshika Phadke Associate, Arogya Legal – Health Laws Specialist Law Firm
The developments in the field of information technology have resulted in geographic borders becoming increasingly redundant. Within the healthcare system, this has had a marked impact on the access that patients have to medical care since it is becoming increasingly common for doctors to consult a patient remotely. The Telemedicine Practice Guidelines have re-affirmed that inter-state teleconsultations within India are lawful and permitted…Readmore
History of Teleophthalmology at Sankara Nethralaya
Dr. Sheila John Head of Teleophthalmology and E-Learning Department, Sankara Nethralaya, Chennai.
Teleophthalmology holds great potential to improve the quality, access, and affordability in health care. For patients, it can reduce the need for travel and provide the access to a super-specialist. Ophthalmology lends itself easily to telemedicine as it is a largely image based diagnosis. The rapid progress achieved in the field of Telecommunications renders Teleophthalmology easily feasible…Readmore
17th Annual International Conference (TELEMEDICON2021) of Telemedicine Society of India
The 17th Annual International Conference (TELEMEDICON2021) of Telemedicine Society of India to be held on 12th-14th November, 2021. The theme of the conference is – ‘Tele-health Trends in the 21st Century.’ This issue of the newsletter carries the program for your perusal. Due to COVID the number of participants who would be physically attending are limited, however it is expected that like the last year there will be an overwhelming response. The sessions for free papers and posters are still open. Do make your submission to make the meeting a success…Readmore
FICCI Healthcare Excellence Award 2021 Bagged by Meenakshi Mission Hospital Madurai’s Meenakshi Mission Hospital & Research Center has secured the 13th edition of FICCI Healthcare Excellence Awards 2021 in the category of Digital Innovation in Healthcare. Introduction of Teladoc Health Robots by the hospital in June 2020 helped confer the award…ReadMore
Partnership aimed at leveraging AI for medical diagnostics: Nivruti Rai, Intel India Intel on Monday said that it has partnered with IIIT-Hyderabad, Public Health Foundation of India (PHFI) and Telangana government to set up a new ‘Applied Artificial Intelligence (AI) Research Centre’ for solving challenges in key sectors like healthcare and smart mobility… ReadMore
International
Duke Professor Wins $1 Million Artificial Intelligence Prize, A ‘New Nobel’ Cynthia Rudin becomes second recipient of AAAI Squirrel AI Award for pioneering socially responsible AI. She is being cited for “pioneering scientific work in the area of interpretable and transparent AI systems in real-world deployments… ReadMore
AI ALGORITHM ENHANCES ABILITY TO DIAGNOSE HEART FAILURE Among other things, analysis suggested that the algorithm may be effective at detecting heart weakness in all patients, regardless of race and gender… ReadMore
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- www.medindia.net
Telemedicine has recently emerged and gained popularity as a new hope to remove the bottlenecks in the healthcare seeking. While telehealth technology and its use are not new, widespread adoption among patients, especially in rural areas, beyond simple telephone correspondence has been relatively slow. Many professional medical societies endorse telehealth services and provide guidance for medical practice in this evolving landscape.
One such example are the incessant advocacy efforts of the Telemedicine Society of India (TSI) that have paid off with the approval of Telemedicine Practice Guidelines by Ministry of Health and Family Welfare, Government of India in March 2020. TSI, now with an enhanced vitality is determined to reduce Urban-rural healthcare disparity.
My detailed research has looked at the problem that exists in rural India and why people residing there are hesitant to adapt to telehealth as a prime medium to acquire healthcare services. Thereafter, it goes into further detail of how this can be destigmatised through solutions like overcoming the language barrier, hiring ambassadors for spreading awareness, and regularly updating the content on the company website.
Lastly, it also includes a state-wise analysis of the 11 states that TSI principally targets, which discusses the problem that a certain state faces and a recommended solution for that problem. For example, people in Maharashtra have concerns about the privacy guidelines around the uptake of telemedicine and to resolve this problem, a recommendation was to revise the guidelines to address the weaknesses and to establish an ongoing system of evaluation to permit future improvements in the guidelines to make them increasingly comprehensive.
The recommendations for adaptation of telehealth in rural areas include –
1. proper training of doctors and other healthcare professionals to deliver the telemedicine technology effectively, including vastly improved Internet services;
2. A much higher level of public-private partnerships related to telemedicine activities;
3. Developing more cohesive privacy policies and guidelines for TSI to ensure that patients feel secure and integrate telemedicine with the existing health system;
4. An efficient management structure for monitoring quality standards of telemedicine practice in the country;
5. Efforts should be made to educate public about telemedicine and its related benefits.
This kind of research was necessary because of the growing relevance of telehealth services in today’s rapidly revolutionising, technology-dependent world. It is also prominent in the situation of the pandemic in which we are living in today, given the requirement to stay at home and reduce physical contact. In terms of focusing on rural areas of India as a prime target audience for this research, there was a crying need for habitants of these areas to accept newer approaches as the world progresses.
To obtain a full copy of my research, please write a mail to my mentors – aks1953@hotmail.com
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
The next annual conference of Telemedicine society of india – the 17th TELEMEDICON2021 will be held in hybrid mode at Lucknow from 12th to 14th November 2021.
TELEMEDICON this year takes special significance as it coincides with the 21st anniversary of our society which was formed in Lucknow in the year 2001. Prof. S. K. Mishra is the Chairman and Prof. P.K. Pradhan the Organizing Secretary for the meeting. You should register for the meeting by visiting https://www.telemedicon2021.com
The big event this month was the launch of the Health card by the GoI on 27th Sept, by our Prime Minister, Mr. Narendra Modi under Pradhan Mantri Digital Health Mission (PM-DHM). During the launch he said: “The drive to strengthen the health facilities of the country, in the last 7 years, is entering a new phase today. This is not an ordinary phase. This is an extraordinary phase.”
Under this scheme, now every citizen in India will have a separate health ID. The Health ID will have a unique 14-digit health identification- for every citizen that will also work as their health account. This would help give a big boost to the ‘Digital Health’ in India. The key objectives are as follows:
The national Health ID will be a repository of all health-related information of a person. The health ID will enable access and exchange of longitudinal health records of citizens with their consent.
Healthcare Professionals Registry (HPR) and Healthcare Facilities Registries (HFR) that will act as a repository of all healthcare providers across both modern and traditional systems of medicine.
This health account will contain details of every test, every disease, the doctors visited, the medicines are taken, and the diagnosis. This information will be very useful as it will be portable and easily accessible even if the patient shifts to the new place and visits a new doctor.
The personal health records will be linked and viewed with the help of a mobile application;
Ayushman Bharat Digital Mission Sandbox, created as a part of the Mission, will act as a framework for technology and product testing that will help organizations, including private players, intending to be a part of National Digital Health Ecosystem become a Health Information Provider or Health Information User or efficiently link with building blocks of Ayushman Bharat Digital Mission.
This Mission will create interoperability within the digital health ecosystem, similar to the role played by the Unified Payments Interface in revolutionizing payments. Citizens will only be a click-away from accessing healthcare facilities
Thank You Dr. Sunil Shroff Chief Editor President – TN Chapter – TSI
History of Telemedicine @ Apollo Hospitals India
Prof. K. Ganapathy Former Secretary and Past President Neurological Society of India, Telemedicine Society of India & Indian Society for Stereotactic & Functional Neurosurgery | Hon Distinguished Professor The TamilNadu Dr. MGR Medical University | Member Roster of experts Digital Health WHO | Director, Apollo Telemedicine Networking Foundation & Apollo Tele Health Services | URL: https://kganapathy.in |Email: drganapathy@apollohospitals.com
Chronicle of events
Sep 16th 1996 – The compiler of this chronicle delivered an Institute Lecture @ IIT Kanpur at 8pm. . Prof K. Srivathasan then HoD EE introduced him to the word Telemedicine and persuaded him to jointly prepare a project report from 10.30pm to 4am immediately after the lecture !!!….Readmore
Informed Consent for Telemedicine
Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist Law Firm Eshika Phadke Associate, Arogya Legal – Health Laws Specialist Law Firm
The Telemedicine Practice Guidelines specify that consent may be implied when a patient initiates a teleconsultation; however, there are certain situations wherein a doctor is legally required to obtain consent from the patient… Readmore
Problems that exists in Rural India to Adapt Telehealth
Telemedicine has recently emerged and gained popularity as a new hope to remove the bottlenecks in the healthcare seeking. While telehealth technology and its use are not new, widespread adoption among patients, especially in rural areas, beyond simple telephone correspondence has been relatively slow…Readmore
Telemedicine Practice Guidelines – A Foundation Course for RMPs by TSI
CoWIN develops API to track COVID vaccination status in India First unveiled in January, the CoWIN portal has now launched a new feature called Know Your Customer’s Vaccination Status (KYC-VS). Spotted by Republicworld, the new tool was announced by the Union Health Ministry of India on September 10. It will now enable companies to check the vaccination status of individuals via the official CoWIN portal. … Read More
Kotak, IISc to set up AI, machine learning centre in Bengaluru Kotak Mahindra Bank and the Indian Institute of Science (IISc) on Thursday announced a partnership to set up an Artificial Intelligence & Machine Learning (AI-ML) Centre at the IISc campus in Bengaluru… Read More
94% Indian healthcare leaders want to invest in AI technologies: report NEW DELHI : At least 94% of Indian healthcare leaders would most like their hospital or healthcare facility to invest in Artificial Intelligence (AI) technologies in the near future, the Future Health Index (FHI) 2021 India Report released by the Royal Philips a global player in health technology on Thursday, said… Read More
International
World’s First AI Developed to Treat Covid-19 Patients Worldwide Artificial intelligence (AI) has been used by Addenbrooke’s Hospital in Cambridge along with 20 other hospitals from across the world and healthcare technology leader, NVIDIA, to predict Covid patients’ oxygen needs on a global scale… Read More
AI Algorithm to Treat Psychiatric Illness, Stroke Google and Mayo Clinic researchers partner to develop new artificial intelligence (AI) algorithms to improve brain stimulation devices to treat people with psychiatric illness and direct brain injuries, such as stroke… Read More
Study shows success of hybrid in-person, telemedicine model of vitreoretinal care A hybrid model of patient care, combining telemedicine and traditional face-to-face visits, may offer the best of both worlds, minimizing the risk for disease transmission while maximizing practicality and patient safety… Read More
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- www.medindia.net
Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist Law Firm
Eshika Phadke Associate, Arogya Legal – Health Laws Specialist Law Firm
The Telemedicine Practice Guidelines specify that consent may be implied when a patient initiates a teleconsultation; however, there are certain situations wherein a doctor is legally required to obtain consent from the patient.
Consultation not initiated by the patient If someone other than the patient – including their family member, a healthcare professional, another doctor, or even the doctor who is consulting the patient themselves – initiates the consultation, explicit consent must be taken from the patient.
If a healthcare professional seeks a medical consultation for a patient through telemedicine, both the healthcare professional and the consulting doctor would need to obtain explicit consent from the patient. The healthcare professional would be required to counsel the patient on the risks and limitations of telemedicine, and the doctor would be required to seek the patient’s consent to proceed with the consultation.
No capacity to consent If the patient is a minor or does not have the mental capacity to legally provide consent, the person’s caregiver is authorised to consult with a doctor and take decisions on their behalf. However, the doctor must first confirm that the person is the patient’s caregiver by asking to see either a formal authorisation to that effect, or a government-issued document that establishes the person’s relationship with the patient. This would not be required if the doctor has previously treated the patient in-person, and is aware of their relationship with the caregiver. For the sake of documentation in such cases, the doctor ought to record that they have treated the patient in-person prior to the teleconsultation, and may even request that the caregiver confirm the same through a text message or email.
Recording If the doctor will be recording the consultation, they ought to inform the patient and seek their consent for the same. This is especially vital for specialists like psychiatrists, venereologists, gynaecologists, etc, who discuss highly sensitive and personal information and may receive private visuals from the patients.
Refusal to comply If the doctor is of the impression that the patient ought to go for an in-person consultation for their condition but the patient refuse, the doctor should inform them of the risks and consequnces of not seeking in-person treatment. If the patient still refuses, the doctor should require the patient to send a statement that they were informed of the risks and elected to proceed with the teleconsultation against medical advice in writing or as a voice note, and the doctor should preserve the consent with the records that he/she maintains for the consultation.
Transmitting Prescription to Pharmacy If the doctor issues a prescription post a teleconsultation and the patient wishes that the prescription be sent directly to a pharmacy of their choosing, the doctor must obtain explicit consent from the patient prior to doing so, since without consent, the act of transmitting a patient’s prescription to a pharmacy would constitute a breach of confidentiality.
Support groups If the doctor starts virtual support groups for patients suffering from or people affected by a disease/condition where they will be sharing information and/or allowing the group members to provide emotional support to one another, the doctor must seek explicit consent from a patient/person before adding them to the group, since the patient’s identity would be revealed to other members of the group, and confidentiality would thus be compromised.
