Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
Next month comes the annual meeting at Kochi and preparations are in full swing. This will hopefully be a good face to face meeting with some online components. The program is still not out there but we are sure it will be a very engaging program.
This month we see the inauguration of Telemedicine Society of India’s J&K chapter. Wish the chapter all the very best.
October has been a quiet month for telehealth with all the other festivities. The highlight of this issue is the work of our member Indiritta Indiritta Singh Dmello with a NGO called ‘Hospital Guide Foundation’ that works for upliftment of healthcare in remote locations.
The COVID menace is not yet gone but we are learning how to live with the virus, do take your precautions when you travel for the conference.
Thank You Dr. Sunil Shroff
Chief Editor
President – TN Chapter – TSI
Hospital Guide Foundation – Working in Villages to Uplift Healthcare
Indiritta Singh Dmello
Director, Hospital Guide Foundation (An Oxford graduate in Politics, Philosophy & Economics with a PG Diploma in Medical Law & Ethics-National Law School, Bangalore)
Inspired by Gandhiji’s quote “The future of India lies in its villages” Hospital Guide Foundation (HGF) has been working towards strengthening India’s villages with a focus on rural health.
With the concentration of Doctors in the Urban areas and more than two-thirds of Indians living in villages, there is a huge shortage of Doctors in the rural areas. (A shortfall of 79.9% specialists) https://main.mohfw.gov.in/newshighlights-90
The major disease burden in India resides in Non-Communicable Diseases (NCDs) such as Heart and Lung diseases, Stroke, Cancer & Diabetes. Nearly 5.8 million people in India die due to NCDs making it a leading cause of deaths. The majority of premature NCD deaths are preventable. NCDs cause considerable loss in potentially productive years of life and hence inflicting a burden on the socio-economic development of India (Ref –https://www.wbhealth.gov.in/NCD/)
Hospital Guide Foundation (HGF) ensures comprehensive Quality Healthcare is accessible in the rural areas with a focus on Non-Communicable Diseases free of cost. It works with an effort to have a sustainable impact supported by Corporate Social Responsibility and is currently working in Western Uttar Pradesh, impacting masses of people annually and hoping to hit a million by 2025, by expanding to the entire state and then the entire country.
For effective last mile connectivity, HGF works with the Pradhans of the villages with a two-pronged strategy of spreading awareness followed by action. It uses Telemedicine as an enabler to address the gap where there is a lack of sufficient Doctors in the rural areas. To have a sustainable and successful Telemedicine program, HGF deploys a holistic approach with seamless processes and optimal technology hence achieving better results. It ensures tests, medicines, counseling is given (about the process, disease & treatment), right expectations are set, ensures compliance (tests, medicines & life style) and pro-active follow ups. Multiple touch points are managed seamlessly between patients, nurses, Doctors and telemedicine specialists for enabling a great healthcare experience against a harsh backdrop of poor infrastructure be it roads, electricity or internet. Hence optimal technology is deployed for a superior Doctor-Patient experience as the quality of communication has a direct impact on the diagnosis, prognosis and treatment.
Regular Health camps are conducted to drive awareness and reach the masses. Post the health camps, patients are linked to HGF’s telemedicine program to ensure continuum of care.
HGF’s focus on quality processes and alliances with the best institutes such as AIIMS, National Heart Institute, Sita Ram Bhartia Institute of Research & Sciences, Dr Dang’s Path lab has ensured that the best care is provided.
Being the most stringent form of an NGO (licensed by the Govt of India, Company U/S 8 for charitable purposes) only reinforces the core values it stands for – Ethics, Competence and Compassion. It has been featured by many prominent media houses like Economic Times, India Today, Hindu and internationally covered by BMJ Innovations (British Medical Journal). The Advisory Board comprises of stalwarts like Dr. M.C. Misra, Ex Director with AIIMS (appointed on HGF’s Advisory Board on approval of the Union Health Ministry while he was the Director) handholding HGF through all its processes to ensure quality delivery. The Director of HGF, Indiritta is an Oxford Graduate with a PG Diploma in Medical Law & Ethics from the National Law School, Bangalore, who works relentlessly towards achieving HGF’s dream of a Stronger Healthier Rural India.
A case study of HGF’s work featured in a top Medical Journal and a success letter from the Government of Uttar Pradesh is a testament to the quality of work being done on the ground. However, the truest and most rewarding testament is from the patients itself!
Curtain raiser Webinar for TELEMEDICON 2022
“Strengthening Health Systems through Sustainable Telemedicine and Digital Health”
in Association with Telemedicine Society of India Kerala Chapter, Amrita Hospitals & Journo Med
26 October, Wednesday, 8:30 PM
A curtain raiser webinar for TELEMEDICON 2022 was conducted at Amrita Hospitals with Telemedicine Society of India Kerala Chapter, on 26 October.
The theme was “Strengthening Health Systems through Sustainable Telemedicine and Digital Health”
With the significant increase in technological usage at all levels, Telemedicine and Medical Informatics are expected to grow at a considerable pace in the upcoming years, which enhances the growth of the MedTech space. . The significance of Telemedicon 2022 is to discuss the future of Telemedicine which holds immense potential in the healthcare sector. The pandemic catalyzed the pace and the growth dimension in the field of Telemedicine and digital health.
Topics Discussed
How Remote Patient Monitoring is Changing the Healthcare Services
How to Implement Telemedicine in Daily Practice
Expert Speakers
Dr. Rajesh Pai, Chief Operating Officer, BMH Gimcare Hospital, Kannur
Dr. Uma Shankar, Principal, Padmashree School of Public Health Bangalore, Managing Director – Med.Bot
Telemedicine Society of India (TSI) Maharashtra Chapter Organizes Annual Conference Mahatelemedicon 2022
The Maharashtra Chapter of TSI recently Organized Mahatelemedicon 2022-on 17 Sep 2022 in association with DY Patil Medical College and Research Centre (DYPMCH-Pimpri).
The conference was well attended and had unique highlights.
Two credit points were awarded to participants by Maharashtra Medical Council.
There was a poster and an essay competition on the theme My Idea of Telemedicine
A Product Theatre on connected care devices was presented by Dr SV Kulkarni.
The conference was inaugurated by Dr Yashraj Patil Trustee and Treasurer DYPMCH-Pimpri Plenary Oration was by Dr Ganapathy on the topic- DIGITAL HEALTH IN 2030 : A PEEP INTO THE FUTURE.
Keynote addresses were given by Vimal Wakhlu and Dr Gaur Sundar. They spoke on AI in health care and Ayushman Bharat Digital Mission respectively.
Dr Bagmishika Puhan gave an excellent presentation on medicolegal aspects of telemedicine.
Dr Suchitra Mankar -current President of TSI-MH conducted a quiz on Telemedicine Guidelines in which there was very good audience participation.
The entire chapter worked and contributed to the success of the conference.
Notably, Constant guidance and mentorship was provided by Dr BS Ratta.
Dr JS Bhawalkar (Dean DYPMCH) provided immense support in venue and infrastructure.
Dr SV Kulkarni-President elect and Dr Prachee Sathe provided excellent liaison and sponsorship.
Dr Suchitra Mankar (President) and Dr Prashant Kulkarni (Organizing Secretary) planned and executed the entire conference efficiently and effectively.
TSI MH has been very active and dynamic in 2022. Besides Mahatelemedicon, an annual conference by a State Chapter, they have hosted many events like Telemedicine Quiz for all doctors of Pimpri Chinchwad and for Indian association of Occupational Health; Teleophthalmology Conference; Tele physiotherapy conference to name a few.
Lamp Lighting Ceremony
Dr Ratta felicitation the poster winner
The Chairpersons, The Org Secretary and the MC-Dr Sayali Shinde enjoying the moment
AI assisted model to predict bone repair outcomes for various fracture-treatment methods
AI-based simulation model can potentially help a surgeon choose the right implant or technique before a fracture-treatment surgery.
Developed at Indian Institute of Technology Guwahati.
Researchers have developed Artificial Intelligence (AI) model to predict the healing of thigh bone fractures after surgery. The model developed by Dr. Souptick Chanda, Assistant Professor, Department of Biosciences and Bioengineering, IIT Guwahati, and his team can be used to assess the healing outcomes of different fracture fixation strategies so that an optimum strategy can be chosen for the patient depending on their personal physiologies and fracture type. Using such precision models can reduce the healing time, lighten the economic burden and pain for patients who need thigh fracture treatment.
The results of this research have recently been published in the open-source journal, PLoS One, in a paper co-authored by Dr. Souptick Chanda and his research scholar, Mr. Pratik Nag.
Speaking about the research, Dr. Souptick Chanda, Assistant Professor, Department of Biosciences and Bioengineering, IIT Guwahati, said, “AI has tremendous potential when it comes to understanding and predicting complex biological phenomena and hence, can play a big role in health sciences applications.”
The research team have used a combination of Finite Element Analysis and the AI tool, Fuzzy Logic to understand the healing process of fracture after various treatment methods. Various bone-growth parameters were used along with a rule-based simulation scheme for this purpose. The study further examined the influence of different screw fixation mechanisms to compare the fracture healing efficacies of each process. The predictions of healing made by the model agreed well with experimental observations, pointing to its reliability.
IIT Guwahati’s AI-based simulation model can potentially help a surgeon choose the right implant or technique before a fracture-treatment surgery. In addition to various biological and patient-specific parameters, the model can also account for different clinical phenomena, such as smoking, diabetes, etc. The model can also be adapted for veterinary fractures which are, physiologically and in various aspects, similar to those occurring in human patients.
The researchers plan to develop a software/app based on the algorithm that can be used in hospitals and other healthcare institutions as part of their fracture treatment protocols. The team is presently collaborating with Dr. Bhaskar Borgohain and his team of orthopaedists from the North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences Hospital, Shillong, for animal studies to validate and fine-tune certain parameters.
Research done by IIT Guwahati researchers is useful because the incidences of thigh-bone and hip fractures have increased significantly due to the increasing geriatric population in the world. An estimated 2 lakh hip fractures occur every year in India alone, most of which require hospitalisation and trauma care. Treatment for hip fractures traditionally includes bone plates and rods to bridge the fracture site and promote bone healing. Fracture treatment methods are intuitively chosen by surgeons based on their experience, and there is no way of predicting the efficacy and success of the treatment method chosen. The research from IIT Guwahati will help increase the accuracy rate in decision-making in orthopaedics, thereby reducing the cost and disease burden associated with fracture recovery.
IIT Guwahati is working progressively in the field of medical technology and related fields. With the recent installation of Supercomputer facility PARAM KAMRUPA at the Institute, Artificial Intelligence, Data Science, and Deep Learning, among others, and their applications in the inter-disciplinary areas of health sciences, weather prediction and nanotechnology have got a major boost.
Telemedicine – News from India & Abroad
LifeHub+ App Links Patients, Doctors With Fitbit?
LifeHub+ app launched by telecom company StarHub links patients to their doctors with Fitbit data for better healthcare management.The LifeHub+ app provides two different ‘ConnectedCare’ plans to the patients– $9.99 monthly plan and $99.99 annual plan…Readmore
Are Smartwatch Health Apps Smart Enough?
Philadelphia, October 12, 2022 – Extended cardiac monitoring in patients and the use of implantable cardiovascular electronic devices can increase detection of atrial fibrillation (AF), but the devices have limitations including short battery life and lack of immediate feedback. Can new smartphone to…Readmore
Artificial Intelligence Helps Find Similar Cases, Diagnose Rare Diseases
A deep learning algorithm known as SISH (Self-Supervised Image search for Histology) teaches itself to learn features which can then be used to find similar cases in large pathology image repositories.The new machine learning tool acts like a search engine for pathology images and has many potential ….Readmore
Facemask can Detect Viral Exposure Within 10 Minutes?
Scientists have created a face mask that can detect common respiratory viruses, including influenza and the coronavirus, in the air in droplets or aerosols. The highly sensitive mask, presented September 19 in the journal Matter, can alert the wearers via their mobile devices within 10 minutes if …Readmore
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
The Personal Data Privacy act has been long overdue in India. It was introduced in the parliament in December 2021, to regulate personal and non-personal data jointly but was withdrawn in August 2022. The government has now put out the draft of the telecommunication bill that was put out recently for public comments (https://dot.gov.in/relatedlinks/indian-telecommunication-bill-2022). Comments may be sent on the email ID : naveen.kumar71@gov.in Last date of sending the comments will be 20th October 2022. This bill will influence the provisions in the data privacy act too.
The existing regulatory framework for the telecommunication sector is based on the Indian Telegraph Act, 1885. With advent of new technologies such as 4G and 5G, Internet of Things, Industry 4.0, M2M Communications, Mobile Edge Computing, AI and many more, the technologies are creating newer opportunities for India’s socio-economic growth. Therefore, India needs a legal framework attuned to the realities of the 21st century.
The draft bill covers conventional phone calls, text messages broadband connections and over-the-top applications, including WhatsApp defined as telecommunication services.