Limitations of Telemedicine It is advisable that doctor’s refrain from tending to spontaneous teleconsultations unless it is an emergency; they should put in place a process whereby the patient takes an appointment. Along with the appointment confirmation, the doctor should send a brief statement outlining the risks and limitations of teleconsultation, and informing the patient that by proceeding with the consultation, they are providing their consent.
How to record consent For the teleconsultation itself, the consent will be implied if a patient proceeds to initiate the consultation after being informed of the risks involved.
For situations where explicit consent is required or advisable, the doctor may ask the patient to record it in any form – they could send an email, text, audio note, video recording stating that they are providing their consent for telemedicine (and any other context that may be required). The doctor must always record the fact of receipt of consent in his notes which should be preserved with the patient’s records.
Prof. K. Ganapathy Former Secretary and Past President Neurological Society of India, Telemedicine Society of India & Indian Society for Stereotactic & Functional Neurosurgery | Hon Distinguished Professor The TamilNadu Dr. MGR Medical University | Member Roster of experts Digital Health WHO | Director, Apollo Telemedicine Networking Foundation & Apollo Tele Health Services | URL: https://kganapathy.in| EMail: drganapathy@apollohospitals.com
Chronicle of events
Sep 16th 1996 – The compiler of this chronicle delivered an Institute Lecture @ IIT Kanpur at 8pm. . Prof K. Srivathasan then HoD EE introduced him to the word Telemedicine and persuaded him to jointly prepare a project report from 10.30pm to 4am immediately after the lecture !!!.
Nov 1996 – Made a formal proposal along with Prof Srivathsan to Dr P C Reddy, Chairman Apollo Hospitals to do a pilot project @ Apollo Hospital Nellore . Prof Srivathsan and I even chose the room in Nellore !! However it did not fructify . We were too far ahead of the times!
April 1998 – Dr Reddy asked the author if he was still interested in Telemedicine. Ms Sangita Reddy had persuaded ISRO to use a VSAT for Telemedicine purposes @ the new secondary level hospital in the village of Aragonda ( near Chitoor) the birth place of Dr Reddy.
March 24th 2000 – The world’s first Teleconsultation from a village hospital thro amn ISRO enabled VSAT was commissioned by the then US president Bill Clinton from Hyderabad in the presence of the then Chief Minister Sri Chandrababu Naidu
In 2001 – Apollo Telemedicine Networking Foundation was formally established as a not for profit Section 25 company. Spoke in the first intercontinental live multipoint telemedicine symposium on June 19 2001. Bill Gates was also a speaker . Initiated teleconferences with, Japan, USA, Saudi Arabia and Hong Kong.
Feb 15 2002 – Apollo SHAR Telemedicine project commissioned by Chairman ISRO . ISRO convinced that Telemedicine was doable and took it up as a major initiative.
April 2002 – Addressed 600 principals of Engineering Colleges @ Anna University on Telemedicine. Subsequently started Telemedicine units in 5 Engineering colleges !!
May 2002 – Assisted ATnKK Area in Southern Command. Indian Army to set up Telemedicine units
2003 – First formal University accredited 4 week certificate course on Telehealth technology was started with Anna University. Featured in Govt of India Documentary India 2.0
2004-05 – Clinically validated Telemedicine enabled peripheral medical devices for IITM start up REMEDI
2005 – VSAT enabled Hospital on Wheels commissioned at Madurai . Became first Treasurer and Joint Secretary of TSI with Reg No 001 ATNF also became first institutional member of TSI
2006 onwards – Evangelisation on mission mode ! Talks given all over India and overseas creating awareness . Large number of VIP’s and VVIP’s visited the Dept to see Telemedicine in action . ATNF became a member of the Standards Committee on Telemedicine, the National Task Force on Telemedicine, the Working Group on Telemedicine of the Planning Commission, and the SARC Committee.
August 2007 – Assisted Ericsson in demonstrating wireless transmission of heart sounds etc thro 3G for the first time in South Asia
Nov 2007 – International Conference on Telemedicine at Chennai 350 attended including 35 from overseas
2009 – MEA Govt. of India initiated the Pan Africa e-Network project for teleconsultations ATNF was part of the steering Committee and an active participant
2010 – Commenced “Transforming Health Care with IT” international conference held annually till 2019
2010 – Creation of Apollo Telehealth Services Pvt Ltd with a full time CEO and support staff
2011 – eHome Visits initiated in Chennai won Best Post Poster award Washington DC
2012 – 527 patients in 13 different specialities were connected simultaneously to six tertiary Apollo hospitals, from a Hospital on Wheels @ a mega health camp in Ajmer 11th /12th February. A world record then.
2014 – Patient empowerment in rural India – project with MS Swaminathan Research Foundation promoting eHealth Literacy thro internet enabled Village Resource Centers > 26,000 from 13 villages have attended
2015 onwards International Educational Activities with various Management Schools including London School of Economics, Harvard , Columbia etc , Chosen as case study to illustrate Global Best Practices by Columbia University
eICU’s 20 smaller ICU’s connected to Apollo Hospitals Hyderabad 1200 plus teleICU consults in subspecialities given.
Public Private Partnerships a) Himachal Pradesh . Four Telemedicine Centres in the Himalayas and the world’s first 24/7 Tele emergency Services . About 30,000 teleconsults already provided . b) >1.2 million teleconsultations provided under the Mukhyamantri Arogya Kendram (e-UPHC)- project covering 182 Centres from October 2016.c) Jharkhand Digital Dispensaries programme In first 15 months 328,648 patients attended d) Uttar Pradesh Telemedicine programme in the first one year 141,793 patients visited 114 Government Community Health Centres e) Uttar Pradesh Teleradiology PPP program has 127 teleradiology centres in rural UP with 400 images reported daily with turn around time < f 4 hours f) Tele Opthalmology Through 115 existing Community Health Centres / Vision Centres in 13 districts,5 million patients screened in 2 years. Thro Mukhyamantri e-Eye Kendram or MeEK project 405,000 fundus examinations were done remotely by 30 Opthalmologists from Chennai.
2019 Only medical paper presented @ International Conference on Human Spaceflight Programme organised by ISRO.
2021 Since inception over 400 papers have been presented in various regional, national and international meetings held in India and 105 held overseas . Over 180 articles have been published on Telehealth besides 45 in peer-reviewed journals and 12 chapters in textbooks. Several national and international awards have been received.
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
Launch of Telehealth Diabetes Online Course by TSI
In its pursuit to promote telehealth training, Telemedicine Society of India has been conducting training for telemedicine since April 2020.
On the 30th July, during the 8th Edition of Dr. Mohan’s International Diabetes Update, the society launched Telehealth Diabetes online course for medical practitioners.
This is the second online course on Telemedicine launched this year by TSI. The course has interactive video lectures, power-point presentations and theory material and is divided into four broad segments as follows:
Module I- Introductory Primer to Tele-Diabetes Module II. Setting up a Diabetes & Telehealth Practice Module III- Legal & Ethical Aspects Module IV – Optional Material
The total duration of this online course is four to six hours with post course assessment to get a proficiency certificate of completion of the course. The specialist course faculty include – Dr. V. Mohan, Chennai Dr. Jothydev Kesavadev, Trivandrum Dr. Sanjay Sharma, Bengaluru
Thank You. Dr. Sunil Shroff
Chief Editor
President – TN Chapter – TSI
Webinar on ‘Ethical Issues in Telehealth Practice’
Dr. S. K. Mishra
Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow.
SGPGIMS has been conducting seminars on various aspects of healthcare and medical ethics. On August 14th, 2021, another program in this series was conducted through Videoconferencing on Ethical Issues in Telehealth Practice’. Telehealth is one of the evolving information technologies and COVID-19 pandemic has accelerated the use of telehealth globally. Telehealth can help decrease the burden of the healthcare system to a large extent. Prof R K Dhiman, Director, SGPGIMS, welcomed the participants and said that SGPGIMS has been a front-runner in establishing Telemedicine services not only for the Institute but also all over the country. He shared his experiences and informed that telemedicine is an important modality in patient care. Prof Vinita Agrawal, faculty in charge Bioethics cell SGPGI and moderator of the program, said that telehealth services can now aim not just for ‘sick care’ but also for ‘health care’. However, certain ethical concerns need to be understood for the use of this important technology as a means to improve access and quality of healthcare for all members of our society.
Prof S K Mishra, ICMR, Emeritus Scientist at the School of Telemedicine and Bioinformatics, SGPGIMS, who established the SGPGI telemedicine training and research facility, introduced the speakers and discussed the ethical aspects in Telemedicine. Dr Sunil Shroff, Managing Trustee of the MOHAN Foundation, a NGO that pioneered organ donation in India, talked about the scope of Telehealth and informed that the Telemedicine practice guidelines of the MoHFW discuss and cover the various ethical issues related to the use of telemedicine. Dr K Ganapathy, from the Apollo Telemedicine Network Foundation, said that the man behind the technology is more important and emphasized the need of maintaining standard of care and webside manners. Dr BN Mohanty, Honorary Advisor on Telemedicine to the Govt. of Odisha, talked about the responsibility of stakeholders to facilitate Ethical practice of Telehealth. The participants joined the program from within the institute and from the NMCN network. It was also streamed on YouTube.
Confidentiality and Data Protection in Telemedicine
Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist Law Firm
Eshika Phadke Associate, Arogya Legal – Health Laws Specialist Law Firm
As a concept, doctor-patient confidentiality is well established and widely understood by the medical fraternity. The principle, which is laid down in the MCI Code of Ethics, 2002 and the declaration that doctors take at the time of registration, also forms a part of the Charter of Patient Rights.
A doctor is duty-bound to maintain all information that a patient shares with him/her in utmost confidence irrespective of whether it pertains to their medical treatment itself or to their personal or domestic lives. The exception, of course, is when the doctor is of the opinion that keeping the information confidential would cause harm either to a specific person or society at large. This obligation has been explicitly adopted under the Telemedicine Practice Guidelines. While confidentiality has evolved to cater to telemedicine, it is still intuitive for doctors. However, data protection, which in the digital age goes hand in hand with confidentiality, is a new compliance for doctors.
The information that is collected in the course of a medical consultation (online or in-clinic), procedure, pathology or diagnostic test is recognised as “sensitive personal information” under the Indian data protection laws. This includes cases notes, test reports, diagnostic images, recordings, etc. Protecting this data has always been of utmost importance since a data breach would result in confidentiality being compromised. With the changes in the delivery of medical services, the responsibility of ensuring that the data is properly protected no longer vests only with the hospital administration.
The Telemedicine Practice Guidelines explicitly specify that doctors are required to comply with the data protection law, namely the Information Technology (Reasonable Security Practices and Procedures and Sensitive Personal Data or Information) Rules, 2011. While this may sound overwhelming, it is actually quite straightforward. The law merely expects that a person, in this case the doctor, takes reasonable actions and adopts appropriate systems to ensure that the data that they collect is with the consent of the person (i.e. the patient) and is protected. With clinics and telemedicine platforms becoming a lucrative target for cyberattacks, it is especially important to be cognisant of the best practices. The extent to which a doctor would need to be involved with data protection would vary.
All doctors who are offering teleconsultations in their individual capacity are responsible for ensuring compliance. First and foremost, their devices and browsers should be protected by a security software. If they are offering consultations via third-party text-based services, or video calling services, they must ensure that the service provider’s terms and conditions do not prohibit the use of the platform for telemedicine. If the consultations or information exchange is taking place via email, they must ensure that their email provider is reliable, that they use a strong password for the account and do not allow anyone else to access it. If the doctor offers consultations through their own website, they must ensure that suitable data protection systems are built in, and that they have a clear policy on the website outlining how the data is handled.
If a doctor is consulting through a telemedicine platform/aggregator or a hospital’s telemedicine services, it is most likely that the platform itself is looking into data protection. In such cases, the doctor should familiarise themselves with any restrictions that the platform may have placed to ensure patient data is protected. For example, several platforms prohibit doctors from storing patient records locally on their device and require that everything be stored on the platforms’ servers. Doctors should strictly comply with these restrictions, since failure to do so would weaken their defence in the event that a data breach occurs.
Remember that a doctor will not be held responsible for a breach of confidentiality, provided that he/she can prove that the breach of confidentiality was the result of a technological failure or the wrongdoings of a person other than the doctor. The caveat is that the doctor should be able to show that he/she has done their due diligence while selecting the technology service to use.
The takeaway is that prior to registering with a provider (which could range from a simple chat service provider to a dedicated telemedicine platform), the doctor should read the privacy policy to ensure that the data is being suitably handled to minimise the risk of data breaches.
References:
Indian Medical Council (Professional Conduct, Etiquette and Ethics) Regulations, 2002
Telemedicine Practice Guidelines, 2020
Charter of Patient Rights (adopted by the National Human Rights Commission)
Information Technology (Reasonable Security Practices and Procedures and Sensitive Personal Data or Information) Rules, 2011
ISRO’s contribution for Indian Telemedicine Program from Concept to completion – Towards National Adaptation
Dr. L.S.Satyamurthy
Former Program Director, Telemedicine, ISRO.
Preamble
It was in November 2001 when I had just returned to India completing my Diplomatic assignment as Counselor of Space, Science and technology, at the Embassy of India, Washington D.C, USA. The then Chairman of ISRO, Dr.K.Kasturirangan called me and said “there is talk of technology and benefits of telemedicine services in the advanced countries like US, Europe, Russia and Japan and they have already initiated the Telemedicine programs. NASA and ESA have started projects which was a part of Space Medicine program for the benefiting the public at large and we at ISRO should not lag behind. As the Indian Space program is basically an application-oriented program for national development and as we are the custodians Satcom technology, we should move forward immediately and take up the challenge of ushering health care for the remote, distant and underserved rural population of our country through the power of Telemedicine using Satellite communication. “That was the beginning of the momentous Telemedicine/Tele health movement in India and rest is history”.
The daunting task of Telemedicine Program conceptualization, formulation and implementation in India was primarily spearheaded by the Indian Space Research Organization ( ISRO ) along with the support of some Govt and private hospitals, dedicated Doctors, Technologists, State governments and Health Administrators. The Telemedicine being new and a technology-based healthcare delivery system, the challenges for implementation and adaptation needed to be comprehensively addressed since the health care in India is a State subject whereas Central government being for national policies and funding.
Beginning
ISRO initiated Telemedicine program under Space Technology applications for societal benefits in the year 2001 adopting multipronged strategy of addressing some of the important issues like:
Resistance to change to new system of functioning and lack of infrastructure
Technology adaptation and evolving National Standards for Telemedicine practice
Creating awareness among Public, Doctors, Hospitals and Health administrators
Judicious application of Telemedicine technology at appropriate levels of healthcare system
Cost of service vis-à-vis affordability,
Sensitivity to fast changing technology and its obsolescence,
Training aspects for Doctors/ paramedics in the usage of the new technology in Medical care
Evaluation of Telemedicine service and community satisfaction.
The Telemedicine pilot project era started by ISRO in 2001 culminated into operationalization of telemedicine network in different states of our country during the year 2005-2008. The important factor of providing satellite connectivity free of charge by ISRO, Govt of India was the major boon for many of the specialty hospitals and state governments hospitals to come together in providing health care service through telemedicine for the benefit of rural and underserved population.
Telemedicine Implementation
ISRO’s Telemedicine network covered several states of J&K, Karnataka, Kerala, Maharashtra, TN, AP, Orissa, Jharkhand, Rajasthan, Gujarat, Chhattisgarh, MP, Punjab, Haryana, Uttarakhand, Jammu, Kashmir, Ladakh and North eastern states; UT of Andaman, Lakshadweep Pondicherry, Diu, Daman and Sylvasa connected to50 Specialty/Medical college Hospitals.
That was how ISRO started implementing the Telemedicine program during 2001 -2008 with the assistance of several medical institutions namely: AIIMS Delhi, SGPGI Lucknow, PGI Chandigarh, JIPMER Pondicherry, SRMC Chennai; Several State govt District/Taluk hospitals all over the country including North eastern states, Jammu, Kashmir and Ladak and Union territories of Andaman and Lakshadweep ; specialty hospitals like , Jayadeva Institute of Cardiology, Narayana Hrudayalaya, Sathya Sai and Fortis hospitals in Bangalore; Apollo, Shankara Netralaya, SRMC, Mohan Diabetic foundation at Chennai, Aravind Eye care and Meenakshi hospitals clinics in Madurai and Coimbatore, LV Prasad Eye care in Hyderabad; Amritha institute, Kochi; KEM, Tata Memorial Cancer Centre and Nanavathi hospital in Mumbai, Gangaram and Safdarjung Hospital in Delhi ; Armed Forces medical hospitals at he forward areas including Srinagar, Uri, Udhampur Kargil and Parthapur (Siachen) connected to R & R hospital Delhi and some of the IAF regional hospitals linked to Command hospital, Bangalore.
Further, ISRO provided the assistance for setting up of Telemedicine center at Kabul in Afghanistan under WHO sponsorship and at Male in Maldives under MEA sponsorship.
During the Tsunami in 2005, ISRO’s Telemedicine network provided the Satcom link for Andaman and Nicobar Islands were provided for both Telemedicine service and telecom support for connecting the mainland of India. ISRO was responsible for preparing the first project report for Pan Africa Telemedicine Project covering 48 countries in Africa on the advice of the then President A.P.J.Abdul Kalam, under MEA sponsorship, which was subsequently executed by TCIL, Delhi.
Other effort included Satcom linked Mobile Telemedicine Bus/Vans set up by ISRO in association with leading specialty hospitals covering various Medical disciplines like Ophthalmology, Diabetology, Cardiology, Mammography, General Medicine and Surgery and rural community.
ISRO virtually marshalled the various stake holders on a common platform for the cause of ushering healthcare to the remote, rural and underserved population of the country. During Tsunami in 2005 ISRO set up emergency satellite links to provide emergency care connecting the main land.
During that time 2005-2008, India had one of the largest Satcom based Telemedicine networks in the world network with about 400 remote/ rural/ district hospitals and 200 Village resource centers in most of 25 States connected to 50 Specialty/Medical college hospital located in major cities/towns in the country including 15 Mobile units covering the various medical specialties.
More than 10 Lakhs of Teleconsultation took place with several life saving instances during the period of 2002-2010.
Outcome of ISRO’s Initiative:
ISRO’s Telemedicine program initiatives resulted in the formation of National taskforce by the Ministry of Health in 2006, Government of India, for formulating policies and guidelines for ushering Telemedicine into the mainstream of health care delivery and future implementation in different states by the health ministries and departments. This also lead to Health Ministry, GOI, recognizing Telemedicine as an important application under National Health Mission (NHM) of the country under Ayushman Bharath.
Today many of the State Govt and Private along with the Specialty hospitals are proving Telemedical services with different connectivity options like Wireless and Mobile, to needy patients on clear business model as applicable for reaping the benefits of the initiatives ushered by ISRO.
Telemedicine Practice Guidelines – A Foundation Course for RMPs by TSI
Feedback for Telemedicine Practice Guidelines Course
The foundation online course for Telemedicine Practice Guidelines being conducted by TSI has been taken up by almost 160 registered medical practitioners. The feedback of the course has so far been excellent. To view these feedbacks please visit – https://tsi.org.in/course-feedback/
A snapshot is presented a below:
1. Did you find the live interaction useful?
2. Were most of your doubts cleared regarding telehealth practice?
3. Do you feel more confident to practice safe telemedicine?
4. Overall rating
Telemedicine – News from India & Abroad
India
India launches incentive scheme supporting 75 startups in telemedicine and digital health
WHAT IT’S ABOUT The announcement comes as India celebrates its 75th year of independence from the United Kingdom. Amid the celebration, Science and Technology Minister Jitendra Singh said identifying and supporting the 75 startups is the ministry’s “most appropriate” task that will promote research and development in the healthcare sector… Read More
International
Artificial Intelligence (AI) Enhanced Through Brain Networks
Cognitive tasks can be performed efficiently using artificial intelligence (AI) networks based on human brain connectivity as per a study at the Mcgill University, published in the journal Nature Machine Intelligence… Read More
New AI Blood Test for Lung Cancer Detection
A novel artificial intelligence blood testing technology can detect over 90% of lung cancers in samples from nearly 800 individuals with and without cancer. ‘The DELFI technology blood test for lung cancer can be a good way to enhance screening efforts.’… Read More
Mobile telemedicine unit found to be effective in treating opioid use disorder in rural areas
Rural regions in the U.S. have been disproportionately affected by the opioid epidemic, while also having the fewest number of programs to treat opioid use disorder. In an effort to remedy this dire health issue, University of Maryland School of Medicine (UMSOM) researchers reconfigured a recreational vehicle (RV) as a telemedicine mobile treatment unit to determine whether it could provide effective screening and treatment to individuals with opioid use disorder in rural areas… Read More
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
We had an excellent webinar on telemedicine technology by Mr. Mathur from Ahmedabad and the report is covered in this newsletter.
The self-learning course with live interaction with the course faculty has been already upgraded to Ver.2 with more interactive lecture videos to provide better learning experience.
The online self-learning course ‘Train to Practice Telemedicine’ is a foundation course for all practicing RMPs.
This month we are also launching a speciality course on diabetes and telehealth with help of Dr. V. Mohan, Dr. Jothydev Kesavadev, and Dr. Sanjay Sharma.
Please visit https://tsi.org.in/courses to view all the courses. If you wish to contribute as a TSI member you are most welcome to join us in development and delivery of these courses.
Thank You. Dr. Sunil Shroff
Chief Editor
President – TN Chapter – TSI
Tele Rehabilitation : The Time has come
Prof. K. Ganapathy
Former Secretary and Past President Neurological Society of India, Telemedicine Society of India & Indian Society for Stereotactic & Functional Neurosurgery | Hon Distinguished Professor The TamilNadu Dr. MGR Medical University | Member Roster of experts Digital Health WHO | Director, Apollo Telemedicine Networking Foundation & Apollo Tele Health Services | URL: www.kganapathy.com | EMail: drganapathy@apollohospitals.com
“If I had known I was going to live this long, I would have taken better care of myself.” – Mae West
Rehabilitation, the process of restoring an individual to health or normal life through training and therapy, is a major component of Health Sciences. Rehabilitation services have been disrupted due to the COVID-19 pandemic. Even with unlocking and post vaccination, some form of physical distancing is likely to be part of the new normal. This review suggests that, Telerehabilitation (TR) will soon be a distinct stand alone sub speciality of Telehealth and is here to stay.
Introduction to Telerehabilitation Services
Digitalisation of health care is at an all time high, as is the exponential growth of Telehealth. TR is “the delivery of rehabilitation services via Information and Communication Technologies” . Reduced access to in-person rehabilitation, secondary to the pandemic, is resulting in TR growing exponentially. TR services include evaluation, assessment, monitoring, prevention, intervention, supervision, education, consultation, and coaching. TR services can be deployed across patient populations and multiple healthcare settings including clinics, homes, schools and community-based worksites. A Fortune Business Insights Report estimated a market value of USD 3.32 billion in 2019,with a Compounded Annual Growth Rate (CAGR) of 13.4% leading to USD 9.13 billion by 2027.
Advantages and Barriers in TeleRehabilitation
These include exercising from comfort of home, ability to work on one’s recovery irrespective of time schedule of health care professionals and improved quality of exercise instruction, as they are available for repeated review on video format. Access to high-quality care despite geographical isolation, reduced travel and waiting time, flexibility, and cost-effectiveness are additional benefits Limited computer literacy, unreliable internet connection, language barrier, inability to perform an actual physical assessment, patient privacy, and safety concerns are challenges Some participants were enthusiastic about TR as they could be in contact with their therapist and continue training.
Clinical indications for TR include musculo skeletal disorders, low back ache, spondylosis, osteo arthritis, neck pain ,frozen shoulder and post joint replacement. Neurological conditions benefiting from TR include stroke, neuro trauma, neuro degenerative disorders, cerebral palsy, Post TB Meningitis, neuro muscular disorders, Gullian Barre syndrome, Deuchenne muscular dystrophy and demyelinating diseases. Chronic Obstructive Pulmonary Disorders, post ICU conditions, post Covid, cardiovascular disorders, visual, hearing, developmental disorders, speech and voice dysfunction, swallowing disorders and cognitive dysfunction also benefit from TR . Virtual assessments for pain, swelling, range of motion, muscle strength, balance, gait, and functional assessment demonstrated good concurrence with physical assessments. TR can provide high-quality personalized musculoskeletal physiotherapy. Knee osteoarthritis causes musculoskeletal pain and disability affects up to one-third of people aged over 60 years. Remote muscle strengthening exercises can significantly reduce pain, improve physical function and quality of life. TR for musculo skeletal conditions leads to reduced hospitalization and crowding in physio therapy departments. Musculoskeletal disorders (MSDs) are the second commonest cause of chronic pain and physical disabilities. Physiotherapy assessments that can be done through video include evaluation of pain, swelling, range of motion, muscle strength, balance, gait and functional assessment . TR for stroke, cardiac, pulmonary afflictions and swallowing difficulties
Tele Rehabilitation potential in India
India now has over 100 million senior citizens. The market for geriatric rehabilitation alone is high. Confederation of Indian Industries, in a report showed that 5.5% of seniors were staying at homes. 6% of seniors live alone. Of the 700 million active internet users, 70% access the internet daily mostly using mobiles. Interestingly communication technology is growing faster in rural rather than urban areas. were using smartphones in 2020. 77% of 500 million smartphone users were accessing broadband services. The National Institute of Mental Health and Neuro Sciences (NIMHANS), services delivered telemental health services during the COVID-19 crisis to ensure continuity of care for patients who were unable to avail outpatient services .. A report on 22 senior citizens from four Community Centers in Delhi showed that home-based TR could be used as an adjunct to continue follow up care thus improving outcomes.