The worrying aspect is that the bill seeks the regulatory powers to control and management of, or suspending the operation of services without putting a review mechanism in place. The explanatory note to the bill says – “The Bill provides an enabling framework for the Central Government to address any situations of public emergency, public safety, or national security concerns. These provisions provide for the time-bound limited suspension of transmission of messages, or of provision of telecommunication networks or services while ensuring the rights of the citizens of India,”
The Supreme Court in January 2020 had said that such shutdowns should be temporary and periodically reviewed. No review mechanism has been mentioned in the draft bill and this will invite criticism. Such provisions will have a bearing on the Data Privacy Act too. The Sept Newsletter covers an updated information on Data Privacy Act from Ms. Bagmissikha Puhan.
It is now just another 6 weeks to the national conference of TELEMIDICON2022 at Kochi. Do register in large numbers to make this national event a success.
Wish all our members a Happy festivities during Navaratri.
Thank You Dr. Sunil Shroff
Chief Editor
President – TN Chapter – TSI
Digital India Act and Pending Legislations
Bagmisikha Puhan Associate Partner, TMT Law Practice
Siddhant Gupta Associate, TMT Law Practice
The Data Protection Bill, 2021, introduced in December 2021, to regulate personal and non-personal data jointly, was withdrawn in August 2022, in view of the increased regulatory compliance upon start-ups, and persistent opposition from stakeholders on provisions of data localization, data transfer, and LEA access to such datasets [including anonymized data]. The absence of a comprehensive data privacy legislation compels stakeholders to rely upon sectoral guidelines, which while enforceable, may become more onerous, for want of a common thread across all sectors. It is expected that the Information Technology Act, will also undergo a complete overhaul, pending legislation with respect to data privacy . The intention of legislature is to create a future-proof, comprehensive regulatory landscape for the regulation of digital activities, the government has proposed to issue a set of legislations, to usher a comprehensive framework for information technology law and regulation.
The legislators propose to introduce the Digital India Act (DIA), to address the convergence in technologies, services, and devices in the digital ecosystem. The DIA is expected to govern aspects of regulation of intermediaries, over-the-top (OTT) platforms, and provide for guidelines around women and child safety on the internet. While the DIA is expected to be tabled in the winter session of the Parliament, the privacy legislation may be introduced only during the budget session.
Presently, the regulation of over-the-top platforms is not contemplated under any enforceable statute; DIA is likely to provide for a definitive classification for OTT services, and provide guidelines for developing appropriate self-regulatory methods, providing guidelines around classification of content, age verification mechanisms and other issues.
DIA is further expected to account for new age technologies, such as artificial intelligence, internet of things, blockchain, and address regulatory concerns. Keeping in mind the business friendly outlook of the regulators towards digital space, it is expected that there would be an evaluative criteria to determine the level of compliance for entities. With the existing telemedicine practice guidelines referencing the usage of AI, ML, and big data to the advantage of the platforms, as well as the practitioners, a little more clarity will drive the functionality of platforms in the digital health sector, better. Interestingly, the telecom regulator is also considering revisions around use of this technology in the telecom sector, which will be also something that the digital health world will rely upon.
It is expected that DIA will harmonize the legislations, regulations, amendments released within the last couple of years, with respect to social media platforms, digital services, and blockchain related business undertakings. Towards such end, the government had released a draft Non-Personal Data Governance Framework in 2021, for consultation, to enable controlled access to non-personal data for “sovereign, public good purposes”.
It is expected that the DIA shall provision for such controlled access to NPD, per the granularity criteria of DIA, to provide access to such aggregated data sets to public, private entities, for their intended use. It is pertinent to note that IRCTC had sought to capitalize on the passenger sets available and had introduced a tender for hiring consultants in order to formulate a passenger data monetization plan. For example, businesses may have access to estimated footfalls in a particular location based on ticketing volumes bound for the location through IRCTC’s monetized data. The scope of work was to be limited to sharing aggregated data and anonymous data for sharing with private and government companies; however, in absence of a dedicated central data privacy legislation, the tender has been temporarily put under review.
TSI Mid-Term Conference – Proceeding and Recommendation Thereof
Mr. Farooq Ahmad Wani M. Tech. Superintending Engineer, Electronics & Communication / Information Technology (E&C/IT),
Sher-i-Kashmir Institute of Medical Sciences (SKIMS), Soura, Srinagar | State Nodal Officer (Telemedicine), Jammu & Kashmir
Department of Electronic Communication & IT at Sher-i-Kashmir Institute of Medical Sciences or SKIMS conducted the first TSI Mid-Term Conference 2022 in Jammu and Kashmir under the Aegis of Telemedicine Society of India on 25TH – 26TH AUGUST, 2022.
The Chief Guest of the Conference was Shri Rajeev Rai Bhatnagar, Advisor to Hon’ble Lieutenant Governor J&K and the Guest of Honour was Shri Bhupinder Kumar (IAS) Administrative Secretary, H& M E Department, J&K. The event was attended by faculty SKIMS, faculty from other Institutions, Administrative staff and students along with the national TSI executive members.
This event in Srinagar holds special significance as it is the first of a kind conference in this UT and this could give great impetus to the ongoing rolling out of ABDM in the UT.
As far as Telemedicine in J&K is considered, the Government of Jammu and Kashmir and The Indian Space Research Organisation (ISRO), both have contributed immensely to creating this facility at SKIMS along with 12 other Medical Colleges/District & Sub District Hospitals with SKIMS Telemedicine Centre as its hub.
Theme The theme of the event had been carefully chosen – “Telemedicine in Special Conditions & Special Geographies” as we expected that the conference became a platform for discussing the role of Information Communication Technologies (ICT) in bridging the gap between the patient and the doctor in the terrains like J&K.
The theme was apt for the UT as it is a disaster-prone area and has the occurrence of earthquakes and floods, and turmoil prone. It also has extreme winter, making many of its parts inaccessible during winter periods. This is particularly true for Ladakh, Gurez, and Zanskar areas and some parts of the Jammu region which include Padar and Wud Vun, that remain cut off for more than six months in a year.
Telemedicine has the potential to play a bridging role in overcoming these challenges. Telemedicine also finds its use in places where large populations occasionally/periodically gather at a point in time, where the provision of medical care becomes the need of the hour; for example, the Government of J&K practices telemedicine during the Amarnath Yatra.
The Chief Guest along with the guest of honour inaugurated the two-day mid-term conference in presence of various other dignitaries.
Key Messages from the Dignitaries
Shri Rajiv Rai Bhatnagar who was the chief guest on the occasion in his address complimented SKIMS for pioneering services in Telemedicine. He said there needs to be more focus on telemedicine services in UT J&K attributing vast expansion in the medical area. He also said that critical services need to be accessible in remote places and access to masses to various services in telemedicine needs to be prioritized. He hoped that today’s event will provide us with better inputs and ideas to further improve upon the better patient care services.
Mr. Bhupinder, IAS, Secretary Health and Medical Education Govt. of J&K who was the guest of honour on the occasion said UT J&K has many inaccessible areas and has made a lot of strides to adopt digital services and the general public has been provided satisfactory services like comprehensive call centres, mobile ambulances in remote areas. He further said IT solutions including hospital management system are revolutionizing the functioning of hospitals. He underlined that user-friendly technology can be significant in the use of telemedicine services and emphasized training/capacity building of practitioners and said a lot more needs to be done to popularize telemedicine services to benefit the common man. He also highlighted various services being provided under the Ayushman Bharat Initiative in UT J&K including Ayushman Bharat Pradhan Mantri Jan Arogya Yojana. He said times like COVID made the adoption of technology much easier and brought greater work efficiency and the use of various applications generating sufficient data helps strategize policies for the future to come.
Director SKIMS Prof. Parvaiz A. Koul complemented the organizing team and thanked the Telemedicine Society of India for choosing SKIMS for the event and said that SKIMS is the only public hospital with a well-established Telemedicine Centre and said the department of Electronics and Communication/IT needs to be commended for their excellent work. He further said SKIMS recently digitized important service areas including patient registration, payment system, and report access which has been well received by the public and has facilitated patient care services here at SKIMS.
Prof. Tariq Gojwari, Dean Medical Faculty and organizing chairman, while speaking on the occasion gave a detailed account of Telemedicine services at SKIMS and said SKIMS is the only tertiary care centre with well networked digital platform which has so far benefitted the huge number of patients.
Prof. Prasanta Kumar Pradhan, President of the Telemedicine Society of India who joined online while addressing the audience said that it is the first mid-term conference organized by the Telemedicine Society of India in J&K. He emphasized the use of digital technology in health services. India has adopted digital technology which has been a game changer and has brought greater accountability and accessibility to health care services, he added.
Dr Murthy Remilla LN, Hon. Secretary TSI, welcomed the dignitaries and the guests. At the outset he, complemented the Director SKIMS for allowing the conference at such short notice. He urged, not to see the quantity but quality of the conference which is at par with any national level conference, that too at such short notice. He further said that this meeting is the only such conference outside the headquarters of TSI, and will act as a precursor to the Annual Conference of TSI at J&K in future. He congratulated the team and appreciated the efforts of organizers, dignitaries, guests and SKIMS administration. Regarding Telemedicine at J&K, he emphasized the need for champions for utilizing the Telemedicine system and leaders making the people make use of the system by the convergence of technology for the implementation of Telemedicine and take forward this technology state-wide. He concluded by advising the audience to leave with good memories and utilize Telemedicine to provide good services to patients.
Er. Farooq Ahmed Wani, organizing secretary of the event welcomed the guests and thanked Rajiv Rai Bhatnagar and other dignitaries for attending the event. He gave a detailed account of the activities of the Telemedicine Society of India vis a vis Telemedicine services at SKIMS. He said Telemedicine Centre at SKIMS is an essential link in providing the best health care services state-wide and has served as the nerve centre of the JK Telemedicine network, particularly in various disaster situations like the 2005 Earthquake, 2014 Floods and the 2019 Covid 19 Pandemic. He thanked Director SKIMS for supporting and facilitating the event.
Mr Vimal Vakhloo former president of TSI also spoke on the occasion and Er. Parvaiz A Bhat co-organizing chairman and Chief Engineer SKIMS were also present at the event.
PROGRAMME The event had a total of 10 sessions of one hour each, spanned over 2 days (5 each day) where each session had 3 slots for presentation or panel discussion. Day first had the first 2 sessions merged and the inauguration session in the afternoon and the day second had a valedictory function at the end. The following is the list of topics for each session.
Besides the usual scientific programme the event focussed on newer emerging digital technologies which are influencing telehealth, strategy besides showcasing the ABDM initiatives.
In the last two decades, the domain has progressed a lot and is still expanding like Artificial Intelligence, Machine learning, imaging informatics, 5G network, cloud, blockchain etc. having potential in healthcare and professional education.
OUTPUT As evident from the discourse of this conference, the future holds enormous opportunities in the usage of these technologies which are becoming simpler and less expensive day by day and many of them are patient-centric applications in home settings.
The COVID-19 pandemic demonstrated the potential telemedicine offers in augmenting health systems capacity in the UT. During the pandemic, there were operational challenges at multiple levels and there was an urgent need to find the right solutions for contactless healthcare delivery where SKIMS has efficiently used its telemedicine resources to the full extent by using Telemedicine and virtual meetings as the crucial link between all the stakeholders in tackling the pandemic.
Following the outbreak of COVID-19, India’s government has launched new telemedicine guidelines to help healthcare professionals and the ICT industry provide medical services to the population during the lockdown. Even as the health systems transformation envisaged through establishing primary care networks and health and wellness centres under Ayushman Bharat are being established, the Telemedicine Guidelines 2020 provide the opportunity to leapfrog and invert the healthcare delivery paradigm.
Large-scale telemedicine practice in UT would also facilitate the adoption of electronic health records and thereby realize the grand vision for the digital health backbone as envisaged in the National Digital Health Blueprint and strategies outlined by Niti Aayog in Health Systems for a New India: Building Blocks—Potential Pathways to Reforms.
In Summary As with all technological innovations, telemedicine will be as best at the hands of human experts who leverage it to their advantage. It would be paramount that the health professionals at SKIMS leverage telemedicine to their competitive advantage.
In the long term, empowering citizens, and enhancing user experience in healthcare delivery are likely to improve health-seeking behaviour.
It is high time that digitalisation, cloud solutions, and analytics technologies are leveraged in the healthcare setting, especially at SKIMS. Digitally connected processes enable paperless operations. It is high time for a perception change of viewing IT as an enabler of healthcare delivery.
Further, the process of health planning needs to evolve through the use of Telemedicine in healthcare delivery and distribution and public health decision-making at every level.
AI for Radiology Being Used in Russia
Ms. Filippova Anna
Diagnostics and Telemedicine Center, Moscow Health Department.
Smart algorithms aids doctors in 15 research areas. Now neural networks determine the signs of arthrosis in the knee joint on x-rays and emphysema on computed tomography. This was announced by Ilya Tyrov, Deputy Head of the Moscow Health Department.