Tele Rehabilitation; A peep into the Future
TR will eventually be integrated with Smart Homes in Smart Cities. Functional monitoring with bed sensors, activity/motion sensors and gait monitors will be a reality. This will be followed by Creating a connected home with pressure-sensing floors, smart furniture and medical sensors. Assistive robots, power wheelchairs, prosthetic limb controls, Home Automation systems and AI Chatbot companion at Home will add value providing “smarter care”. This will include encouraging activities and contacting caregiver/children in emergencies. Staying @ Home, better known as aging in place will lead to better health outcomes.
Conclusion
Understanding who will use TR, how it will help achieve customized, well defined and changing goals is critical. Beneficiary’s goals alone matter. TR is only a tool to achieve them. The Health Care Provider using TR should get into the minds of the the end user. It should never be forgotten that for digital natives, an octogenarian is from another planet. “Customer delight” is not a cliché used as a marketing ploy. TR is not a solution searching for a problem. Nothing can stop an idea whose time has come. Covid has ensured that Telerehabilitation is here to stay.
Telemedicine and Its Applications for the Common Man during COVID Pandemic – A three-day virtual online lecture series by ISIE Ahmedabad
Mr. Anil C. Mathur Group Director (Retd.),Space Applications Centre, ISRO, Ahmedabad | MD, Indian Space Industries Exhibitors, Ahmedabad-Ghaziabad | Email: antrixudyog@gmail.com
In this era of digital world, technology is going to play a big role in establishing India as a superpower. Telemedicine is one such area. Telemedicine, also known as telehealth or e-medicine, is the remote delivery of health services, including examinations and consultations, on telecommunications infrastructure. Telemedicine is the practice of medicine using technology to deliver care remotely. A physician at one location uses a telecommunications infrastructure to provide care for a patient at a distant location. Telemedicine allows healthcare providers to evaluate, diagnose and treat patients without the need to meet in person. Patients can communicate with physicians from their homes using their own personal technology or by visiting a dedicated telehealth kiosk.
A three-day virtual online lecture series on the theme “Telemedicine and Its Applications for the Common Man during COVID Pandemic” was organized by Indian Space Industries Exhibitors (ISIE) Ahmedabad from 10 July 2021 to 12 July 2021. ISIE is a micro-venture established under Micro, Small and Medium Enterprises (MSME). This organization has been founded by Mr. Anil C. Mathur, retired group director, ISRO Ahmedabad and alumnus IIT Roorkee. From the very beginning, ISIE has encouraged the public especially scientists, students, science communicators to adopt science and technology applications in daily life.
The programme was virtually inaugurated on the Zoom stage by the Chief Guest Shri B. S. Bhatia, Former Director,DECU/ISRO, Ahmedabad. In the inaugural session, Mr. Bharat Mehta, Editor-in-Chief of the journal “Space Industry” published by ISIE, gave information about the activities of ISIE and repeated strongly, the goal of all the organizers to bring the activities and benefits of space science and technology to the common man of the country. The Chief Guest of the inaugural session Shri B. S. Bhatia expressed his thoughts on the importance of telemedicine for shaping the diverse possibilities of a futuristically developed world. Mr. Dinesh Kumar, Chairman Institute of Engineers Delhi State Centre, also addressed the participants in the inaugural session as a special guest.
In this virtual series of lectures, online addresses were given by eminent doctors, scientists, technical and industrial experts of the country in the sessions organized between 10 am IST to 4 pm IST on all three days. In this three-day virtual online lecture series, the experts tried to portray the future India’s telemedicine healthcare technology to capture the imagination of the audience, especially the students, by giving their address session wise as follows according to the schedule:
India’s Space programme and History of Telemedicine in India by Mr. A. K. Sangal, Retd. Group Director, DECU/ISRO and former President, Telemedicine Society of India; Telemedicine Society of India , its training activities and Relevance of Telemedicine in the Covid pandemic by Dr. Ashvini Goel, Retd. Colonel (Dr.) Indian Army, and Current President, Telemedicine Society of India; Applications of Telemedicine in Surgical care and Skill transfer by Dr. S. K. Mishra, Founder President, TSI and Senior surgeon and Dean at Sanjay Gandhi PGI, Lucknow; Telemedicine – Accessible and Affordable Healthcare for All by Dr. Sunil Shroff, President Telemedicine Society of India, Tamil Nadu Senior Consultant Urologist Madras Mission Hospital; Role of Videoconference in Telemedicine by Mr. Bijoy M. G., Managing Director, Unarv Telemedicine & Healthcare Services (P) ltd, and Secretary Kerala state chapter of Telemedicine Society of India; Tele-health activities during Covid-19 pandemic-Odisha Experience by Dr. B. N. Mohanty, Hon. Advisor to the Odisha Government and former president of Telemedicine Society of India; Merits, demerits and problems associated with Telemedicine Network and System by Dr. T. N. Ravishankar, Specialized family physician and currently Director Sudar Hospital; Applications and Usage of advanced Artificial Intelligence(AI) technology in Health Care by Dr. Masood Ikram Doctor turned entrepreneur and expert in applications of AI in the Healthcare industry; Telemedicine-During and after COVID pandemic by Dr. Sanjeev Mehta Senior pathologist, Ahmedabad and Member Telemedicine Society of India; ISRO’s Telemedicine Network by Mr. Arvind Tyagi Scientist/Engineer, DECU/ISRO, Ahmedabad; NavIC, Telemedicine and the COVID by Dr. M. R. Sivaraman Retired Scientist/Engineer ‘G’ and DPD, SAC/ISRO, Ahmedabad; Lessons from Covid-19 for Community enabling to counter infodemic by Mr. J. Venkataramaiah, Retd. Sci./Engr. ISRO. Alumni & Mentor, International Space University. Currently associated with PSF; Clinical Applications of Telemedicine by Dr. N. K. Agarwal Professor of Endocrinology and Nodal Officer of Regional Resource Centre of Telemedicine, Institute of Medical Sciences, Banaras Hindu University, Varanasi; Block Chain in Healthcare by Dr. Bhagwant Singh Ratta Pediatric Surgeon/Urologist and former president Telemedicine Society of India; Continuing Medical Education through ISRO’s Telemedicine Network and Tele-consultations during Covid-19 by Dr. Maulesh Gadani, Medical Officer, SAC/ISRO, Ahmedabad; Telemedicine- What really works by Mr. Mayank Agarwal CEO, M/s Smart Square Tech., NOIDA; Televital Journey and Latest Trends in Telemedicine Technology Mr. Sateesh Bhatt Solution Architect, M/s Televital India Pvt. Ltd., Bangalore; Telemedicine and Privacy by Ms. Bagmisikha Puhan, Technology Lawyer and Privacy Practioner, EC member Telemedicine Society of India.
The concluding session of this lecture series on 12th July, was presided over by Dr. Velchamy, Founder ‘Krithin Foundation’, Trichy, Tamil Nadu. Dr. SK Mishra, former Head of the Department of Endocrine Surgery and Nodal Officer Telemedicine Program, S.G.P.G.I. Lucknow; Shri AK Sangal, Former Scientist SAC, ISRO, Ahmedabad; Shri Vikram Desai, Former Director DECU ISRO; Shri VK Jain, President BES Ahmedabad Chapter; Shri Anil C. Mathur, Managing Director, ISIE expressed their views while discussing the future roadmap of telemedicine through panel discussion.
On all three days of the lecture series, BES Ahmedabad Chapter President Shri VK Jain conducted the entire program with technical support from the team of Space Geeks led by the Founder Shri Chintamani Pai, Dr. Vaibhav Rawat and Shri Hari Tejas Iyer. At the end of the program Shri Amritanshu Vajpayee, Founder Coordinator, Ignited Minds VIPNET Club-Farrukhabad presented a formal vote of thanks and then the end of the three day virtual lecture series was announced by the organizers. Due to this unique effort of ISIE in the midst of the worldwide pandemic of COVID-19, this three-day virtual online lecture series can be considered as an effort to reach out to the masses through participating audiences belonging to different fields.
Broadcasters Engineering Society Ahmedabad Chapter, Space Education and Research Foundation, Space Geeks Mumbai, UL Space Club, IITR Alumni Association Ahmedabad, UOR77 Batch Foundation New Delhi, Space Education and Research Foundation Ahmedabad, Ignited Minds VIPNET Club -Farrukhabad were the collaborating organizations as knowledge partners and Sunrise India Samachar – New Delhi was associated as a media partner for the programme. Many serving and former scientists of ISRO as well as representatives of different collaborating institutions graced the occasion. The live broadcast of the event was arranged by the organizers on the YouTube channel of Indian Space Industries Exhibitors, viz., https://youtube.com/c/ISIEIndianSpaceIndustryExhibitors. The entire virtual lecture is available for public viewing on the channel above.
Medical Negligence in the Telemedicine Era
Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist Law Firm
Eshika Phadke Associate, Arogya Legal – Health Laws Specialist Law Firm
In our previous articles, we discussed the legal considerations and compliances that must be followed to practice telemedicine in India. In this article, we are going to examine a less pleasant but equally important subject: how does a doctor protect themselves from allegations of medical negligence while practicing telemedicine?
It is important to first understand what medical negligence is. When a doctor-patient relationship is formed, a duty is cast upon the doctor to act and provide treatment to the patient as per the applicable standards of reasonable care. Any act (including a failure to act) by a doctor that is in a breach of the standard of care, which results in the patient being harmed, would constitute medical negligence.
Standard of reasonable care
The standard of reasonable care that is applicable to a doctor differs based on specialization, level of education and amount of experience, and is ascertained on the basis of what would be considered reasonable by a responsible body of professionals in that specialization for a doctor with ordinary skill.
For telemedicine, the jurisprudence around the “standard of reasonable care” is still in a stage of infancy in India, since telemedicine was only legitimized in March last year. The Telemedicine Practice Guidelines (“Guidelines”) make it clear that the professional and ethical norms that are applicable to in-person care are also applicable to telemedicine, bearing in mind the intrinsic limitations of telemedicine. So, while the principles of medical negligence for traditional consultations remain the same, they must be adapted to virtual consultations.
At a fundamental level, deviating from the practices laid out in the Guidelines would be considered a breach of standard of reasonable care, and if it results in harm to the patient would constitute medical negligence. Doctors should familiarize themselves with telemedicine guidelines for their specialty to get a clear understanding of what is recognized as the standard of reasonable care.
Documentation and Consent
Similar to in-person consultations, documentation is of utmost importance, not only because it is required under the law, but also because it serves as the doctor’s primary defense should a patient make allegations of negligence or deficiency in service in court.
While consent for the consultation is implied when the patient initiates the consultation, explicit consent must be sought in all other cases. For instance, if the patient’s caregiver or another healthcare professional initiates the session. In such cases, consent ought to be recorded. As a precautionary measure, doctors should also record if a patient refuses to act as per instructions, which may result in their condition worsening. In particular, if a doctor deems an in-clinic visit necessary but the patient refuses, the doctor should obtain, in writing, a declaration from the patient that he/she has been informed of the risks of proceeding via telemedicine and has been advised to visit a doctor’s clinic, but is electing to proceed with telemedicine.
Delay in seeking treatment
The most likely scenario that would result in allegations of negligence is if a doctor does not recommend that a patient see a doctor in-clinic, when it is evident that it is required or fails to communicate the urgency with which the patient ought to seek in-person care. If the patient’s condition deteriorates as a result of the delay in receiving the treatment that they require, the doctor with whom the patient did a teleconsultation with will likely be held for negligence.
Incorrect mode of teleconsultation
The Guidelines recognise video, audio, real-time text and asynchronous interactions between a doctor and patient as telemedicine. While a doctor is at liberty to select which mode to adopt, it is essential that they act prudently while doing so and ensure that the mode allows them obtain all the information required to take a decision. If required, it is perfectly acceptable to switch to another mode. If failure to adopt the most appropriate mode results in a failure to diagnose or misdiagnosis or incorrect treatment, it would likely be considered negligence on the doctor’s part.
Prescriptions
It has been held that prescribing a drug without following the due process to arrive at a diagnosis amounts to (criminal) medical negligence. Doctors must be especially wary of this before prescribing a course of treatment via telemedicine, and must ensure that they have gathered all the relevant information (which may include shifting to a different mode of teleconsultation or requesting the patient to visit a doctor for a physical examination, and ordering diagnostic tests) prior to writing the prescription. Doctors should also ensure that they strictly adhere to the limitations specified in the Guidelines in relation to drugs that may be prescribed via telemedicine.