“Thus, smart algorithms help doctors in 15 research areas. In total, it already has processed more than 7 million x-rays studies. Further, we intend to expand the application of AI to 29 different areas.” he said.
AI simplifies and speeds up the work of a doctor. It detects and reports even minor deviations and report about it. The doctor receives a picture already marked by the algorithm and describes it independently.
“The radiologist may disagree with artificial intelligence and make a decision himself. The use of such services is not intended to be a substitute for the work of a specialist. You can draw an analogy between modern dictionaries and old ones. You had to open the dictionary and spend a lot of time looking for the right words, now you just need to click on the right link,” said Yuri Vasilyev, Chief Freelance Advisor for Radiation and Instrumental Diagnostics of the Moscow Healthcare Department, CEO of the Center for Diagnostics and Telemedicine.
Nowadays, thanks to smart assistants, it has become less demanding for radiologists to find signs of lung cancer, COVID-19, spinal osteoporosis, thoracic aortic aneurysm, coronary heart disease, stroke, pulmonary hypertension, hydrothorax, as well as lung pathologies, breast cancer and flat feet on CT scans. Neural networks have been introduced into the work of Moscow institutions, which recognize symptoms of 7 different pathologies in one medical image of an X-ray examination at once.
An experiment on the introduction of computer vision into medicine was launched jointly by the Moscow Social Development Complex and the Department of Information Technologies on the basis of the Center for Diagnostics and Telemedicine. Since the start of the Experiment, AI services have processed over 7 million studies. The Center has become a platform for the development of artificial intelligence technologies in Russia, as well as support for domestic developers.
Briefly on the Diagnostics and Telemedicine Center: Diagnostics and Telemedicine Center was established in 1996. It is a top scientific and telemedicine organization under the Moscow Health Department. It specializes in AI implementation in medicine, researches radiation diagnostics, manages departments in medical organizations, including the telemedicine approach.
TELE ICU – Challenges and Solutions
Dr. Raj Raval President of Telemedicine Of India – Gujarat Chapter
The Indian healthcare industry is under severe pressure owing to a large population and a massive shortage of skilled healthcare professionals including doctors, nurses and intensivist.
There is a shortage of intensivist in India, and the demand for them is only going to increase with the aging population.
India will have 5,00,000 ICU beds by 2023, but only 8,350 critical care specialists / Intensivist to monitor it
Need 50,000 Critical Care Specialists but has just 8,350, As per, the Indian Medical Association source.
Having timely access to critical care doctors, medical facilities and treatment centers is limited to only a small portion living in developed metro cities leaving a large part of the population living in rural areas without access to quality healthcare.
Lack of protocols driven ICU.
High Mortality Rate in ICUs.
Lack of real time interventions to treat patients.
How Tele-ICU Works TeleICU is an advanced intensive care solution powered by revolutionary technologies that aim to offer round-the-clock critical care even in the remotest corners of the country.
TeleICU solutions allow hospitals to become robust in early interventions for critical care patients even when they lack professional resources like critical care specialists on-site. Through a multi-pronged, technology-driven approach, Entel Healthtech looks forward to providing best-in-class intensive care facilities to patients requiring advanced level care.
• Entel Healthtech is a technology-driven organization which aims at revolutionizing the existing healthcare infrastructure in the country. Founded by an expert team of medical specialists and technology veterans, Entel Healthtech looks forward to providing high-quality critical care to patients even in the remotest corners of the country, round the clock. • Using advanced Artificial Intelligence tools and robust technologies, Entel Healthtech aims to solve India’s problem of lack of critical resources in the field of healthcare. • An expert team of tele-intensivists keeps an eye on patient’s health and vitals using 24×7 tele-coverage feed acquired by the mobile kiosk. Along with real-time feed, they access the patient’s health records and information on on-going treatment.
Direct benefits for a Hospital & Patient through tele-icu
1/3rd Cost Saved through TeleICU Services
Shorter length of Stay for ICU patients
Lesser Mortality rates
24X7 remote monitoring “Crisis Prevention over Crisis Intervention”
Implementation of International Critical care best
Digitising ICU Data
Improving the quality and clinical output
Acts as an extra pair of Eyes & Ears in the Hospital ICU
Capacity Building of Bed Side Staff
Entel Healthtech has implemented Tele-ICU located at Godhara, Mahisagar district. The unit established in November 2021.
Saving Life Remotely A 47- year old female patient, was admitted to General hospital Godhra on December 07 2021. On admission patients have symptoms like tachycardia, Breathlessness,. patient had known case of HTN/ DM .Patient have no any other previous medical history. And vitals are, BP- 190/109 mm hg, pulse- 125, Temp- normal.
Using technology developed and set up at a remote ICU, Team of Experience Critical Care Specialist at Entel Healthtech’s Command Centre clinically examined the patient thoroughly and showed stability in all vitals parameters. During this period of time necessary Reports like Blood investigation + ECG + Chest x ray + ABG had been done.
In this examination there was an abnormality found in ECG and ABG(Compensated respiratory acidosis ). CXR shows pulmonary congestion. By this way Patient was diagnosed with Acute congestive cardiac failure/COPD.
The TeleICU platform used to consult with the primary consultant and patient’s relatives about the future treatment and course of action.It was decided to give medication that can help to reduce chest congestion, control blood pressure and decrease breathlessness.
Throughout the observation and treatment period,Regular discussions were done with the primary consultant about regular reports and medication via TeleICU platform.The patient’s condition improved and he is getting better by each passing day.
These success stories will go a long way in accepting remote monitoring for critically ill patients.
Tele ICU Facility Inaugurated at Visnagar, Gujarat
Interesting Telemedicine Research Studies
a.Impact of Telemedicine on Prenatal counseling The transition from an in-person consultation to a tele-consultation has been significant since the pandemic due to COVID-19. Expecting mothers with a pregnancy complicated by a fetal surgical anomaly were studied before using tele-consultation and after using tele-consultation by a team of researchers. A Mixed method study was performed on the expectant mothers, where both qualitative and quantitative data were analyzed. To know more, please click the link below. https://www.sciencedirect.com/science/article/abs/pii/S002248042200470X
b.Exploring mHealth potential to improve kidney function: secondary analysis of a randomized trial of diabetes self-care in diverse adults
Individuals living with Chronic Kidney Disease (CKD) are likely to have comorbid Type 2 diabetes. A team of researchers used Telemedicine intervention to reduce the glycemic index in the patient and studied whether it reduced the progression of CKD. The telemedicine support intervention emphasized medication adherence, diet and exercise which significantly improved the individual’s glycemic index. The details of the study can be found by clicking the link below. https://bmcnephrol.biomedcentral.com/articles/10.1186/s12882-022-02885-6
Telemedicine – News from India & Abroad
Your Smartphone can Now Measure Blood Oxygen Levels: Here’s How? No need to search for pulse oximeters. Your own smartphone camera and flash can now help measure blood oxygen levels easily at home, suggests a new study…..Readmore
Can AI-Powered Robots Laugh at Human Jokes? Artificial intelligence-powered robot Erica is now trained to laugh at human jokes. Since at least the time of inquiring minds like Plato philosophers and scientists have puzzled...Readmore
Artificial Intelligence Shows Promise in Tuberculosis Detection An artificial intelligence (AI) system developed could help detect tuberculosis (TB) in chest X-rays at a level comparable to radiologists resources.TB is an infectious disease ….Readmore
Telehealth Linked to Reduced Opioid Overdose Risk? During the pandemic, the extended use of telehealth for opioid use disorder is linked to decreased risk of overdose, revealed a new study.Published today in JAMA Psychiatry, this study was ….Readmore
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
The month of August issue has three interesting articles. The first is from Anay on consultations between two doctors, relating to the care of a patient, as telemedicine consultations and the legal requirements.
The second is from Prof Ganapathy about having a band of clinician scientists and clinical technologists to help with growth of telehealth. He also emphasizes the role of clinical research.
Teladoc has been in the news and we bring you the experience on how these telemedicine robots have the capabilities to carryout basic clinical examination (such as checking blood pressure and heart rate) on their own, as instructed by the doctors. At Meenakshi Mission, these robots have empowered the doctors to treat patients anywhere and anytime.
Thank You Dr. Sunil Shroff
Chief Editor
President – TN Chapter – TSI
Teleconsultations between doctors
Mr. Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist Law Firm
Ms. Eshika Phadke Associate, Arogya Legal – Health Laws Specialist Law Firm
Telemedicine, as a practice, is typically associated with consultations that take place remotely between a doctor and a patient. While doctors are familiar with the Telemedicine Practice Guidelines, 2020(“Telemedicine Guidelines”) and its applicability to such consultations. However, it should be noted that the Telemedicine Guidelines has adopted a broader interpretation of what amounts to a teleconsultation, and classifies consultations between two doctors, relating to the care of a patient, as telemedicine consultations.
In practice, a doctor (“treating doctor”) may often need to consult with another doctor (“consulting doctor”) to determine the best course of treatment for a patient. For example, while consulting with a professional of another specialty or with extensive experience in treating a certain condition. Such consultations would generally take place when the patient is physically present with the treating doctor, but there is no bar on all three participants consulting remotely.
The mechanism for such consultations is largely similar to traditional teleconsultations between a patient and doctor. However, there are certain considerations that a doctor should be mindful of while engaging in a consultation involving another doctor.
Explicit Consent The general principle is that when a patient initiates a teleconsultation with a doctor, their consent is implied. However, in case of a consultation between two doctors and the patient, even if the patient has initiated the consultation, it is best to obtain explicit consent from the patient for the consultation with both doctors.
In the event that the treating doctor initiates the consultation, explicit consent is required to be sought from the patient prior to proceeding with the consultation. Such consent may be obtained through a text message, email or voice recording, or the doctors may have the patient categorically confirm that he/she consents, and record the same. As a matter of practice, both the treating doctor and the consulting doctor should record the consent in their notes.
The treating doctor should also obtain explicit consent from the patient before sharing information or records with the consulting doctor, even if the patient has consented to the consultation.
Patient History The consulting doctor may rely on the information provided by the treating doctor, including their findings in a physical examination. In addition, the consulting doctor may gather additional information from the patient, as they deem fit. The consulting doctor may recommend to the treating doctor that certain additional tests be carried out if required.
Control of case As per the Indian Medical Council (Professional conduct, Etiquette and Ethics) Regulations, 2002 (“Code of Ethics”) the consulting physician is required to discuss the diagnosis treatment plan with the treating doctor, and should not take charge of the case.
In case of a consultation involving two doctors, the consulting doctor should be mindful that the case has not been handed over to them, and that the ultimate control rests with the treating doctor. The treating doctor must exercise professional discretion and determine how to proceed with the patient’s care.
While recommending a treatment plan, the consulting doctor should be mindful of the restrictions, if any, that the treating doctor may be subjected to. For example, if the treating doctor does not have the training to administer a treatment or procedure, the consulting doctor should clarify that the patient would need to seek such treatment from another professional. However, in doing so, the consulting doctor should be careful to not professionally undermine the treating the doctor or his treatment plan.
Necessity for formally dually trained Clinician Scientists and Clinician Technologists
Prof. K. Ganapathy
Past President, Telemedicine Society of India & Neurological Society of India | Hon Distinguished Professor The Tamilnadu Dr. MGR Medical University | Emeritus Professor, National Academy of Medical Sciences | Formerly Adjunct Professor IIT Madras & Anna University | Director Apollo Telemedicine Networking Foundation & Apollo Tele Health Services | URL: www.kganapathy.in
Healthcare necessitates bridging the gap between full time clinicians, full time medical researchers and full time engineers and technologists working in Healthcare. I have pioneered Stereotactic radiosurgery in 1995 and have always been interested in the use of Technology in Healthcare. In the article that has a link provided, I speak about the relevance in emerging economies and strongly supports the plan to create a band of clinician scientists and clinician technologists. This will also ultimately help the growth of Telehealth. The article is available at:https://issuu.com/verticaltalk/docs/ahhm-issue-57/20
2. RELEVANCE OF CLINICAL RESEARCH
The growth and development of any discipline or area ultimately depends on providing unequivocal scientific evidence that a particular facility / intervention in this case Telehealth (Remote Health Care) has indeed made a significant difference. Unfortunately in the real world priorities for clinical research takes a back seat. In this presentation I share “Lessons learnt & Opportunities missed: over 54 years in Clinical Research”. Hopefully the present generation with all the technology at its command will not only evangelise Telehealth but equally important produce hard core irrefutable evidence that telehealth needs to be incorporated into the mainstream of Healthcare.
Mobile Teladoc Health Robots at MMHRC
Mr. P. Sundarraj Head – R & D, Meenakshi Mission Hospital and Research Centre, Madurai
In India, despite several advancements made in the medical field, the benefits are still available to the privileged who are residing mainly in the urban areas. It is known fact that 75 percent of the qualified doctors practice in urban centres, whereas the vast majority of India’s population live in the rural areas. To address the issue, Meenakshi Mission Hospital and Research centre in Madurai extends its support by establishing Telecare centres in remote rural areas. So far it is established 15 centres in and around southern Tamilnadu with the support of public undertaking sectors & corporate.