REFERENCES
1.Indian Medical Council (Professional conduct, Etiquette and Ethics) Regulations, 2002. 2.Telemedicine Practice Guidelines 3.Deepa Sanjeev Pawarskar & Anr. v. The State of Maharashtra (Bombay High Court)
Birth of Tele-Radiology (History and Evolution of Telemedicine –9th Milestone)
Dr. Sunil Shroff, MS, FRCS, Dip. Urol (Lond.)
President, Tamil Nadu Telemedicine Society of India,
Editor, www.medindia.net,
Consultant Urologist & Transplant Surgeon, Madras Medical Mission Hospital, Chennai, India (shroffmed@gmail.com).
Tele-radiology has been an integral part of development and advancement of telemedicine. The advantage has been that it can use asynchronous technology of store and forward to transmit the heavy images to another location for reporting. Important early milestones I the development of Tele-Radiology have included –
In 1929 – Dental x-rays were transmitted with the help of telegraph to a distant location
In 1959 – Canadian radiologist reported diagnostic consultations based on fluoroscopy images transmitted by coaxial cable
Radiologist Joseph Gershon-Cohen and inventor Austin Cooley spent 2 years testing a system invented by Cooley to connect Chester County Hospital to Philadelphia, PA, 28 miles away through wire and radio circuits. The early process was described by Bashshur RL as follows:
‘Primitive by modern standards, the equipment consisted of a glass drum with a clamp on top to attach the film while the drum rotated at a uniform speed of 180rpm. A beam of light illuminated tiny elemental areas of the film and picked up by a photo cell inside the cylinder and connected with a preamplifier to produce the full picture. The image was passed through an output amplifier before connecting it to a telephone line or radio transmitter.’
The two authors eloquently described the essence of their invention: “Consultation between the roentgenologist and surgeon, twenty-eight miles apart, took place over the same telephone circuit, with no more delay than a similar consultation would entail with the surgeon and roentgenologist present together in the hospital.”
It was in 1993 that the American College of Radiology (ACR) and the National Electrical Manufacturers Association (NEMA) brought minimum standards for medical images and metadata, with respect to handling, storing, printing, and transmitting images and other medical record information. This was called ‘Digital Imaging and Communications in Medicine’ (DICOM). DICOM is today an internationally accepted standard for medical images and applies to a number of key aspects of the digital radiology enterprise. It also has standards for file format and network communications.
In India, the first successful use of teleradiology transmission was done in 1996 was done from Jankharia Imaging in Mumbai where image was transferred to the homes of the individual doctors for reporting emergency CT scans.
Artificial Intelligence (AI) Unfolds the New Dimension of Social Development ‘Artificial Intelligence (AI) proves as an inevitable tool in achieving Sustainable Development Goals (SDGs – 17 interlinked global goals for a better future). A global virtual event organized by Amrita Vishwa Vidyapeethamprovided excellent and up-to-date research for all AI enthusiasts from the industry, academicians, and students to realize the importance of AI in all fields. ’….. Read More
International
Recent Improvements In Pharmaceutical Sector AI and big data/analytics are identified by healthcare industry professionals as the top technologies that will transform pharmaceutical drug discovery and development processes, according to a survey by GlobalData, a leading data and analytics company……….. Read More
Machine Learning-powered Imaging Helps Diagnose Thyroid Cancer A new non-invasive method to distinguish thyroid nodules from cancer by combining photoacoustic (PA) and ultrasound image technology with artificial intelligence has been devised by scientists…. Read More
AI-powered emotion analysis technology to help diagnose mental health conditions in seniors in Singapore Through video calls, Opsis Emotion AI’s software will be used by counsellers to help diagnose mental health conditions such as anxiety, stress and depression. Emotional analysis technology developed by software solutions provider Opsis Emotion AI will be piloted over the next two years in a programme targeting more than 4,300 seniors in Singapore.….. Read More
New Revelation About Brain Activity During Sleep Using an artificial intelligence approach, scientists at the University of Geneva (UNIGE), Switzerland explained the brain activity during sleep. They provided strange evidence that sorting out of things during the day time takes place during deep sleep by combining functional magnetic resonance imaging (fMRI) and electroencephalography (EEG).….. Read More
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
I am pleased to inform you about the online telemedicine course from TSI for the RMPs. This self-learning course with live interaction with the course faculty became operational this month. The course is called ‘Train to Practise Telemedicine’ and is housed on the learning management platform called MOODLE. In the near future ‘Telehealth speciality courses’ will also be developed. Please visit https://tsi.org.in/courses to view all the courses. If you wish to contribute as a TSI member you are most welcome to join us in development and delivery of these courses.
With the last issue of the Newsletter we have introduced visual abstract of articles. Please find the second visual abstract from TELEMEDICON2020.
We have also shared the Telemedicine course video – we request you to forward this in your groups to make the course popular.
Thank You. Dr. Sunil Shroff
Chief Editor
President – TN Chapter – TSI
Towards Blockchain Based Secure Healthcare Information Systems
Prof. Prabhu Rajagopal Faculty-in-charge, CFI, IIT Madras, Associate, Center for Non-destructive Evaluation
A team guided by Prof. Prabhu Rajagopal, Lead Faculty – Remote Diagnostics at the Center for Nondestructive Evaluation (CNDE), Department of Mechanical Engineering, IIT Madras (IITM) has developed a first-of-its-kind Blockchain-based secure medical data and information exchange mobile application “BlockTrack” currently out on trial at IITM Institute Hospital. The BlockTrack project aims to securely digitize Healthcare Information Systems while ensuring protection of sensitive personal information and medical records by decentralizing the control and ownership of patient data, through a Blockchain-based innovation. Additionally, the algorithm to generate identification codes for users ensures uniqueness across boundaries with very little chance for duplication.
This disruptive innovation opens up the promise of a universal and transferable Healthcare Information Management with a strong emphasis on data privacy, and tracking the spread of infectious diseases across geographies. The Android version of the application has been developed separately for both patients as well as doctors.
(L) Dr. Rebecca Punithavalli, CMO, IITM Institute Hospital with the Doctor app. (R) Team member at the hospital with the Patient app.
Key outcomes from this project are:
Universally Unique Identification: Blockchain-based identifiers that are nearly impossible to duplicate
Interoperability of Systems: multiple hospitals, institutes, and healthcare organizations can join the system.
Single point records: The patient can choose to visit any healthcare facility which is on Blocktrack’s Blockchain Network without having any concerns about duplication of records or re-registrations. The consistency of the data flow is maintained without any branching issues.
This Blockchain platform developed by the team can further be used to integrate medical supply chain management and proactive tracking of the spread of contagious infections.
(L) Team members Selva and Ramashankar assisting the patients with app installation and user registration. (R) The Blockchain network running behind the application makes the entire system decentralized and secure.
Reflecting on this innovation, PI Prof. Prabhu Rajagopal said “Initiated at the height of the COVID pandemic, BlockTrack is an exciting project close to my heart, as this work showed that engineering innovations have disruptive potential to transform multiple domains. This is one of the first implementations of Blockchain technology for securing Healthcare Data management systems and we see the immense impact this approach can make in securely digitizing and maintaining unique patient records across the country and indeed across the world eventually. The system of permissions natural to Blockchain based distributed ledgers allows editability while maintaining privacy, opening up the possibility to integrate this system across primary healthcare, prescription, pharmacy, distribution and even insurance networks.We are grateful to Dr Sapna Poti at the office of Principal Scientific Adviser (PSA) to Government of India who brought the opportunity for funding this project under COVID themed support, and Infosys Limited for backing our vision. Dr Ravi Kumar of Infosys has been a gracious and supportive patron for this effort”
Prof. K. VijayRaghavan, PSA to the Government of India said “The National Digital Health Mission launched by the Government of India last year had the secure processing of individual data, and the easy accessibility of digitalized personal and medical records by individuals and health service providers, as its two important objectives. Effective implementation of these objectives will require leveraging emerging technologies. BlockTrack is a step in the right direction and I congratulate the team from IIT Madras for developing an innovative solution for a complex health information system. This will enhance and enable the efforts of health systems to efficiently track disease spread, and maintain confidentiality while storing personal data in a network.”
Teleophthalmology Adoption – Barriers and Solutions
Dr. T. Senthil MBBS DO FICO Ophthalmologist and CEO Welcare Health Systems Chennai Honorary Secretory, Telemedicine Society of India Tamil Nadu Chapter
With the COVID-19 Pandemic, as with any other modality of Telemedicine, Teleophthalmology Teleconsultations also saw a huge uptake initially- but as time progressed, the no of Teleophthalmology consults gradually came down to almost precovid levels. This article would evaluate the barriers and possible solutions for Teleophthalmology revival.
Teleophthalmology is done through the following modalities:
Teleophthalmology Consultation between Patient and an Ophthalmologist,
Image Based Teleophthalmology for Diabetic Retinopathy Detection,
Teleophthalmology for Retinopathy of Prematurity.
This article mostly covers the Teleconsultation part of Teleophthalmology.
Acceptance by Ophthalmologists and Patients
Teleophthalmology adoption by Ophthalmologists was very minimal before COVID, but once the pandemic struck and lockdown announced, Ophthalmologists started reaching out to their patients using Digital modalities, and patients also were accepting this newer modality. According to a study done by All India Ophthalmic Society only 17.5 % of Ophthalmologists were using Teleophthalmology currently, in another study 98.6 % of Ophthalmologists were willing to incorporate Teleophthalmology in their practices. There was an initial hesitation for the patients to make payment for Tele consults, but as time progressed patients started paying and this barrier was overcome.
The pandemic has hence created good acceptance level of Teleophthalmology among Patients and Doctors.
Dependence on Diagnostic Tests and Equipment’s
This is the most Important barrier to Ophthalmic Teleconsultations, since unlike psychiatry or dermatology, an Ophthalmic examination involves various tests right from testing Visual acuity, Intraocular pressure, anterior segment imaging and fundus evaluation. An Ophthalmic examination on a patient can only be done, if we get lot of information about the condition of the eyes, for which all these equipment’s are invaluable, it may not be possible to conduct these tests at patients houses, hence the number of conditions which can be treated by just doing a tele consult and seeing images of the Eye through regular computer or mobile cameras becomes grossly limited. This barrier can be addressed when there is app-based tests of visual acuity and mobile cameras getting in higher quality images etc. Till that time a model wherein patient can reach a nearby centre (Example an Optometry clinic, or Optical shop) where these equipment’s are available and tele consult done from that centre may be a viable option.
High Cost of Equipment’s and Poor Quality of Images
Other challenges
Lack of Trained Staff
Policy and Regulatory barriers
Privacy and Security concerns
With Innovations in Ophthalmic Devices and with advancements in machine learning and Artificial Intelligence, Image based Teleophthalmology will definitely see a growth in the coming years, Ophthalmic Tele consult will take its time, but as home-based devices are improved and available for a lower cost, there will be increase in Teleconsultations in Ophthalmology in the coming years.
TAKING YOUR PRACTICE ONLINE (PART 2): LEGAL COMPLIANCES AND GOOD PRACTICES
Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist
Eshika Phadke
Associate, Arogya Legal – Health Laws Specialist Law Firm
In our last article, we wrote about general considerations to be kept in mind before venturing into telemedicine. In this article, we will discuss important legal considerations to be kept in mind for operating a virtual clinic.
The Telemedicine Guidelines published last year recognize voice-video and text-based modes of consultations, so a doctor may choose to offer teleconsultation over any telemedicine apps, messaging/videocall app, SMS, email, or even set up a personal website for teleconsultations. But, while offering teleconsultations, it is important to be clear about legal dos and don’ts.
Registration of Online Clinic A common question that doctors have is whether they ought to register their work premises (or home) with any government body since they are offering medical services from the premises. In other words, does a doctor need to obtain a registration from a government department to operate a telemedicine “clinic”? The answer is NO, at least not at the moment. The existing clinical establishment or nursing home laws in various states in India regulate only those premises which receive patient footfall. By definition, virtual consultations between patient and doctor do not involve patient footfall at the premise from where the doctor is offering medical consultation. Therefore, clinical establishment or nursing home laws are presently not triggered by medical teleconsultations. Needless to say, if the venue is also used for in-clinic consultations, it would require registration under applicable clinical establishment/nursing home law.
Please note that this position may change in future if the law starts recognizing telemedicine-focused clinics as “clinical establishments”.
Website and privacy-related compliances If a doctor decides to offer teleconsultation through his or her own website, then there are certain legal requirements that must be complied with. The most important requirement would be to put in place a privacy policy. The exhaustiveness of the privacy policy would depend on the type of website that the doctor is operating. For example, if a website’s sole purpose is to enable patients to book an appointment, which is then conducted off the website (on a call, WhatsApp, Zoom, etc), a basic privacy policy specifying that the patient’s information is being collected so that the doctor can set up the appointment, would suffice. In such a case, the doctor should refrain from using a form on the website to collect information about the patient’s health condition since it would invite more stringent data privacy related compliances.
If a doctor is operating a website through which he/she can directly consult with the patient, the privacy policy would need to specify what kind of data (e.g. mental health data, physiological data, diagnostic reports, discharge summary etc.) is being collected, the purposes for which the collected data will be used and for how long will the patient’s data be stored, at the minimum.
The website should also have a term of service available as a link on the website itself, which outline the conditions under which services are being made available to the patient. An appropriate legal disclaimer should also be put on the website as applicable, such as that the telemedicine services over the website are not intended to be used in emergency situations.
Furthermore, a website or an app that offers teleconsultations would be considered as an e-commerce entity and as per the Consumer Protection (E-Commerce) Rules, 2020, an e-commerce entity must compulsorily be a company. Thus, a doctor has to incorporate a company if the doctor wishes to offer telemedicine services through the doctor’s own website to his or her patients.
Non-Solicitation The MCI (Professional Conduct, Etiquette and Ethics) Regulations, 2002 explicitly prohibits doctors from soliciting patients by “inviting attention to him or to his professional position, skill, qualification, achievements, attainments, specialties, appointments, associations, affiliations or honors and/or such character as would ordinarily result in his self-aggrandizement”. The Telemedicine Guidelines also specify that a doctor may not solicit patients for telemedicine through any advertisements or inducements. Therefore, whenever a doctor lists his or her experience and expertise on a telemedicine website or application, it should be limited to a description of the doctor’s recognized qualifications and years of experience only. The use of the expressions such as “expert”, “gold-medalist”, “best”, “leading” etc., may be held to be instances of solicitation and are best avoided.
While individual doctors (or groups of individual doctors) cannot advertise, clinical establishments can. Therefore, doctors who wish to market and advertise a telemedicine website or platform should do so through a separate legal entity such as a company or a limited liability partnership only.
When was the Term Telemedicine first used?(History and Evolution of Telemedicine – 8th Milestone)
Dr. Sunil Shroff, MS, FRCS, Dip. Urol (Lond.)
President, Tamil Nadu Telemedicine Society of India,
Editor, www.medindia.net,
Consultant Urologist & Transplant Surgeon,
Madras Medical Mission Hospital, Chennai, India (shroffmed@gmail.com).
Telemedicine was used for the first time in a publication in December 1927
Geo W. Gale’s Article “Wants Plane to Change Weather Here”
“If we have telephotography, why can’t we have telemedicine, so that you could walk up to the radio machine, drop your dollar in the slot, take down the particular receiver required and apply it to that part of your anatomy where the pain is?
The cited article was dated December 29, 1927.
When was the Term Telemedicine first used in Scientific Literature? • Telemedical technique – 1970
• Telemedicine – 1972
The term “telemedicine” appeared in the description of the telemedical project of the Arizona Medical University in an article – Arizona TeleMedicine Network: Engineering Master Plan, 1972.
Telemedicine Practice Guidelines – A Foundation Course for RMPs by TSI
New Software Identifies Patients Who may Require Ventilator Support A new software helps identify whether a patient will require ventilator support in an ICU or referral, and will make necessary arrangements before emergency sets in. At a time when sudden ICU and other emergency requirements during the pandemic have been a challenge for hospitals to manage, timely information about such situations.….. Read More
International
Omron, Kyoto University team up to study AI use for early cardiovascular disease prevention Omron Healthcare and Kyoto University are set to undertake a study under a joint research programme to use artificial intelligence and home-recorded health data in predicting early signs of cardiovascular diseases.Their upcoming study under the Healthcare Medical AI research programme will focus on two themes…..….. Read More
Ophthalmology: A pioneer in the field of artificial intelligence Ophthalmology, with its heavy reliance on imaging, is an innovator in the field of artificial intelligence (AI) in medicine.Although the opportunities for patients and health care professionals are great, hurdles to fully integrating AI remain, including economic, ethical, and data-privacy issues… Read More
Life Whisperer launches its third global IVF clinic collaboration at ESHRE to apply Artificial Intelligence to Oocytes LONDON, June 25, 2021 /PRNewswire/ — Life Whisperer, fertility arm of AI healthcare company Presagen, will invite clinics to participate in its third global IVF clinic collaboration at the 37th European Society of Human Reproduction and Embryology (ESHRE) Annual Meeting in June 2021.….. Read More
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
I am pleased to inform you about the online telemedicine course from TSI for the RMPs. This self-learning course with live interaction with the course faculty became operational this month. The course is called ‘Train to Practise Telemedicine’ and is housed on the learning management platform called MOODLE. In the near future ‘Telehealth speciality courses’ will also be developed. Please visit https://tsi.org.in/courses to view all the courses. If you wish to contribute as a TSI member you are most welcome to join us in development and delivery of these courses.
With the May Newsletter there are two additional features being introduced:
1.With this issue we are introducing visual abstracts and articles to make the newsletter more appealing and easy to read.
2.We have also introduced a new medico-legal digital health section and welcome contributions in this area. Mr. Anay Shukla from Arogaya Legal has agreed to contribute a short article for the next few issues.
Thank You. Dr. Sunil Shroff
Chief Editor
President – TN Chapter – TSI
Publication of TELEMEDCION2020 Abstracts and Select Articles in ‘Telehealth and Medicine Today’ Journal
Prof. K. Ganapathy
Guest Editor, Special issue on TELEMEDCION2020 in ‘Telehealth and Medicine Today’ Journal
Past President, Telemedicine Society of India & Neurological Society of India | Hon Distinguished Professor Tamilnadu Dr. MGR Medical University | Director Apollo Telemedicine Networking Foundation & Apollo Tele Health Services
The 16th International Annual Conference of the ‘Telemedicine Society of India’ (https://telemedicon2020.com/) was held virtually from 18th to 20th December, 2020.
The Tamil Nadu chapter of TSI under the leadership of Prof. Sunil Shroff, Organising Secretary along with four other TSI state chapters – Delhi-NCR, Rajasthan, Maharashtra and Karnataka organised this conference as a semi emergency, within 8 weeks. For the first time in two decades abstracts of papers presented have been published in a special issue of a US based journal Telehealth and Medicine Todayhttps://telehealthandmedicinetoday.com/index.php/journal/issue/view/20
This is in addition to the full text of nine papers presented at the conference (peer reviewed) besides two editorials.
John F. Kennedy in his inaugural address on 20th January 1961 remarked “ ……all this will not be finished in the first one hundred days. Nor will it be finished in the first one thousand days, not in the life of this Administration, nor even perhaps in our lifetime on this planet. But let it never be said that a beginning was not made “. I am much more optimistic. This optimism comes from the actions of my teacher Prof B. Ramamurthi. In the year 1951 four young men, driven by a passionate vision conceptualised, created and constituted India’s first ever neurological society. Dr. Jacob Chandy, Dr. B. Ramamurthi, Dr. S.T. Narasimhan and Dr. Baldev Singh brought all the disciplines associated with the science of neurology under one roof. The NSI was born. The four founding members were all office bearers !! This was audacity at its highest.
Within a year in March 1952, the society had its first meeting in Hyderabad, with 30 members from all over the country. The first presidential address was aptly titled “Neurology Comes To Life”. It was at this meeting the society decided to publish its own journal Neurology India. Today 69 years later Neurology India is a globally recognised journal with thousands of citations and 20% overseas contributions.
The world in April 2021 has turned upside down. If a journal could be started in 1952 in a then developing country in an unknown super speciality in the BC ( pun intended !) era with 30 individuals in the whole of India, I fail to see why we cannot start our own journal. Future Ready Next Generation Sequencing is now available across genetics labs in the country. It is time that the NG of Telehealth enthusiasts with access to all the resources in this planet step in and take over. Septuagenarians have shown the way.. “ Lead kindly light, lead thou me on, I do not ask to see the distant scene. One step enough for me” Saint John Henry Newman could very well have been referring to the Founding editors of TSI’s first journal.
I would like to once again place on record our thanks to the EC of the TSI to permit this exercise and also to Tory Cenaj and Prof Amar Gupta of Telehealth and Medicine Today for the unstinted support extended. HAPPY READING of the Special issuehttps://telehealthandmedicinetoday.com/index.php/journal/issue/view/20
Tele Ophthalmology Society of India – Launch Webinar on 1st May 2021
Dr. BNR Subudhi
I am happy to inform you that the Launching of Tele Ophthalmology Society of India was held on 4th April 2021 in Presence of President and Secretary of AIOS, President of Telemedicine Society of India and few international dignitaries working in the field of Teleophthalmology.
Padmashree Awardee Prof. S. Natarajan of Mumbai is the President of the Society I am the Hony Secretary, Dr. S. Pattanayak is the Treasurer and eminent Ophthalmologists of the country like Dr. R. Kim is the President elect, Dr. Rajeev Raman is the Vice President and Dr. Sheila John, Dr. Senthil, Dr. Abhesek, Dr. Ashok Nanda, Dr. Kavita Rao and Dr. Sandipak Ray are the executive members nominated to carry forward the objects of the Society which is primarily to provide Ophthalmic services to the needy rural and underprivileged people through tele consultation utilising digital technology, block chain and artificial intelligence.
As an initial step we have started collaboration with ECHO India, an organisation sharing their digital platform for Organising meeting, education, tele consultation facilities etc.
The first virtual Symposium of TOSI was organized on 1st May 2021 with Mr. Boman Irani, the Bollywood artist as the Chief Guest and other speakers from different fields of telemedicine and tele Ophthalmology like Dr. SB Gogia, Dr. K. Ganapathy of Apollo Telemedicine network, Dr. Sunil Shroff from Telemedicine Society of India, Dr. Ganesh Joshi from CRC Bhopal, Dr. Padmaja Rani from LV Prasad Eye Institute Telemedicine network and others. This gave us tremendous insight about planning ahead for the spread of Teleophthalmology systematically.
We have decided to have one monthly virtual symposium during this COVID time to interact with the members and the other stalwarts and Institutions and industry representatives to plan ahead for the members to reach the people through digital technology to prevent blindness.
The goal of Tele ophthalmology is to decrease the global burden of vision threatening diseases and improve the quality of life for patients worldwide. It will provide high quality, cost effective community eye care at the door steps of the community.
TAKING YOUR PRACTICE ONLINE (PART 1): LEGAL COMPLIANCES AND GOOD PRACTICES
Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist
Eshika Phadke
Associate, Arogya Legal – Health Laws Specialist Law Firm
During the COVID-19 pandemic, telemedicine has proven itself to be a perfectly legal, effective and safe way for doctors to connect and consult with their patients.
However, before initiating a consultation over a phone call, email or through a mobile app with a patient, it is important that doctors familiarize themselves with the legal framework within which telemedicine can be safely practiced. In this article, we have enumerated key things to be kept in mind by doctors before they take their practice online-
Medical Council Registration. While a doctor does not need to be registered in every State where his or her patients are located for practicing telemedicine, a doctor still needs to have a valid registration with the medical council of the State in which he or she resides and practices.
Familiarity with Treatment Guidelines Every doctor must familiarize himself or herself with telemedicine-specific treatment guidelines applicable to his or her specialty. If no such guideline exists for a speciality in India, a doctor may refer to international guidelines that are easily available on the internet.
Exercising Professional Judgement with Caution. No guideline can substitute a doctor’s own professional judgement to treat his or her patient. However, as a thumb rule, it may be pragmatic to err on the side of caution while offering remote consultation given the lack of physical access to the patient.
Limitations of Technology and Communication Medium. A doctor should always be conscious of the limitations of today’ technology and the medium of communication – mobile network, WiFi, internet speed, camera quality, audio, video, text, email, etc. and should offer his or her services virtually with full awareness of these limitations. It is not wrong on the part of a Doctor to request his or her patient to switch to a different teleconsultation medium or an in-person visit, if the doctor desires so in the interest his or her patient’s health.
Maintaining Patient Privacy. A doctor’s virtual clinic should be conducive to maintaining the patient’s privacy, just like his or her actual clinic. As a good practice, a doctor should also ensure that his or her patient is present in a comfortable surrounding from which the patient can have an open discussion.
Identifying Oneself to the Patient. As in physical consultation, a patient should be able to verify a doctor’s credentials and contact details in a remote consultation. If the teleconsultation is through a reliable teleconsultation App, the App will most likely display the doctor’s name, registration number, qualifications and contact information. However, if a doctor is consulting through WhatsApp, email, videoconferencing service etc., he or she should consciously display his or her registration number and name. In cases where the doctor and patient are unknown to each other, it is expected that the doctor will introduce himself or herself along with his or her qualifications to a patient, and also confirm the patient’s identity by asking the patient’s name, age, and contact information. A doctor has the legal right to request that the patient displays/shares a proof of identity with the doctor before the start of consultation, if necessary.