To bridge the health and technology intensively, MMHRC gone for next phase and establish India’s first telehealth robots.
First of its kind in India, Meenakshi Mission Hospital and Research Centre have deployed 16 mobile Teladoc (USA) health robots. The primary objective of the Teladoc robot is to argument the diagnostic abilities and efficiency of health care delivery of patients irrespective of their physical location.
The Teladoc telemedicine robots have the capabilities to carry out basic clinical examination (such as checking blood pressure and heart rate) on their own, as instructed by the doctors. As 10T devices, they can be used to control other advanced diagnostic equipment such as CT and MRI scan machine. These robots can collect and process data from other diagnostic equipment and present it to doctors to help them make precise clinical questions with the help of Teladoc, doctors from different disciplines, from all parts of the world, can come together to treat and monitor patients all the time.
At Meenakshi Mission, these robots have empowered our doctors to treat patients anywhere and anytime. Our ambulances will also be equipped with Teladoc robots. By doing this, the patient can immediately get in touch with the emergency and ICU specialists along with the other specialists of all departments. This means that specialists like neurologists and cardiologists can begin vital treatment even as critically all patients are on their way to the hospital.
We are all set to explore ways to use this novel technology to provide expert diagnosis from Madurai to patients in other parts of the country and put world class health care with in every ones reach.
Telemedicine – News from India & Abroad
Can Artificial Intelligence Detect Autism Early? Artificial intelligence (AI) can soon be used to detect autism spectrum disorder (ASD) early, reveal researchers at the University of Arkansas.Han-Seok Seo, an associate professor with a joint appointment in food science…..Readmore
AI Algorithm Helps Cure Epilepsy An artificial intelligence (AI) algorithm developed by researchers detects subtle brain abnormalities which cause epileptic seizures.The Multicentre Epilepsy Lesion Detection project (MELD) used over 1,000 patient…Readmore
New Stamp-sized Ultrasound Stickers can Monitor Your Internal Organs New stamp-sized ultrasound sticker has been developed by a team of engineers in the US. The device can stick to skin and can provide continuous ultrasound imaging of internal organs for 48 hours…..Readmore
Can Artificial Intelligence Improve Stroke Diagnostics? Artificial intelligence (AI) technology identifies when a patient is having a stroke caused by emergent large vessel occlusion (LVO), therefore making them a candidate for endovascular therapy (EVT)….Readmore
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
The executive committee (EC) of Telemedicine Society of India has for the last few months been working on amendments of the society’s bye-laws. In the last 20 years so much seems to have changed including the term telemedicine. First Medicine was replaced with health (Tele-Health) and then Tele was replaced with Digital. The amendments will be circulated by the secretary of the society (Dr.Murthy) and all members should try and send their input so that the new bye-laws are all inclusive. We have published the link here of the bye-laws for the convenience of the members and for their feedback. The Special General Body that was called for this purpose had only 30 members in a society of over 700 members.
The month of July also saw the physical meeting of the EC at Kochi to discuss these amendments plus review the arrangements for the forthcoming annual meeting in November at Kochi.
At Kanpur, Dr. Saroj Mishra put up a great meeting on AI in healthcare and at Srinagar Dr. Farooq Ahmad Wani celebrated the Digital Week – reports are enclosed.
Thank You Dr. Sunil Shroff
Chief Editor
President – TN Chapter – TSI
Draft Bye Laws of TSI
Article I: Name of the Society The name of the of the society shall be “Telemedicine Society of India” herein after referred to as “TSI” or the “Society”; an independent scientific body operating on a notfor-profit basis and not aligned to any particular political party or religion.
Article II: Title These byelaws shall be called the byelaws of the Telemedicine Society of India.
Article III: Office of the society: 1. The registered office of the society shall be situated in Room No.303, 2nd Floor, School of Telemedicine & Biomedical Informatics (STBMI), Sanjay Gandhi Post Graduate Institute of Medical Sciences (SGPGIMS), Raibareli Road, Lucknow- Uttar Pradesh226014, India.
Article IV: Status of Society 1. The Society shall be juristic person and shall have a perpetual succession and can sue, and also be sued, in its own name through the person appointed by the TSI for the purpose.
Article V: Aims & objectives 1. The aims and objectives of the Society will be in furtherance of the activities it wishes to undertake in the field of digital health, and any ancillary activity which has to be accounted for the smooth and continued functioning of the Society. The specific objects have been outlined as below:
(i). To promote and encourage application of Telemedicine along with development, advancement and research in the field of Telemedicine/Telehealth/eHealth/Digital Health (which terms may be used interchangeably in different contexts) and associated fields; for improvement in the overall Healthcare access.
(ii). To promote, increase awareness on matters related to telemedicine, via all means and media which exist currently, or may be developed in future.
(iii). To encourage and promote application of telemedicine technology in clinical care, education and research in the health sector. The Society may work with any person for promotion of corporate social responsibilities of the companies, under the law.
(iv). Fostering networking and collaboration among interest groups in telemedicine technology and professionals from different streams of science, health care providers, policy makers, NGOs and industry.
(v). To promote training of students, health professional, research fellows and technicians in various aspects of telemedicine, on free of cost or suitable arrangement to meet out the expenses as the EC decides Also, to co-ordinate with academic institutions and premier think-tanks in the TM/associated field, industry associations, regulatory authorities, (like National Medical Commission/DCI, AICTE, DOEACC, as the case maybe); in developing curriculum for training courses and incorporating appropriate modules in the healthcare and associated training programmes.
(vi). To conduct regular meetings, symposia, seminars on matters related to digital health.
(vii). Spearheading the development of appropriate clinical and industry policies and standards, in view of adoption of and integration with Telehealth.
(viii). Disseminating knowledge in telemedicine field by publishing brochures, periodicals, and journals, through Society’s own website, or third party literature.
(ix). To work in close collaboration with scientific organizations and the industry in development and implementation of innovative products & services related to Telehealth. Organizing trade exhibitions during annual meetings of the society or at any opportune event.
(x). “To develop, co-ordinate and conduct knowledge and capacity building exchange programmes, with national/international organizations engaged in activities in the field of telemedicine
(xi). To work towards getting recognized as an accreditation body for Telemedicine/Telehealth/eHealth etc.
(xii). Spearheading or collaborating in the development of appropriate clinical and industry policies and standards, in view of adoption of and integration with Telehealth
(xiii). Facilitate Individuals/organisations to start/improve TM practice with proper networking and necessary guidance
Article VI: Definitions 1. In the interpretation of the Byelaws, unless there is something inconsistent or repugnant with the subject or context, the following words shall have the meaning given as hereunder:
(i).“The Society” shall mean the TSI Society having its registered address at School of Telemedicine, SGPGIMS, Raibareli Road, Lucknow
(ii).“Member” shall mean any type of Member as defined in article VII, whose application for Membership: has been accepted in accordance with the Byelaws and is a Member paying the appropriate subscription charge(s) as applicable to their category. For the purposes of proceedings under the Societies Registration Act, 1860 (the Act), no Member shall be entitled to vote or be entitled to the benefits of membership, if their subscription at the time of voting have been in arrear for a cumulative period of 2 months.
(iii).“General Body” shall mean the general body of the Society consisting of all the members of the Society. The General Body of the Society shall be comprised of President, Vice President, President-elect, Treasurer, Members of the Executive Committee and other Patron, Corporate, Professional, Startup and Academia Members.
(iv).“Executive Committee” (EC) is same as the Governing Body of the Society defined by the Act and shall mean the Committee that is constituted in accordance with Article IX of these Byelaws and to whom the management and affairs of the Society are entrusted. The Society shall have the following officers, who shall be the members of the Executive Committee – President, President Elect, Vice President, Immediate Past President, Hony.Secretary, Jt.Secretary,Treasurer and such other nominated members of the Society as confirmed during the AGM. The term of an EC will be for a period of 2 years.
One Day National Workshop on Telemedicine & Artificial Intelligence held at the IIT Kanpur Outreach Centre in NOIDA
Prof. S. K. Mishra, MS, Dip NB, FAMS, FACS Distinguished Visiting Professor, Gangwal School of Medical Science and Technology, Indian Institute of Technology, Kanpur
One day national workshop on Telemedicine & Artificial Intelligence was held on 2nd July 2022 at the IIT Kanpur Outreach Centre in NOIDA. This event was organized by newly launched Gangwal School of Medical Science & Technology, IIT, Kanpur in hybrid mode involving digital health policy makers from government, Telemedicine practitioners from medical community both from public and corporate hospitals and academics from technological institutions from country and overseas.
The workshop was inaugurated by Dr. R S Sharma, CEO, National Health Authority, Government of India who enlightened the participants on the activities undertaken at National level to facilitate rapid adoption on digital technologies for health in the care delivery pathway ensuring universal access to health care services. Earlier Prof. Ashutosh Sharma, former Secretary DST and currently Professor at IIT Kanpur welcome the chief Guest, dignitaries, invited speaker and participants. Professor Abhay Karandikar, Director, IIT Kanpur in his address spoke about the vision of IITK in setting up the School of Medical Science and Technology and various Centres of Excellence in the campus. He stressed the relevance of medical technology in advancing modern healthcare in particular and the need for self-reliance in making quality health services affordable and accessible to billions of population of not only India but low and middle income countries around the world.
The scientific sessions were divided into three sections, the first section covered detailed deliberation on policy and procedures on digital health by Mr. Vikram Pagaria from National Health Authority. The second section addressed the telemedicine technology and it’s applications in various domains like Radiology, Pathology, Surgery, Ophthalmology as practiced in public and corporate hospitals were addressed by medical experts. The National Telemedicine System using e-Sanjeevani was presented by C-DAC, Mohali in great detail. The future plan of development of Version 2.0 of e-Sanjeevani was announced which will have options of integration of third party medical devices in particular point-of-care diagnostics based on IoT technology. The third section focused on application of artificial intelligence addressing it’s usage in remote patient monitoring in ICU setting, Mental health, rural telehealth care system etc.
The concluding Round Table had a brain storming session involving more experts in additions to session experts to develop strategy and vision of developing actions plan in the upcoming centres of excellence in telemedicine and AI.
The list of Speakers include; Mr. Vikram Pagaria, National Health Agency, Govt. of India, Prof. K Ganapathy, Apollo Telehealth Network Foundation, Chennai, Mr. Praveen Srivastava, Associate Director & Head, Health Informatics Dept., C-DAC, NOIDA, Dr. Suchita Markan, Scientist E, Medical Device and Diagnostics Mission Secretariat, Indian Council of Medical Research, Rajesh Kaushish, Asst. Director, Dept. of Health Informatics & Medical Electronics, Center for Development of Advanced Computing, (C-DAC), Mohali, Dr. Arjun Kalyanpur, Chairman, Tele-radiology solutions, Bangalore, Dr. R Kim, Director, Arvind Eye Hospital System, Madurai, Dr. Sangeeta B. Desai, Head, Dept. of Pathology, TMH, Mumbai, Prof. S K Mishra, Distinguished Visiting Professor, Gangwal School of Medical Science & Technology, IIT Kanpur, Dr. Vijayakumar Chinnadurai, Scientist F. Cognitive control and machine learning center, INMAS Delhi, Prof. T K Srikanth, eHealth Research Center, IIIT, Bangalore Tele-mental Health Mission Task Force, MoH&FW, Govt. of India, Dr. Raghu Dharmraju, President, ARTPARK (AI & Robotics Technology Park)@ IISc, Bengaluru, Dr. Dileep Raman, Co-founder, Cloud Physician, Bengaluru, Dr. Presanna Desikan, University of Minnesota, USA, Mr. Vimal, Wakhlu, Former CMD, TCIL, DoT, Govt. of India & Vice President, ITU-APT Foundation, Prof. Sunil Shroff, Sr. Consultant Urology and Renal Transplant Surgeon , Madras Medical Mission, Chennai & President, Tamil Nadu state Chapter, TSI, Editor, TSI News Letter, Prof. P K Pradhan, Dept. of Nuclear Medicine, Nodal Officer, SGPGI, Lucknow Telemedicine Programme & President, Telemedicine Society of India, Prof. Anjali Mishra, Professor, Dept. of Endocrine Surgery, Member, SGPGI.
The workshop highlighted the necessity of telemedicine and AI in the health system in the country. In an effort, several govt. policies over the past couple of years led by the National Health Authority have paved the path for changing Indian healthcare through the advancement of AI and Telemedicine in healthcare.
In view of the inadequate healthcare, the speakers deliberated the below mentioned aspects:
The necessity of the work plan to transform the digital structure in the rural areas is devoted to developing telemedicine to provide quality healthcare services locally and at lower costs.
Artificial intelligence also plays a significant role in diagnostics and digital patent evolutions. An analysis of health-related data collected and measured by digital devices. AI-based systems in performing medical work in specializations including radiology and pathology are becoming increasingly prevalent and desirable in preventative medicine in the Healthcare domain.