Maintaining Records. Before venturing into telemedicine, every doctor should establish a process to maintain and preserve records electronically. For instance, a log book for each interaction with patient should be maintained. A record of patient history, diagnosis, prognosis and prescriptions issued, if any, should also be maintained. The patient’s consent for the consultation should also be recorded, if the patient has not initiated the consultation. It is a good practice to maintain these records for a minimum period of three years.
Prescriptions. A prescription generated in course of a telemedicine consultation should not be different from a physical consultation, and should contain all information as is associated with a prescription generated during a regular consultation (for example, patient identifiers, patient history, date of consultation, provisional diagnosis, investigations recommended, medicines prescribed etc.). The prescription may be handwritten or digital, but it should be signed by the doctors, preferably by hand.
Insurance. As a safeguard against consumer complaint or legal liability, doctors who offer remote consultations should ensure that they have purchased a professional indemnity policy that either explicitly covers teleconsultations, or does not explicitly exclude it. This is not to imply that telemedicine may result in a legal issue. It’s just one less thing to worry about!
Reference: Telemedicine Practice Guidelines
NEXT TOPIC- TAKING YOUR PRACTICE ONLINE (PART 2): LEGAL ISSUES AND CHALLENGES
Space Travel and Telemedicine (History and Evolution of Telemedicine – 7th Milestone)
Dr. Sunil Shroff, MS, FRCS, Dip. Urol (Lond.)
President, Tamil Nadu Telemedicine Society of India,
Editor, www.medindia.net,
Consultant Urologist & Transplant Surgeon, Madras Medical Mission Hospital, Chennai, India (shroffmed@gmail.com).
As space travel became a reality, scientists were curious in the 1960s to find out if the human body could function adequately in outer space or not. And this brought NASA contributing to the growth of telemedicine in 1960s. They first sent animals into space who were connected to medical monitoring systems and their biometric data was transmitted back via a telemetric link.
NASA soon established an Integrated Medical and Behavioral Laboratories and Measurement Systems (IBLMS) to study changes in human physiology in outer space with zero gravity and its effects on human body.
The report described the objective of this centre as – “..It was meant to develop a system that could acquire, display, analyze and record, “…a wide variety of medical, biochemical, microbiological, and behavioral, measurements and experiments designed to study in detail man’s well being and operational capability.