Digital pathology plays a vital role in deep learning for identifying the target of interest. Also, highlighted the challenges in digital pathology image analysis. The nature of diagnostics has rapidly changed owing to an explosion in the availability of patient data for disease diagnosis.
Digital technologies in current surgical practices & potential AI contribute a new development to core the subfield of AI reviewed and identified the key concept and techniques within AI that are driving innovation across industries. AI has the potential to revolutionize the way surgery is taught and practiced with the future optimized for the highest quality patient care.
The guidelines of telemedicine were discussed and how to overcome the challenges like ethical concerns and lack of infrastructure in rural regions. Reimagining the healthcare industry by embracing telemedicine and AI.
The workshop concluded successfully achieved the aim by the valuable prospects from attendees. A compendium document will be developed in a fortnight time with further inputs with well laid down guidelines for the future activity at the Centres of Excellence on Telemedicine and Artificial Intelligence.
At Srinagar – SKIMS Celebrates Digital Week 2022
The department of Electronics & Communications/ Information & Technology and Hospital Administration SKIMS celebrates digital week showcasing various digital services at SKIMS.
Director SKIMS & Ex-Officio Secretary to Government, Prof. Parvaiz Ahmad Koul while speaking on the occasion emphasized for making all the services available in the hospital On-line to benefit patients as well as to enhance efficiency, transparency,accountability and accessibility, which are embedded with digital system and services , he said. He appreciated the department of E&C/IT, Hospital Administration for taking initiatives in this direction and making some of the services digital end-to-end in the hospital.
On the First day of the programme, a review was taken in the SKIMS Auditorium on the implementation of various digital services in the Administration of SKIMS like e-Office, e-Tendering, JKPaysys and other on-line services in these areas and also hands-on training on e-office implementation in un-covered areas of SKIMS was organized.
On the occasion Additional Director SKIMS & EOSSG (Mr. Gulzar Ahmad Shabnum), HOD Endocrinology (Prof. Bashir Ahmad Laway), Medical Superintendent (Prof. Farooq Ahmad Jan), Superintending Engineer E&C/IT, Er. Farooq Ahmad Wani) and Superintending Engineer Mechanical, Er. Muzaffar also addressed the audience and highlighted the importance of e-services.
The programme was attended by the officers/officials of General Administration, Hospital Administration, Materials Management, Finance & Engineering departments.
Issued through, PR Office SKIMS
Namma Bengaluru Award for Dr. Bhaskar
Dr. Bhaskar received the prestigious ‘Namma Bengaluru Award’ under the Health care professional of the year 2021 category – recognising the service during the Covid 19 pandemic.
Telemedicine – News from India & Abroad
New Discovery on Mental Illness Indicators Using the AI
New research may lead to early diagnosis of devastating conditions such as Alzheimer’s disease, schizophrenia and autism — in time to help prevent and more easily treat these disorders, as done by Georgia State University’s TReNDS Center…..Readmore
Artificial Intelligence to Diagnose Birth Defects in Fetal Ultrasound Images
In a new proof-of-concept study led by Dr. Mark Walker at the University of Ottawa’s Faculty of Medicine, researchers are pioneering the use of a unique Artificial Intelligence-based deep learning model as an assistive tool for the rapid and accurate reading of ultrasound images….Readmore
Neuroendovascular Robotics Improves Safety of Complex Procedures
Through robotics, stroke surgery and other neuroendovascular procedures could be made safer and easier. A new multi-articulated, self-steering microcatheter for neuroendovascular surgery has the potential to increase technical precision….Readmore
Can Artificial Intelligence Help Predict Future Impacts of Coronavirus?
Developing Artificial Intelligence (AI) can help forecast the future impacts of the coronavirus, its variants and other evolving viruses, suggests a new study. The National Institutes of Health have awarded Michigan State University….. Read More
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
This issue covers important topics related to Tele-Neurology. We are hoping to bring such focussed newsletters from time to time.
This month also saw submission of draft guidelines of the National Medical Commission and includes some of the many recommendations sent to the apex body. These guidelines would have an impact on over a million medical practitioners of the country. Ms. Bagmishika Puhan our health technology lawyer with many others have submitted a document to NMC and so has TSI national body.
Thank You Dr. Sunil Shroff
Chief Editor
President – TN Chapter – TSI
National Medical Commission, Registered Medical Practitioner (Professional Conduct) Regulations, 2022- Recommendations to the Draft Guidelines
Bagmisikha Puhan
Dr Sunil Shroff
Wing Cdr (Dr) Lavanian Dorairaj (Retd)
Col (Dr) Ashvini Goel (Retd)
Mayank Agarwal
An extensive review and multiple discussions have resulted in the following suggestions for implementation in the draft National Medical Commission, Registered Medical Practitioner (Professional Conduct) Regulations, 2022
Guideline 11 – Guidelines for Practice of Telemedicine in India: Enabling Registered Medical Practitioners to Provide Healthcare Using Telemedicine.
1. Under Scope at 1.2 – it is necessary to convey it to the practitioners that the exclusions are only rendering them to be outside the scope and applicability of these Guidelines and are not illegal in practice or otherwise. There is a lot of incongruity amongst the minds of the practitioners, with respect to cross-border consultations (during international holidays), standards and interoperability.
2. Under 1.4 – discussing Telemedicine Applications, there is reference to “emergency consult for immediate assistance or first aid etc.” – this should be amended to state emergency consult for immediate assistance, life-saving measures, first aid only with advice for immediate in-person consult or ER visit as available locally.
3. Under 3.2- Identification of the RMP and patient is mandatory – there is a requirement that RMPs should begin consultation by introducing themselves, with mandatory details – there is no clarification provided with respect to consultation in continuity of an in-person consultation/ follow-up consultation; this requirement should not be applicable in such situations.
4. Under 3.4, there is a mandatory requirement to have patient consent which has been further segmented into implied and explicit – depending on who initiates telemedicine consultation. It is imperative that this cannot be the case because tied to the telemedicine consult is the process of seeking personal and sensitive personal information of the patient and the applicable information technology laws mandate that the explicit prior written consent of an individual is acquired, prior to the collection and processing of any sensitive personal data so shared. Hence, while implicit consultation may be acceptable for initiation of a telemedicine consult, there is a requirement to process explicit consent prior to processing of sensitive personal information.
5. Prescription Template – There is a template provided within the proposed Guidelines which was also the same in the earlier iteration. It has requirements to the tune of having details about “provisional/appropriate diagnosis”, “LMP”, “special instructions”, “Investigations”, “Lab Findings”, “Chief Complaints” provided within the prescription.
a. While we agree that these parameters must be captured by the RMP, it is important to note that in the online set-up this prescription is also enabled to be shared with a pharmacy. Without any appropriate privacy laws in place, allowing such details to be shared ahead would not just trigger privacy concerns, but may also cause social stigma attached to medical conditions related to STDs/ VDs, Psychiatry-related, MTP, communicable diseases. Furthermore, it is not necessary for the pharmacist to review and retain information related to the “provisional/appropriate diagnosis”, “LMP”, “special instructions”, “Investigations”, “Lab Findings”, “Chief Complaints” – they need the seal, appropriate prescription made out, and the necessary details of the RMP for dispensation. This excessive sharing is in violation of the privacy of the individual, which has been recognized as a fundamental right by the apex court of the country in Justice KS Puttaswamy (Retd) v. Union of India.
b. It is noteworthy that these details can be retained by the pharmacy, and may be used for data analysis, which is not envisaged by the RMP or the patient and will amount to a strict violation of the privacy principles.
c. At pt. 9, there is a requirement that identification and contact details of the patient must also be added to the prescription – this is again inconsistent with the requirement, purpose of a prescription. This is also excessive in nature and is not in conformity with the template at Annexure 2.
d. There must be stress on digital signatures/ electronic signatures (including AdobeSign, DocuSign, etc.) to ensure that the prescriptions are properly time-stamped and are valid. In absence of this, where scanned files or images of signatures are used by the RMPs to issue a prescription – there could be abuse of this by online pharmacies, or the users themselves, to create / issue new prescriptions for seeking drugs.
e. There is also a requirement under pt. 9, that the e-prescription be valid for a period of 2 weeks from the date of issue or once a pharmacist dispenses the prescribed medications – this might not be a sustainable solution for chronic conditions – and also if a prescription is valid for 2 weeks only, the patient will have to pay further for issuance of another subscription even for a refill for a chronic condition or the likes – this provides platforms with an opportunity to deny treatment or deny dispensation of medication / drugs after a period of 2 weeks.
f. There is a separate template provided under Guideline 2 for writing prescriptions rationally. Similar template should be used for teleconsultations for reconciliation of digitization of electronic/ health records of the patients. The ePrescription for telemedicine consultations has excessive, and confidential data that is not relevant to the pharmacy. It is in fact a case summary and not a prescription. It should be made identical to a standard prescription as mentioned in para-Guidelines 2 Prescription.
6. The Guidelines do not permit technology platforms to indulge in providing ratings, feature testimonials of practitioners on the platform – this will be a hindrance to the users, for the ones who are not familiar with the region / practice of the physician – they tend to rely on these to be able to understand how the particular RMP may address a particular situation, or if they have good bedside manners in dealing with patients. This is indeed a guiding factor to the consumers/ patients of the platform – denying them this right, is impinging upon the users’ right to freedom of speech and expression. While the technology platform may be required to substantiate the ratings – to ensure parity with the listing the Guidelines should not strip this from the platform to enable users make an informed decision in engaging with an RMP for teleconsultation.
7. Under “duties and responsibilities of an RMP in telemedicine”, at para 15, there is a requirement for RMPs to ensure that their medical indemnity cover includes cover for telemedicine – we seek clarification with respect to legislative changes in line with this under professional indemnity and insurance norms.
8. Under “Consultations between RMPs with other RMPs” – there is mention of considering e- ICUs during emergencies like COVID-19 pandemic – remote areas invariably have a specific/ high demand for consultations of this nature. Limiting the prevalence of e-ICUs in cases related to emergencies like pandemics will defeat the purpose of this initiative.
9. Chapter 11 TPG2022 Para 3.5: There needs to be a distinction between a telemedicine consult with a NEW patient for the 1st time as compared to a telemedicine consult with an old patient for a new condition. In the latter case, many if not most details of the patient are already known to the RMP. So, in the latter’s case more Rx flexibility should be allowed.
10. Chapter 11 TPG2022 Para 3.7: Change “If the patient’s condition can effectively and appropriately be managed via telemedicine” to “Once the patient is triaged and the RMP is of the opinion that the condition can effectively and appropriately be managed via telemedicine”.
11. Chapter 11, 1.2. Autonomy and privacy of the RMP: add subpara 9: “The RMP has the right to announce that he/she is terminating the consult (along with the reason) if he/she feels that the same is a crank/prank or abusive call. Details of the same should be recorded to take forward legally, if so desired.”
Guidelines for RMPs and Technology Platforms
12. At 5.5, the onus of ensuring valid registration of the RMP is wholly on the owners and administrators of the technology platform. Owing to lack of continuous online/ physical access to national medical register or respective state medical councils’ registers, several tech platforms are already constrained to avoid onboarding such RMPs whose details cannot be verified by this process causing a loss of opportunity to the RMP and facilitating tech platforms to censure admission of such RMPs. A separate cell/ body should be created to enable platforms to achieve this or seek verifiable information from. There is no set pattern or manner provided to convey if the details of the RMP are legitimate or not; we seek clarification on this specific aspect.
13. At 5.7, tech platforms have been disbarred to counsel patients on the basis of AI and ML, it is pertinent to note that counsel is a wide term and may also include gathering of information from end users, triage of patients, provisioning of general information/ FAQs, which can all be done seamlessly, accurately by these automated tools without disrupting the functioning of the RMP. We are of the opinion that instances like triage, data gathering, or automated responses in form of FAQs be allowed by the usage of AI and ML.
14. At 5.9, its stated that the tech platform may be blacklisted for the violation of TPG by EMRB/ NMC, however, there is no avenue for RMPs to be able to access this publicly – a provision to that effect should be added. Following principles of natural justice, the tech platform should also be provided with opportunity to come back into the ecosystem in the event where this provision is triggered and made applicable to them.
15. It is also important to ensure that there is statement made to the effect that the TPG are technology agnostic and change in technology, mode and media of communication will not impact the compliance that is prescribed and expected under the laws.
In addition to this, our concerns with respect to the initial provisions of the draft guidelines are as below:
16. Chapter 2 Para 4: The prefix of Med Dr is not appropriate as a Doctor of Modern Medicine practices medicine as well as surgery. It would be better to continue to prefix Dr. followed by the full name and prefixed by the qualification. e.g. Dr. Name Family-name MBBS; Dr. Name family-name, MBBS, MS (xxx). The MBBS prefix clearly denotes modern medicine as compared to ayurveda or homeopathy.
17. Chapter 2 Para 4 (E): The RMP should be allowed train, utilize and to provide a certificate of competence to an assistant that he/she has trained under him/her. This would allow increased support in rural areas (especially via telemedicine) while ensuring that the responsibility of ensuring competency of the trained assistants rests with the RMP providing such certifications. This is to bring more clarity to this para with respect to point in chapter 2 para 10 (B) which essentially states the same.
18. Chapter 2 para 8: Suggest “Every RMP is expected to prescribe drugs using generic names” to “Every RMP, as far as possible, must try to prescribe drugs using generic names”.
19. Para 13 D: Suggest “the RMP shall fully digitize records.” To “the RMP shall digitize records.” This is because the efforts to digitize records may not be completed in 3 years.
20. Para 41 (8): An RMP cannot be restricted from practicing in any state. This would affect healthcare adversely especially government, armed forces, etc. doctors who are frequently transferred and who frequently travel to different states for short periods on temporary duty. It would also affect specialists who travel to different cities to provide specialist care to needy patients. Once a doctor is certified and registered in one state he should continue to be allowed to practice all over India as per need. He may, if he so desires, move to register in another state.
21. Chapter 10 CPD: No mention has been given as the age limit for mandatory CPD for registration license renewal. It is generally exempt for seniors. E.G. in Maharashtra it is 65 years after which a RMP need not CPD points for license renewal. Recommend an age limit of 60 years.
22. Under Chapter 2 concerning professional conduct of RMPs, at 9, there is a prohibition on fee splitting or commission imposed on RMP. In the event where the RMPs engaging with the tech platform, it is but obvious that the tech platform will be entitled to charge a fee towards the portal or services. This shall be a deterrent for the platforms. Also, this provision states that RMPs shall not use online forums for procuring patients – this is in conflict with the intent that may be evinced from an association of an RMP with a tech platform. For the entire ecosystem is premised on the fact that it allows the RMPs to widen their outreach, and also enables patients to identify and locate RMPs of their choice, accessibility and affordability.
23. In terms of prescription where the proposed guidelines expect that only generic names can be mentioned – it is worth considering that when RMPs use brand names, they are taking into consideration any enhanced efficacy in such drugs, affordability of the patient and also any positive feedback received or witnessed in their experience with other patients in consonance with their professional judgment. At times for chronic conditions, patients develop affinity, association with a particular brand over a period of time so prescribed to them; in this context, the substitution of the brand name with the generic name of the drug may erode their confidence in the advice of the RMP.
24. At the point of discussion of “Responsibilities of RMPs to each other”, it should be mentioned that in case of a treating physician and a consulting physician, there is a difference in the standard of care owed by an RMP, as opposed to the duty of care owed by the other. This was not mentioned in the earlier iteration, neither the first draft of the TPG, and this also does not find place here. As the draft regulations have delved deep into how relationships are forged or are perceived in case of ascribing duties and responsibilities, it must also consider commenting on the associated liabilities. Guideline 4 under “Assessment of attributability and the severity thereof” – at 2(9) indicates that the role that the doctor is expected to play will be considered – this could be expanded upon to bring out the specific relationship that exists between the treating and the consulting physicians/ RMPs. This becomes imperative in case of telemedicine consultation referrals, wherein the referred RMP may not have the necessary knowledge, history, comorbidities, with a particular patient, and must invariably rely upon the advice, inputs of the consulting physician.
We hope this is in order. We thank you for providing us with the opportunity to participate in this round of stakeholder consultation. We are willing to provide further information in this regard, should there be a need for the same.
Our group has also consulted several physicians, practitioners and have taken the liberty of providing changes to the draft so circulated, by including our suggestions within such document.
Teleneurology : Are we there?
Prof. K. Ganapathy
Past President, Telemedicine Society of India & Neurological Society of India | Hon Distinguished Professor The Tamilnadu Dr. MGR Medical University | Emeritus Professor, National Academy of Medical Sciences | Formerly Adjunct Professor IIT Madras & Anna University | Director Apollo Telemedicine Networking Foundation & Apollo Tele Health Services | URL: www.kganapathy.in
It was in 2015 that the author had pointed out (https://www.neurologyindia.com/text.asp?2015/63/2/142/156274) that there was not a single neurologist or neurosurgeon for a population of 935 million Indians. With 773 districts in India likely to have a medical college, no doubt the urban rural health divide will reduce. However not in the life time of my great grand children will there be an equitable physical distribution of super specialists in India. Of the 675 million internet users (48% penetration) 80% use mobile networks. The slogan today is “ Roti, kapada, makan, and bandwidth” A strand of RNA acting as Global CTO has indeed radically transformed the deployment of telehealth worldwide. The 6000 odd neurologists and neurosurgeons cannot cater to at least 30 million(excluding neuro trauma and neuro infection) requiring their services ref (https://www.neurologyindia.com/text.asp?2014/62/6/588/149365.) Teleneurology is obviously the only solution to extend the reach of the super specialists predominantly located in urban and suburban India. It is gratifying to see that this is slowly being accepted by the consultants and the beneficiaries (DOI: 10.4103/0028-3886.232346)
“Tele” is only a tool to achieve the end, which is making available the “neuro” component available in places where the latter does not exist., “Customer delight” is not a cliché used as marketing ploy. The role of the patient is changing. They are now at the center of self-care becoming a “digitally engaged” patient. Technology acceptance, behavioural modification, increasing digital infrastructure and requirements will cause a paradigm shift in delivery of teleneurology. For teleneurology to succeed the practitioners should strive to produce a “wow” effect. One needs to get into the mind of the end user. Healthcare is personal – it is very hard to feel your experience was excellent, when those treating you do not introduce themselves, or make eye contact, or say what they are doing to you and why. Conversely, when those simple things are addressed, the experience rapidly improves. Achieving excellence in healthcare is neither difficult nor expensive. It does not matter if care is cutting-edge and technologically advanced, if it does not take into account the patient’s goals. In fact it may not even be worth doing. Patients do not care how much the doctor knows. They want to know how much the doctor cares!!
Webside manners is replacing bedside manners of the 20th century. https://www.youtube.com/watch?v=BJYp7Ti8noo. Patient rapport is crucial particularly in neurology. 80% of messages are conveyed non verbally through body posture, voice intonation, the way one looks / sits, attire, movement of hands, arms and spontaneous smiling. The practice of medicine is an art, not a trade, based on science. This must be absorbed in the new science. Health care is a calling not a business.
Innovative methods like Group Telecounselling needs to be deployed. Contrary to a common misconception that doctor patient relationship is strictly confidential and always one to one, studies have revealed that patients are more @ home with other patients having similar problems. With acute shortage of neurologists and neurosurgeons, patients with common clinical conditions can be reviewed remotely in groups in one session eg seizures, post head injury sequelae, migraine etc. This would save time and be cost effective and enable larger numbers to get specialist care.
Distance has become meaningless. Geography has become History! The world will never be the same again. It is imperative that we accept and start deploying the “New Normal”. Technology enabled remote health care in neurosciences is here to stay.
Role of Telemedicine in Stroke
Veteran Major General Dr. S. Kumaravelu
Professor and Head Neurology, Ramesh Cardiac & Multispeciality Hospitals Pvt Ltd, Guntur
Stroke is the second leading cause of death after Coronary heart disease and the most common cause of disability in adults with huge social and economic burden. Telemedicine has revolutionised the management of stroke. It has a key role in prevention, hyperacute care, follow up and education of stroke. As regards prevention, it has a significant role to play in secondary prevention. We have regular telemedicine consultation for all our stroke patients to ensure proper diet control, and control of risk factors for stroke and ensure physiotherapy, both by a physiotherapist and caregivers.
Regarding hyperacute care, I shall narrate a different case scenario. Our patient a middle aged male was brought to our Emergency room at 11: 35 hours with history of sudden onset inability to speak, Confusion and staring look since 10:30 hours. He was a known patient of type 2 Diabetes Mellitus, Hypertension, Coronary artery disease with coronary artery bypass graft done and posterior circulation stroke on medication. He also had peripheral arterial disease as well with embolectomy done earlier. He came within a window period of 65 minutes. His imaging was done. His Magnetic Resonance Images and Angiogram are shown as Fig 1 and 2 respectively. The imaging was completed within 30 minutes. He was diagnosed as a patient acute ischemic stroke left middle cerebral artery territory with left middle cerebral artery occlusion. I, being the only Neurologist was away from the hospital. As the stroke was within 4.5hour window, it was decided to offer thrombolysis to the patient. Real time video consultation was given through a video portal. The family agreed to undergo thrombolysis. The thrombolysis clinical protocol was initiated. The indications and contraindications were enquired into. The severity of stroke was assessed using the NIHSS (National Institute of Heath Stroke Severity). His stroke score was 13. After taking informed assent from the wife, telethrombolysis was initiated with injection Actilyse 7 mg intravenous bolus followed by 63 mg intravenous infusion over the next one hour. Patient showed significant improvement with return of speech, and improving weakness of right half of body. Repeat Computerized Tomography angiogram of brain and neck revealed complete revascularization of the left middle cerebral artery.
Telestroke is an emergency telemedicine application that provides physicians with immediate access to neurologists who can support both the assessment and treatment of patients experiencing acute ischemic stroke symptoms. Using teleradiology to review Computerized Tomography (CT) images and videoconferencing solutions, the off-site neurologist can assess the patient and provide recommendations as to whether patients are candidates for thrombolysis and other interventions for acute stroke. The decision to use the thrombolytic (clot busting) agent tPA (tissue plasminogen activator) requires a Neurologist and the drug must be administered as soon as possible within the 4.5 hours following stroke onset. Telestroke is considered to be a key strategy to achieve equitable access to high quality care for stroke for all people. Without Telestroke, many patients living in and around communities lacking a neurologist would simply be denied the benefit of treatment with thrombolysis, or tPA, which is a best practice standard of care for acute ischemic stroke. This has been justified by the American Stroke association in their guidelines.
1. Telestroke/teleradiology evaluations of AIS patients can be effective for correct IV alteplase eligibility decision making.
2. Administration of IV alteplase guided by telestroke consultation for patients with AIS can be beneficial.
3. Telestroke networks may be reasonable for triaging patients with AIS who may be eligible for interfacility transfer in order to be considered for emergency mechanical thrombectomy.
4. Providing alteplase decision-making support via telephone consultation to community physicians is feasible and safe and may be considered when a hospital has access to neither an in-person stroke team nor a telestroke system.
Hence it may be concluded that Telestroke is the only solution to serve suburban areas and to increase thrombolysis rates.
Coming to the next aspect of telestroke, the most important aspect for advocacy and education regarding stroke is feasible through webinars and videoconferences. Imparting such knowledge will ensure equitable medical care beyond the urban limits to the needy patients in rural areas.
Fig 1. Magnetic resonance Image of the brain showing an acute infarct the left middle cerebral artery territoryFig 2. Magnetic resonance Angiography showing occlusion of left middle cerebral artery.Fig 3. Computerized Tomography angiogram of brain showing complete recanalization post thrombolysis.
Tele-Neurorehabilitation: A story from Mumbai
Prof. Nirmal Surya
Chairman, Surya Neuro Centre, Mumbai, Associate Professor, Bombay Hospital and Medical Research Centre, Mumbai.
Dr. Guhan Ramamurthy Consultant Neurologist, Institute of Neurosciences and Neurorehabilitation, BG Hospital, Tiruchendur, Tuticorin.
Tele-Neurorehabilitation: COVID-19 has ravaged economies, societies and human life across the world, and distanced people. The health care resources were strained and depleted. This had resulted in the inability of health care to cater to other non-COVID health services. With the increasing requirement of health care services, the inadequate reach of services to the needy patients and to make ends meet, the popularity of telemedicine emerged during these difficult times.
Telemedicine provides a platform for the exchange of information between the healthcare professionals, and the patient in arriving at the diagnosis and the management of patients. Telemedicine in Neurology (Tele-neurology) is useful for teleconsultations, tele-neurorehabilitation, and tele-research. The tele-neurology can be performed through mobile or computer-based applications. The Government of India has issued telemedicine guidelines for aiding the practitioners (https://www.mohfw.gov.in/pdf/Telemedicine.pdf). It is a prerequisite to obtain the patient’s consent (guardian’s consent in case of a minor).
Neurorehabilitation was no exception and had initially succumbed to the wrath of the COVID-19. However, the healthcare professionals had coped up with the new normal and adopted tele-neurorehabilitation. We were able to deliver tele-neurorehabilitation to patients with acute neurological deficits and chronic neurological deficits. It was useful to assess the patient’s deficit, formulate and tailor protocols to the requirements and needs of the patient and follow up on their progress. The tele-neurorehabilitation was as efficient as in-person neurorehabilitation in terms of clinical improvement. Further, the tele-neurorehabilitation had helped in providing the expertise in rural areas where it was scarce. The team members involved in tele-neurorehabilitation include a neurologist, physiatrist, physiotherapist, occupational therapist, speech and language pathologist, cognitive psychologist, nurse, social worker, and caregiver.
The story from Mumbai: The Epilepsy Foundation India is aimed at providing comprehensive care to patients with epilepsy. The comprehensive care includes tele-neurology consultation (HIPAA compliant), pharmacological treatment, tele-neurorehabilitation, and abolishing the misconceptions associated with epilepsy. The needy patients were provided with drugs, free of cost.