NASA also launched a program, called the Space Technology Applied to Rural Papago Advanced Health Care (STARPAHC). It leveraged the remote monitoring technology that they had developed for space travel to serve terrestrial, rural populations.
The project was conducted on the Papago Indian reservation in Arizona. It evaluated the practicality and efficacy of a large-scale telemedicine operation. This truly gave a new spin to telemedicine for ‘reaching the unreached population to provide healthcare.’
Telemedicine – News from India & Abroad
India
Need to take telemedicine to villages: PM In an interaction with doctors on Monday, PM Narendra Modi drew attention to the importance of telemedicine, how it has played a big role for patients in home isolation and asserted that it needs to be expanded in rural areas as well. The PM also urged doctors to include oxygen audits in their daily routine.….. Read More
80% diseases can be nipped with primary healthcare Healthcare workers, across country, with constant training, have the potential to de-clog and reset the healthcare system. Data Driven Decisions and support for carrying out their tasks should be one of the priority.….. Read More
International
Mental health chatbots might do better when they don’t try to act human Digital mental health platforms have seen something of a renaissance during the Covid-19 pandemic, as in-person appointments have been relegated to the digital sphere. For those who cannot access therapy from a human clinician, mental health chatbot platforms are an increasingly popular digital alternative…….. Read More
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- www.medindia.net
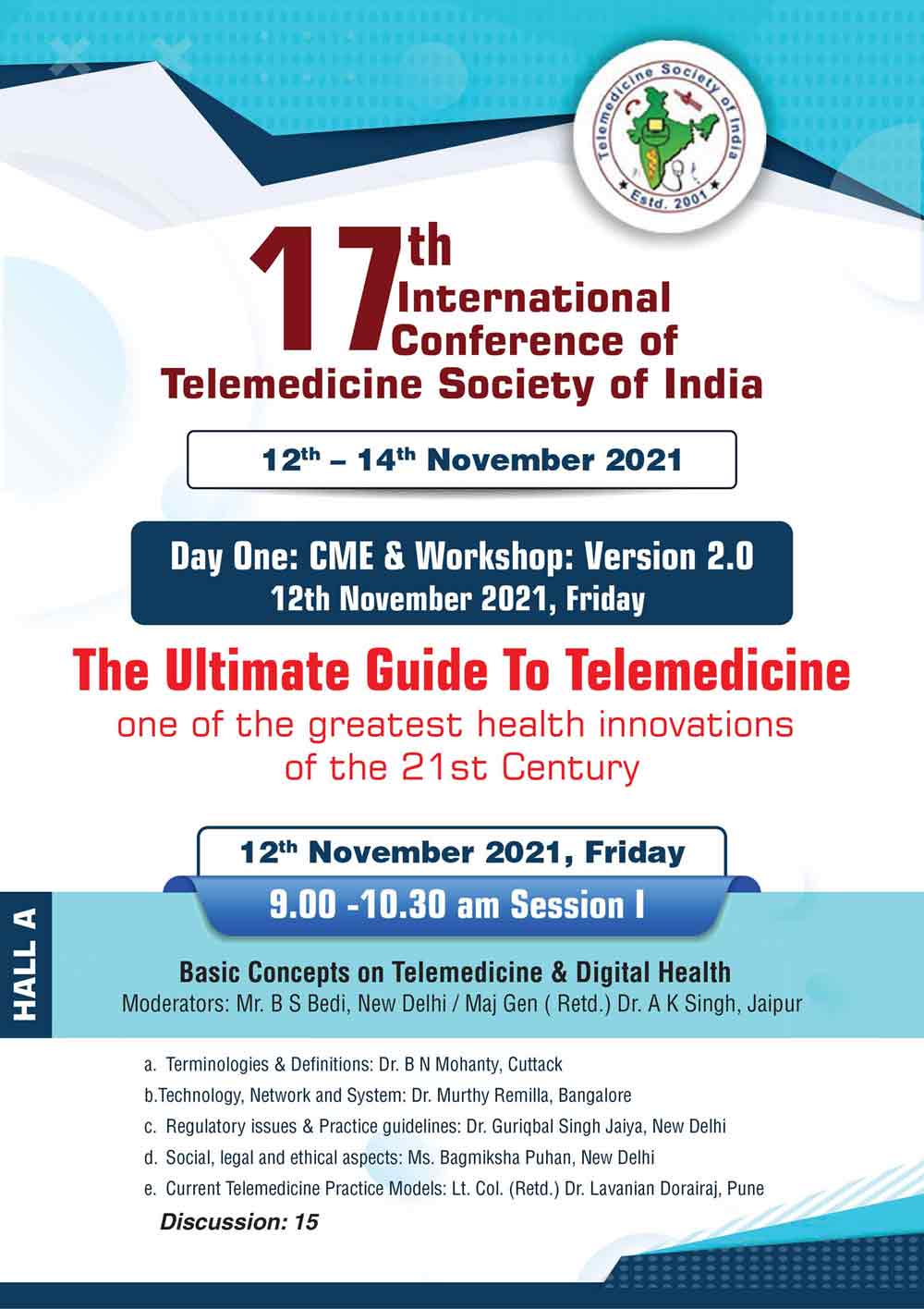



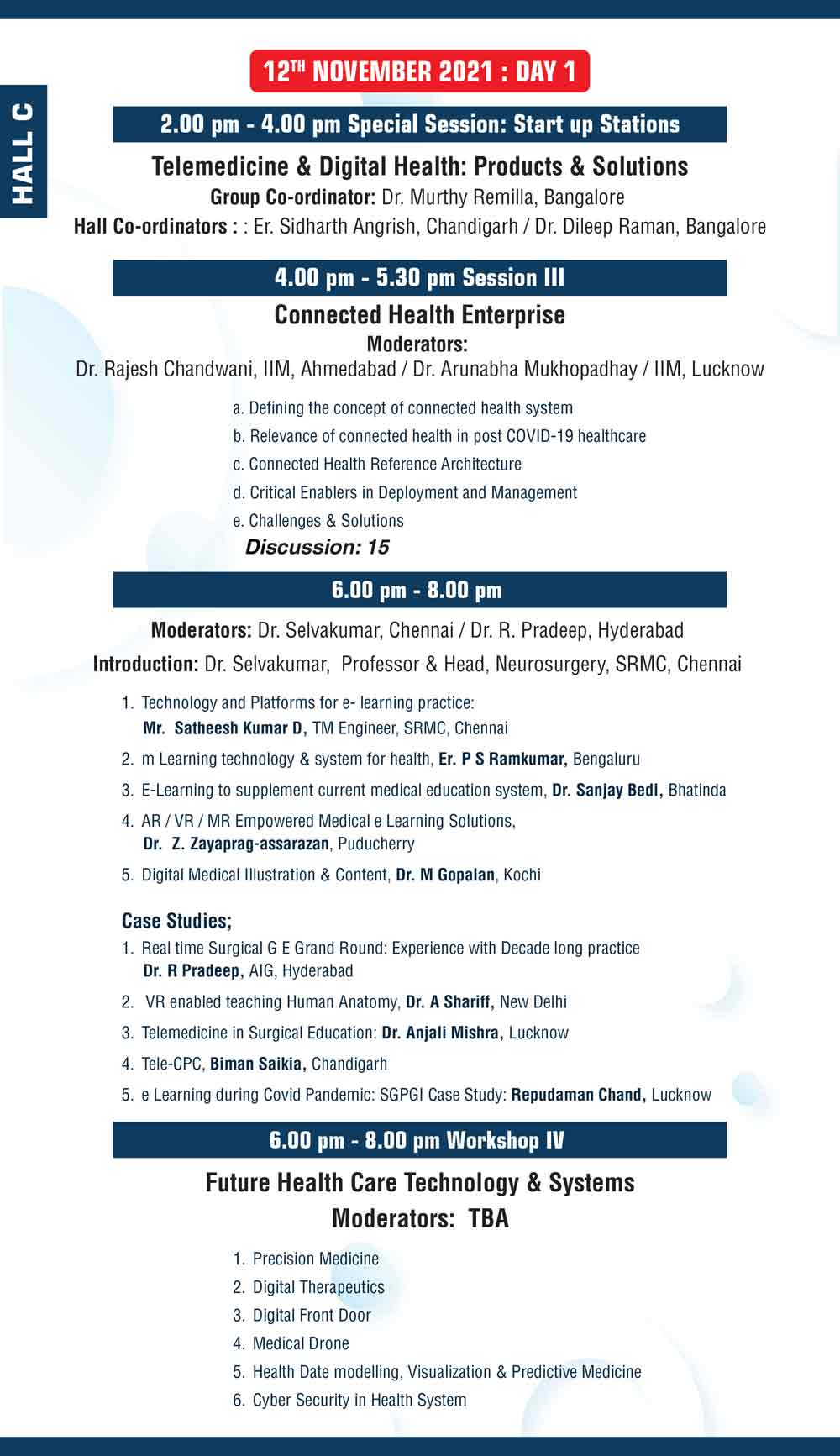
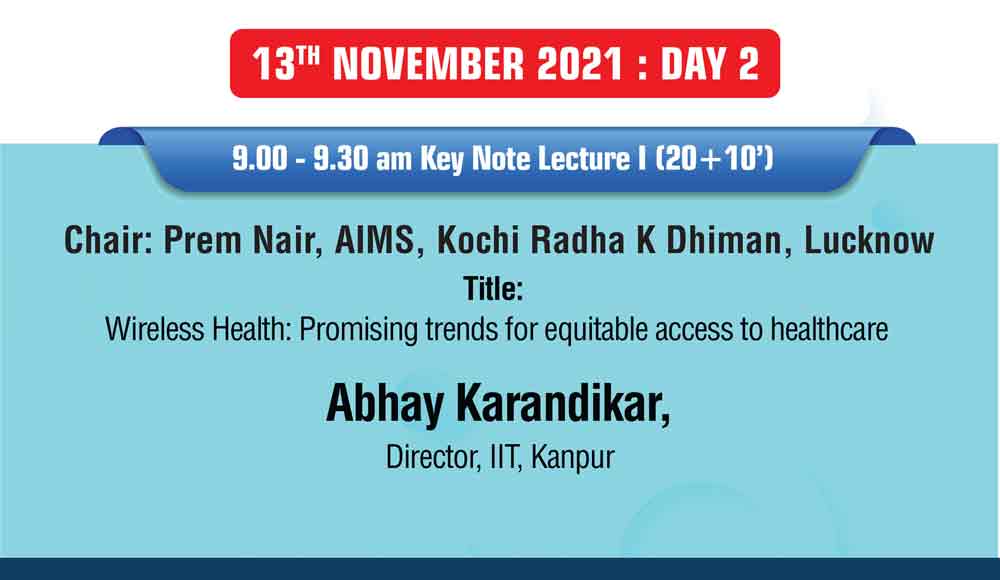














 History of Telemedicine @ Apollo Hospitals India
History of Telemedicine @ Apollo Hospitals India
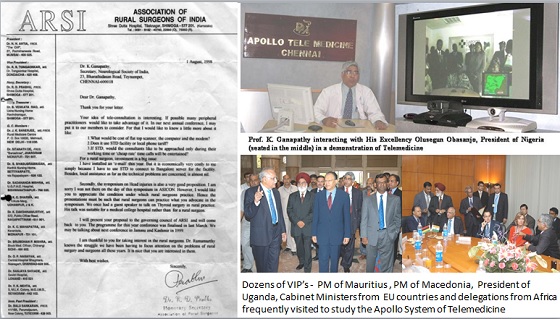
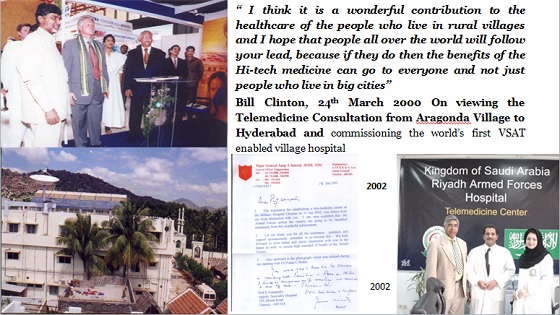
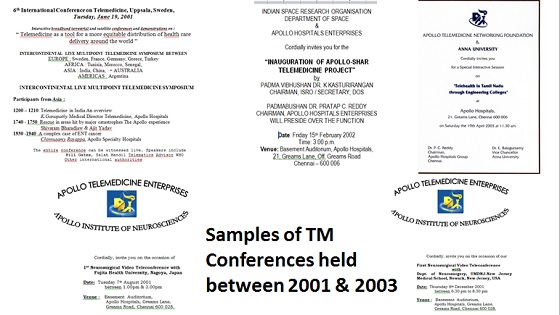


 Webinar on ‘Ethical Issues in Telehealth Practice’
Webinar on ‘Ethical Issues in Telehealth Practice’

 ISRO’s contribution for Indian Telemedicine Program from Concept to completion – Towards National Adaptation
ISRO’s contribution for Indian Telemedicine Program from Concept to completion – Towards National Adaptation


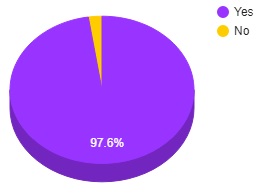
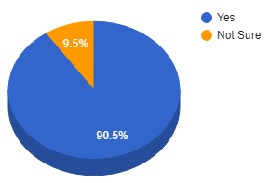
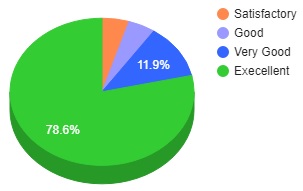









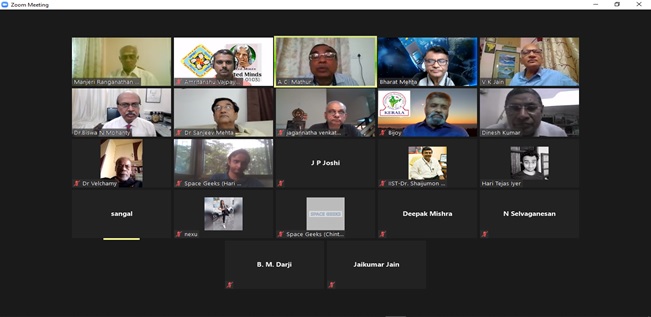
 Dr. Sunil Shroff, MS, FRCS, Dip. Urol (Lond.)
Dr. Sunil Shroff, MS, FRCS, Dip. Urol (Lond.)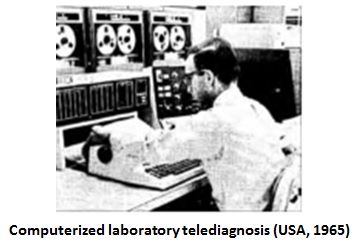


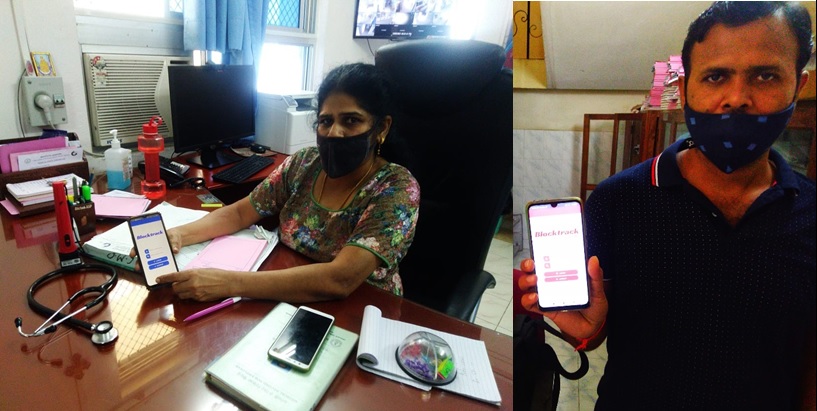
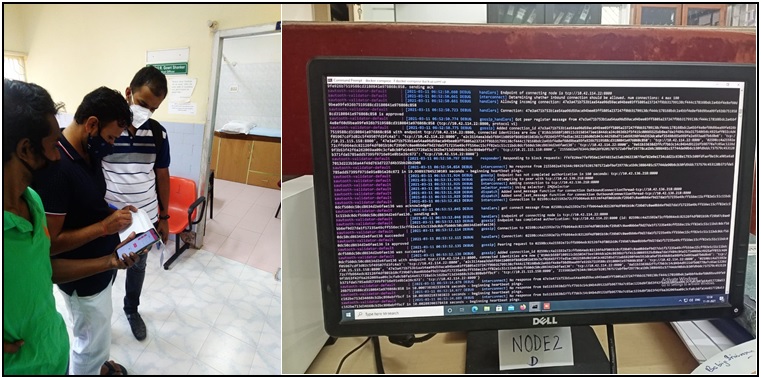



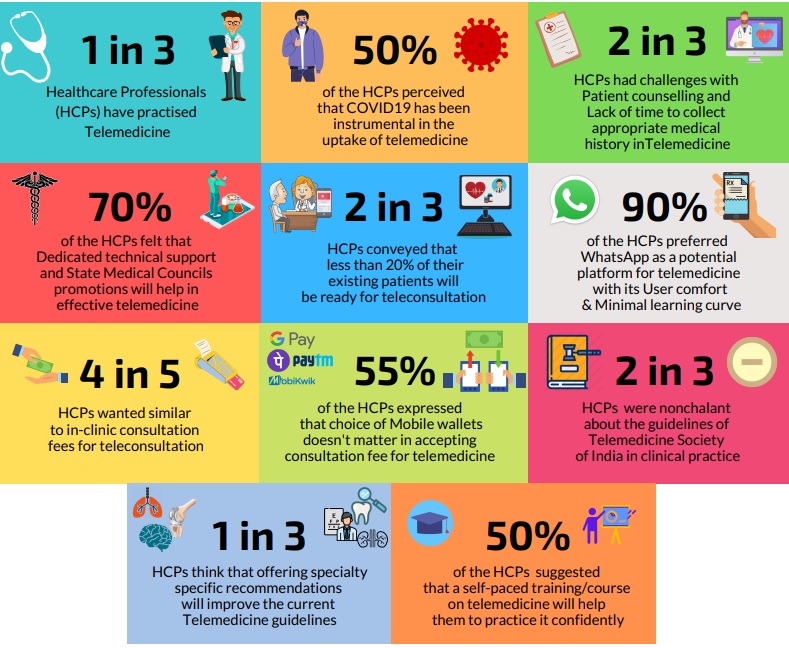
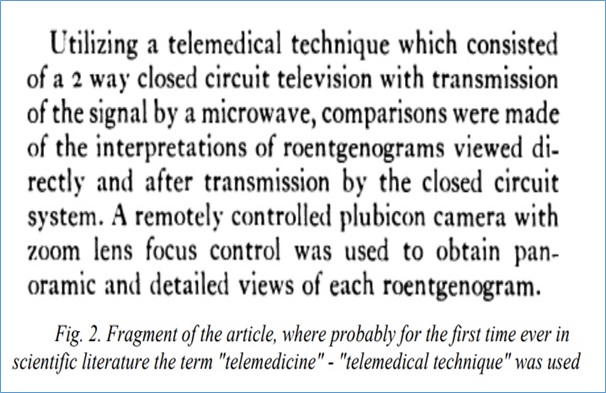

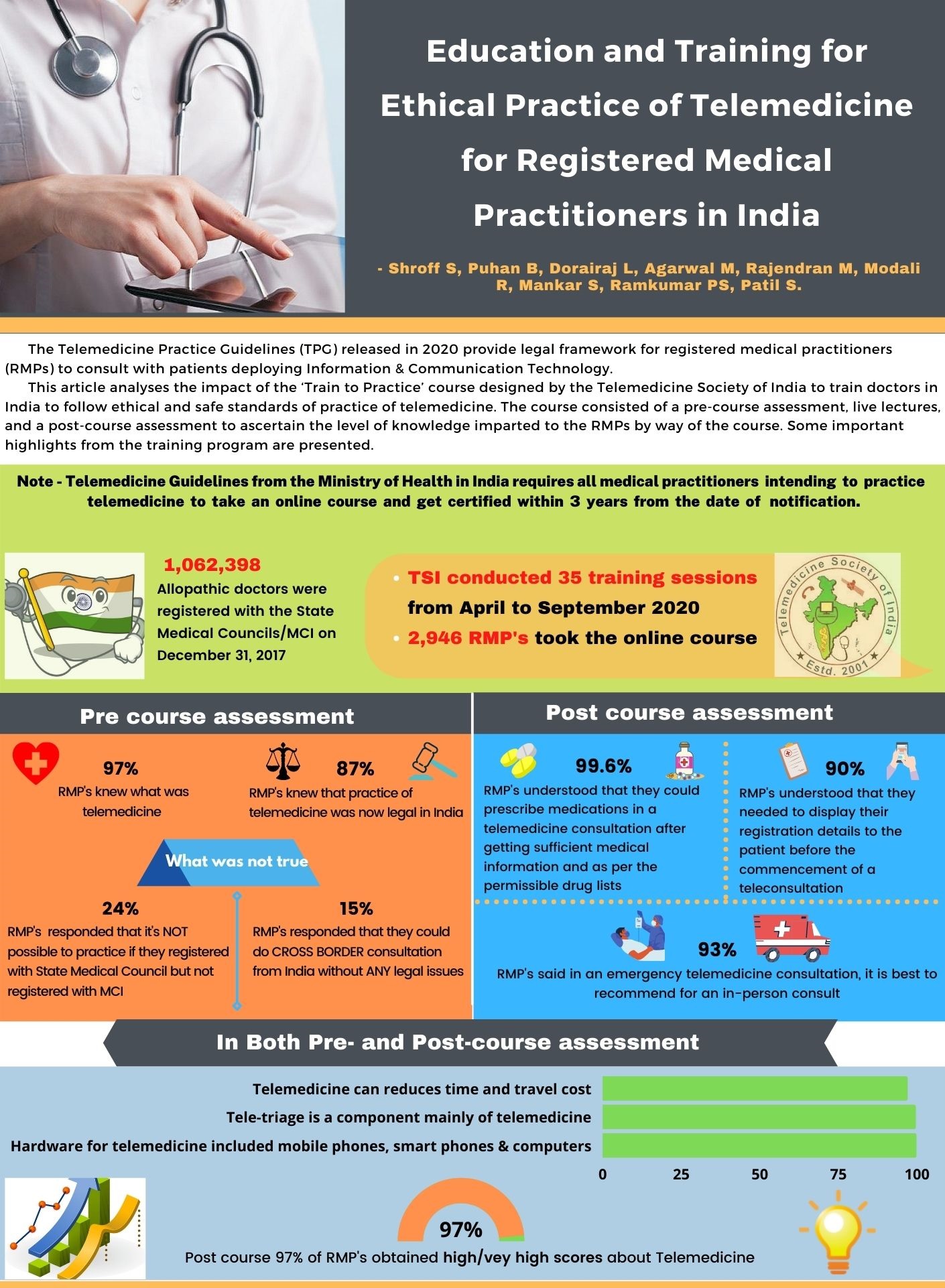

 Dr. BNR Subudhi
Dr. BNR Subudhi 