The tele-neurorehabilitation session included yoga therapy, cognitive therapy, counselling, occupational therapy, and physical therapy. Yoga therapy was provided as a weekly session to reduce stress and improve seizure control. The clinical psychologist provided weekly counselling sessions for the patients to better handle stress due to the stigma of patients with epilepsy and the burden created by COVID-19. The cognitive therapist provided cognitive training. The caregiver was encouraged to perform 3-5 sessions of cognitive rehabilitation per week. The patients were provided with physical and occupational therapy and were encouraged to continue 2-3 sessions per day for 5 days/week.
The model adopted during times of COVID-19 that warranted social distancing is also useful to deliver expert care to patients in rural areas and ensure continuity of care. The comprehensive care was provided to patients through tele medicine platform and serves as a model in the comprehensive care of epilepsy patients. It can be extrapolated and tailored to the management of other neurological disorders.
The tele-neurorehabilitation is also useful in the rehabilitation of patients with postural imbalance and falls by improving balance, improving motor strength in upper and lower limbs through strength training, cognitive rehabilitation using restorative or compensatory strategies and rehabilitation of patients with multiple sclerosis.
The way forward: Tele-neurology is cost effective, easy to use. It helps the patient to receive treatment from their home improving their comfort and saving travel time and cost. It also helps to prevent acquiring COVID-19, especially in the vulnerable patients with neurological disorders, who are at increased risk of complications resulting from COVID-19.
However, tele-neurology though it brings the world closer, it lacks the human touch and certain techniques of examinations are difficult to perform. It requires the doctor and the patient to be adept at modern technology and communication. The privacy, and confidentiality of patient data should be vigilantly maintained.
Tele-neurology has emerged during the times of COVID-19 and helped us deliver health care at times when social distancing was the norm. However, it has become an integral part of neurological evaluation and management that it is bound to fortify for the times to come as the COVID-19 fades into thin air. Updates and modifications to the existing guidelines shall be required as the practitioner faces newer challenges in delivering healthcare through tele-neurorehabilitation. The use of virtual reality in telerehabilitation can bring the healthcare professional and the patient together in the same virtual room augmenting the interaction.
Artificial intelligence (AI) pinpoints thyroid nodules noticed on thyroid ultrasound that are unlikely to be cancerous. The technology reduces a large number of unnecessary biopsies……Readmore
Simple App May Help Ease Insomnia
Treating insomnia becomes feasible without the use of medications as scientists design a new therapeutic app. Insomnia is a common and debilitating sleep disorder that can impact a person’s physical and mental health and wellbeing….Readmore
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
This month the National Medical Commission (nmc.org.in) has released the draft version 2 of the Telemedicine Practice Guidelines on its website. The version two is part of the new Professional Conduct regulation which will now be called National Medical Commission Registered Medical Practitioner (Professional Conduct) Regulations, 2022. Please click here to view and send your comments. The last date is 22nd June 2022. The telemedicine section specifically starts from Page 64 of this PDF document.
The important elements of the guidelines are well summarised by Bagmishika Puhan in this newsletter and makes an easy point of reference. I do hope TSI soon holds a consensus meeting to send in the comments.
Other than that we carry a piece on Speech and hearing from Dr. Vidya Ramkumar. An area of high impact where tele-practice has an important role.
Thank You Dr. Sunil Shroff
Chief Editor
President – TN Chapter – TSI
National Medical Commission Registered Medical Practitioner (Professional Conduct) Regulations, 2022. – Consultation Document
Bagmisikha Puhan Associate Partner, TMT Law Practice.
Siddhant Gupta Associate, TMT Law Practice
Preamble
Draft document for public consultation has been released this month by National Medical Commission (NMC) regarding Professional Conduct Regulations (2022) and includes Telemedicine Practice Guidelines Version 2 for Registered Medical Practitioner. This is likely to have far reaching changes in way doctors practice both physical and remote tele-consultations.
The disciplines of medicine and clinical practice have undergone a complete facelift, to cater to the marginalized and underprivileged populace, with telemedicine and teleconsultation measures. The issuance of the Telemedicine Practice Guidelines, 2020 (TPG) brought upon standardization and regulation of the telemedicine industry, a hitherto adverse proposition for the regulatory authorities.
Highlights of the Draft Regulation regarding Professional Conduct Regulations (2022) including Telemedicine Practice
The issuance of the National Medical Commission Registered Medical Practitioner (Professional Conduct) Regulations, 2022 (Draft Regulations) to update the erstwhile Indian Medical Council (Professional conduct, Etiquette and Ethics) Regulations, 2002 was essential, to update the regulations in view of the novel digitized modes of patient interaction and consultation.
Practice – The Draft Regulations specifically exclude RMP (under NMC) from practicing more than one system of medicine. RMPs are not allowed to practice another system of medicine simultaneously. The certificates so issued by an RMP must contain the details of the training, duration, skills/ competency, and the work done. The onus of establishing the veracity lies on the RMP.
Digitize Patient Records: In addition to impositions at the level of the healthcare institutions, every self-employed RMP must completely digitize patient records within 3 years from the date of publication of the regulations, in absolute compliance with the applicable laws of India and as per the proforma laid down by NMC.
Social Media: The Draft Regulations prescribe the key principles, behavioral obligations upon an RMP on social media. It is pertinent to note that the NMC Regulations do not prescribe any definition for “social media”, and we may be constrained to the definitions provided under IT Act and allied rules, to rely upon the definition of social media.
Training of RMPs: The Draft Regulations make considerable modifications to the TPG and prescribe Continuous Professional Development (CPD) training to RMPs desirous of conducting telemedicine practice in India; the earlier prescribed timeline of seeking a course certification within a period of 3 years from the date of notification of the TPG 2020, has been done away with. It now stresses on how the RMPs must familiarize themselves with the guidelines, as well as appreciate the shortcomings of the practice of telemedicine.
Establishing Relationship & Consent: The TPG now mandate an RMP to commence a consultation with provisioning an introduction [details of name, qualifications, area of specialty] and the location of their affiliate medical establishment. The Draft Regulations further require an RMP to obtain the patient signature or thumb impression with the date of the signature, on the informed consent document shared with the patient. Explicit consent must be recorded in any form – physical, audio, video, graphics, electronic, text – this must be stored by the RMPs. A template with respect to informed consent has also been provided within the draft regulations.
Follow Up Appointments: The specifics of a follow-up consultation have also been amended, wherein the patient may seek an appointment for a follow-up consultation after the expiration of 6 months, provided that the RMP has advised the patient to seek an appointment with him, between the period of 6-12 months from the date of the initial consultation. There is an additional leeway provided to the platforms for affording “follow-up consultations” to the same patient, where the newly assigned RMP / available RMP is comfortable in comprehending the patient’s medical condition after having been provided with adequate information (details of the condition and reports of all relevant investigations) by the patient. We see reliance being placed upon the professional judgment of the RMP who is available. The retention timelines for online consultation remains unchanged from what has been already prescribed for in-patient and out-patient records.
Duties of RMPs: The ethical considerations and duties imposed upon RMPs for practice of telemedicine specifically call out the primary RMP as the one responsible for the care and coordination of the patient, with the distant medical team/ professionals at 1.1.(2). The amended TPG clarify on the range of advisories which may be provided by an RMP during a tele-consult, and allow for advice on immunization, exercise, personal and household hygiene practices, mosquito control and so on.
At Annexure 3, the renewed TPG provide template that must be adhered to by the platform, as a patient information sheet. This includes the information which is already captured within the terms and conditions, and consent form (in some cases) of platforms which own, operate and manage teleconsultation platforms.
Prescription of Drugs: Further, the amended TPG now permit the RMP to prescribe any drugs, depending on the type of consultation, [with the exception of Schedule X drugs] during a tele-consult, basis their professional opinion and judgment.
Telemedicine service providers: The amended TPG now requires telemedicine service providers to establish protocols for referrals to emergency services, a hitherto unregulated aspect of clinical examination and practice in the erstwhile TPG. Further, RMPs must not participate in telemedicine platforms that provide ratings by patient or others including reviews, advertisements, and promotions of RMPs any means. As a consequence, it will become incumbent upon the digital platforms to remove such reviews, ratings that may be associated with a particular RMP listed on their platform.
The Draft Regulations do not merely require the platforms to conduct due diligence of the RMPs qualifications and registrations, but now specifically require that the onus of ensuring all the information regarding the RMP and all their qualifications that have been mentioned on their portal have been authenticated and are registered with the National Medical Register or their respective State Medical Councils is wholly placed on the owners and administrators of the technology platform.
Advertisement of Services: There is a clear embargo on advertisement of any RMPs, and promotion, including by means of manipulation of algorithms, search engines, etc.
Artificial Intelligence: The Draft Regulations reiterate that AI/ ML based counseling and prescription is not permissible; additionally, they clearly state that any correspondence in this regard with the patient shall be delivered directly by the RMP. The Draft Regulations continue to use the same template for prescriptions during online consultations.
Section that Lack Clarity – Unfortunately, the document still does not speak of interoperability, which has been spoken about since the first iteration of Electronic Health Records Standards were released in 2013, by MoHFW. We can only assume that the same is left to be determined by the Ayushman Bharat Digital Mission scheme.
Overall the current document is an improvement on the somewhat outdated Indian Medical Council (Professional conduct, Etiquette and Ethics) Regulations of 2002. All the stakeholders are invited to send their expert comments by 22rd June 2022 to National Medical Commission (www.nmc.org.in). The complete document is available on the site. Use this link to access the document-
Legal challenges with issuing prescriptions through teleconsultations
Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist Law Firm
Eshika Phadke Associate, Arogya Legal – Health Laws Specialist Law Firm
The ability of doctors to offer remote consultations has been legitimized after the notification of the Telemedicine Practice Guidelines, 2020 (“Telemedicine Guidelines”).
The Telemedicine Guidelines provide a framework for doctors on how to offer consultations: doctors are at liberty to select whether or not to consult via a teleconsultation, what mode of teleconsultation to adopt, whether to switch to another mode or in-person consultation midway, how to ensure that sufficient information is collected to arrive at a diagnosis (including ordering laboratory or diagnostic tests). After arriving at a diagnosis, doctors may even issue prescriptions to the patients.
On the same lines, the ability of a doctor to issue prescriptions is not unfettered: the Telemedicine Guidelines have categorised medicines that four broad categories – List O, List A, List B and the Prohibited List. Depending on the type and mode of consultation, doctors may issue prescriptions subject to the restrictions for that category. Non-adherence to the restrictions that have been specified for the lists would be treated as professional misconduct under the Indian Medical Council (Professional Conduct, Etiquette and Ethics) Regulations, 2002.
List O medicines can be prescribed following a first-time or follow-up consultation. These are the commonly prescribed drugs that are often over-the-counter drugs such as paracetamol. medications for coughs or common colds, supplements, etc.
List A medications can only be prescribed following a first-time consultation if it is a video consultation. These include ointments and lotions for skin ailments, local ophthalmological drops or ear drops, drugs used in psychiatric practice, etc. These are the drugs that typically require the doctor to undertake a visual inspection of the patient before arriving at a diagnosis as per standard treatment guidelines. Medications for chronic conditions such as diabetes, asthma and hypertension also fall under this list, provided that the diagnosis was made at an in-person consultation, and the doctor has last seen the patient regarding the same condition less than six months prior to the teleconsultation.
Doctors may prescribe re-fills of the same medication or add-ons for the ongoing treatment. The add-ons fall under List B.
The lists are not exhaustive, but indicate the rationale behind the categorisation so that doctors may apply it while issuing prescriptions. Doctors should bear in mind that they are ultimately responsible for the prescriptions, and they should err on the side of caution while issuing prescriptions. They should keep in mind the standard treatment guidelines for the condition while ascertaining what list a drug is likely to fall under and what mode of consultation would be appropriate. If any visual examination is required, a video consultation or in-person consultation should be requested. If a physical examination is typically necessary to arrive at a diagnosis, the doctor should not issue a prescription based on a teleconsultation. If a drug is to be administered only under medical supervision (such as injectables or abortion pills), a prescription cannot be issued to a patient directly, but may be issued during a consultation with another doctor or health worker. In some situations, a video consultation or in-person consultation may not seem necessary to a doctor, but the doctor should bear in mind that it is required under the law.
If a patient refuses to comply with the instructions given by the doctor regarding the mode of consultation, the doctor must record the non-cooperation in their notes and end the consultation without issuing a prescriXJption.
A violation of Telemedicine Guidelines at the hands of a doctor may amount to professional misconduct. Hence, it is paramount that prescription related decisions are based on sound medical and legal rationale.
References: Telemedicine Practice Guidelines, 2020 Frequently Asked Questions on Telemedicine Practice Guidelines
Understanding the implementation of telepractice in speech and language services for children and adults using a mixed-methods approach
Ms. Varsha Shankar
PhD Research Scholar, Department of Speech, Language and Hearing Sciences,
Sri Ramachandra Institute of Higher Education and Research (DU), Chennai – 600 116.
Email – varshashankar@sriramachandra.edu.in
Dr. Vidya Ramkumar DBT/Wellcome Trust India Alliance Intermediate Fellow in Clinical and Public Health Research Associate Professor, Department of Speech, Language and Hearing Sciences, Sri Ramachandra Institute of Higher Education and Research (DU), Chennai – 600 116. Email – vidya.ramkumar@sriramachandra.edu.in
Review of Telepractice in speech-language pathology (SLP) & Semi-structured interviews (SSI)
In recent years, telepractice in speech-language pathology (SLP) has emerged as a solution to overcome the challenges of access in the delivery of healthcare. Telepractice in SLP has been explored for over a decade, yet there is a significant knowledge gap with respect to factors influencing the implementation and sustaining telepractice. We aimed to identify implementation factors that influence the provision of telepractice in SLP services.
The current study consisted of a scoping review and semi-structured interviews (SSI). Articles that described telepractice in SLP were included if it was implemented for two or more years, providing screening, diagnostic or rehabilitative services to individuals of all age groups with speech and language difficulties across the world. Literature from January 2010 – April 2021 published in the English language were considered. Data from studies was extracted on: project description, geographical distribution, the focus area of service delivery, method and model of telepractice service delivery. Barriers and facilitators were identified and grouped under five domains identified from telemedicine implementation frameworks (technical aspects, organizational aspects, patient perspectives, economical aspects, and ethical legal aspects).
The SSIs were conducted for five authors who provided consent. Data was analysed using a hybrid method (Swain, 2018), which included
i) Deductive template of codes and themes derived from our scoping review and ii) Data-driven inductive approach that was carried out following data collection.
We then applied the principles of thematic analysis as described by Clarke & Braun (2012).
Data was extracted from 11 studies that were mapped to nine projects in telepractice in SLP.
Telepractice in SLP was implemented in five projects from the USA; two in Australia; and one each in Norway and Canada.
Five of the nine projects reported service delivery to be on-going or routine. The broad focus areas identified included diagnostics and evaluation, therapeutics and comprehensive assessment, management and follow-up care services. Synchronous/ real-time telepractice methods were always used for the provision of diagnostic testing or when providing therapy services using video conferencing. The ‘professional-facilitator-patient’ model was used most commonly followed by the ‘professional-patient’ model.
Barriers: for long-term sustainability included a. Inadequate initial capital investment, b. Lack of reimbursement and payment options, c. Low internet speed and bandwidth, d. Resistance and hesitancy to use telepractice from the patient’s end, e. Lack of organizational policies and uniform regulations. Organisational aspects had substantial influence on implementation.
Funding, administrative and infrastructure support were key elements that emerged as a part of organisational support from this study.
Findings of the study –
A. We found that telepractice services that received public-funding reported better sustainability. Availability of critical infrastructure such as internet also depends on political will of administrators.
B. Having a dedicated team of professionals and technicians with clear roles and responsibilities, and inclusion of systematic planning facilitated implementation.
Unique Proposition of the Study – The strength of the current study lies in the unique method of using a mixed-methods approach (combining a scoping review and semi-structured interviews) to get a deeper understanding of the barriers and facilitators influencing the provision of telepractice services in SLP.
Conclusion:
The findings from this study can guide the planning of future telepractice based services in SLP. Telepractice implementation research and reporting in the LMIC context is limited and no study fulfilled the inclusion criteria. Outcome reports from LMIC will be valuable considering the demand for such services in these regions.
In general, telepractice in SLP was not explicitly guided by implementation science or framework. The use of implementation frameworks ensures systematic planning and feasibility assessment to inform the scale-up of implementation. Therefore, it would be worthwhile for program implementers to consider these aspects when exploring telepractice services.
Full article Published in :Wellcome Open Research, 7, 46.
Telemedicine – News from India & Abroad
India
Unlocking the Power of Digital Health – Mansukh Mandaviya at Davos
Digital health is a great equaliser and enabler to support Universal Health Coverage and Sustainable Development Goals and can help ensure accessibility and affordability of health service delivery. India is implementing a national framework for digital health.
Under Ayushman Bharat (Long Live India) Digital Mission, India has embarked on digital transformation of healthcare in India. The focus is on creation of a longitudinal Electronic Health Record for more than 1.3 billion people of India. Health Minister Mandaviya said ‘We have already issued more than 220 million Unique Health IDs along with health facilities and provider registry’.
India also is utilising digital health interventions for its national program management. Reproductive & Child Healthcare IT platform tracks more than 120 million pregnant women for their ANC, PNC check-up, delivery planning and over 90 million children for immunization. Health Management Information system regularly collates data regarding health programmes from more than 200,000 health facilities.
PredictAI, a new machine-learning tool developed by researchers, speeds up the diagnosis of psoriatic arthritis (PsA) by up to 4 years, potentially preventing irreversible joint damage and deteriorating function for sufferers…..Readmore
New App Detects COVID by Hearing Sound of Cough
A new app, called ResApp, detects COVID-19 infection by just the sound of a cough. The app, which uses machine learning to analyze cough sounds, could detect Covid with 92 percent accuracy, Daily Mail reported……Readmore
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
In the April issue of the newsletter we have covered some interesting articles including one by Prof. K. Ganapathy on ‘Metaverse in Healthcare; that will eventually perhaps lead to you having a Metaverse Avatars visiting different virtual worlds.
Ayushman Bharat Digital Mission has invited Consultation Paper on creating Drug Registry for the country and the last date for such comment submission is midnight of 1st May. Please do spend some time by visiting the website and sending your valuable suggestion on this very important initiative.
The COVID numbers are again showing a rise, so we request our readers to continue wearing masks, practice hand wash and keep physical distancing. The course of the disease can still be unpredictable so do take your precautions.
Thank You Dr. Sunil Shroff Chief Editor President – TN Chapter – TSI
Consultation Paper on Drug Registry by Ayushman Bharat Digital Mission
Ayushman Bharat Digital Mission (ABDM) has been launched to create a national digital health ecosystem that supports universal health coverage in an efficient, accessible, inclusive, affordable, timely, and safe manner.
ABDM envisions open, interoperable, standards-based digital systems, and ensures the security, confidentiality, and privacy of health-related personal information.
Registries are one of the core building blocks of the ABDM which if standardized would help in enabling interoperability of healthcare data. These registries shall be designed with strong data governance mechanisms, adhering to the principles of verifiability, accessibility, and identity management.
One of the critical components of these registries is the Drug registry, which is envisioned to be a single, up to date, recognized registry of all the drugs. It is being conceptualized as the primary source of information for all other databases and lists and facilitates the exchange of standardized data across all systems of medicine, from allopathy to Ayurveda.
A central database of the approved drugs sold in the market will serve multiple benefits including free availability of verified information for all drugs, simplified regulatory flows, smoother supply chain management, streamlined insurance claim processing, innovations in clinical decisions, disease management and assurance models. Initially, the goal is to comprehensively capture relevant & accurate details of all drugs sold in India.
Over time, the drug registry is envisaged to help smoothen the inventory flow throughout the drug supply chain, improving the quality and patient trust and ultimately enabling patient centric digitization by ensuring machine readability of prescribed drugs. This document covers the strategic and technical design associated with the Drug Registry. The potential sources of input data, self-certification, verification, and data distribution flow have been proposed in the document to ensure the creation of a single nationally recognized source of truth for data on drugs that is trusted, digitally enabled, and widely adopted by the healthcare ecosystem stakeholders. We look forward to feedback and support from the ecosystem partners to enable the design and adoption of a Drug registry in India.
Written Comments on the Consultation Paper are invited from all the stakeholders by 11:59 pm of May 1, 2022.
The comments may also be sent on the email ID: abdm@nha.go National Health Authority Tower 1, Jeevan Bharati Building, Connaught Place, New Delhi – 110001.
Webinars on Digital Health and its Future
Prof. K. Ganapathy
Past President, Telemedicine Society of India & Neurological Society of India | Hon Distinguished Professor The Tamilnadu Dr. MGR Medical University | Emeritus Professor, National Academy of Medical Sciences | Formerly Adjunct Professor IIT Madras & Anna University | Director Apollo Telemedicine Networking Foundation & Apollo Tele Health Services | URL: www.kganapathy.in
On Thursday 24th March 2022 the Tamilnadu Chapter of the Telemedicine Society of India joined hands with PALS as co-organisers to promote a two webinars on
1. Role of technology in enabling Digital Health
2. Role of Technology in Health Care in 2030 – A peep into the future.
This 2 hour interactive session was conducted by Prof. K. Ganapathy Past President TSI.
The webinars were conducted on 24th March 2022 and it marked the 22nd anniversary of the formal commissioning of the world’s first VSAT enabled village hospital @ Aragonda the birth place of Dr Prathap C Reddy Founder Chairman of the Apollo Hospitals Group. To commemorate this a global webinar was held. The recorded proceedings are available @ https://youtu.be/eG2yj1pBkjU or https://bit.ly/3vLc257
The contents were customised specifically for students and faculty of Engineering Colleges.
The Metaverse is slowly becoming an interesting and popular topic. On 6th March 2022 the Chennai Chapter of the COMPUTER SOCIETY OF INDIA had a 2 hour session on The Metaverse. This included a talk on “Role of the Metaverse in Healthcare” by Prof. K. Ganapathy Advisor to the Tamilnadu Chapter of the TSI. Dr Ganapathy defined the Metaverse as the augmented Virtual World derived by convergence of virtual and physical space, where users can interact within the augmented world, to meet each other virtually, immersing themselves in performing virtual activities that gives real experiences. The untapped potential in healthcare to combine AI, Virtual Reality, Augmented VR, Extended VR, Internet of Medical Things , Web 3.0, I Cloud, Edge, Quantum Computing and Robotics was illustrated.
On 2nd April 2022 Innovaspace, GAPIO ( Global Association of Physicians of Indian Origin ) and Apollo Telemedikcine Networking Foundation jointly organized an international webinar on Role of the Metaverse in Healthcare. The speakers included Dr Shabbir Sayeed Abdul Professor of AI & Digital Health, Taipei and Mr Silviu Pervu CTO Various Deep Tech Companies, London, besides Dr Ganapathy. Interestingly there were more attendees from other countries than India !! The talks are available @ https://bit.ly/3seWx4P
Decoding the Healthcare Professional Registry’s Utility in Telemedicine
Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist Law Firm
Eshika Phadke
Associate, Arogya Legal – Health Laws Specialist Law Firm
Saloni Kedia
Associate, Arogya Legal – Health Laws Specialist Law Firm
The Ayushman Bharat Digital Mission (ABDM) was launched in 2020 with the vision of creating “a national digital health ecosystem that supports universal health coverage” and “establishing registries at the appropriate level to create a single source of truth in respect of clinical establishments, healthcare professionals, health workers, drugs and pharmacies”.
To streamline the flow of health data, the ABDM also envisages four electronic registries: the Ayushman Bharat Health Account (ABHA), the Healthcare Professionals Registry (HPR), the Health Facility Registry (HFR), and the Drug Registry. The ABHA is a unique identification number that will be assigned to each individual patient, and enables them to digitise their health records and make it available to healthcare professionals. The HPR will be a registry of all doctors, nurses, allied and healthcare professionals, paramedical staff, ASHAs, etc across both the modern and traditional systems of medicine. The HFR will serve as a directory of all public and private hospitals, clinics, diagnostic centres, pharmacies, etc. The Drug Registry will be a database of all drugs from all systems of medicine that are approved in India.
Recognising the role that telemedicine plays in the realisation of the vision, the ABDM also places a strong emphasis on creating an open telemedicine network, which will consist of a government owned, operated and managed system at the back-end, and privately owned and operated consumer apps at the front-end which operate on the data contained in the four registries. In this article, we will focus specifically on the HPR, and its significance in telemedicine.
Doctors are familiar with the rolls that are maintained by the National Medical Commission and the all the state medical councils – the HPR is essentially a larger scale version of the list, which will include all professionals involved in the healthcare delivery system, and will enable registered professionals to be connected to the ecosystem. Doctors may elect to enrol with the HPR and, upon verification by the respective medical council, they will be given access to the account and will be assigned a Healthcare Professional ID. For a professional providing teleconsultation, there are several advantages to being enrolled in the HPR.
First, a profile on the platform will be generated which will contain the doctor’s name, specialisation, educational background, availability, etc. As there is no law that explicitly recognizes the right of the doctors to be listed on the private aggregator platforms, the creation of a profile under the government-led HPR will provide online visibility to the doctor without there being any apprehension of violation of law.
Second, as per the Telemedicine Guidelines, doctors providing teleconsultations are required to establish a mechanism whereby patients can verify the doctor’s credentials and contact details. Thus, even when a doctor is providing consultations via phone calls, he/she can lead the patient to their public profile on the HPR, which will serve as a credible source for verification.
Third, the ecosystem will enable doctors to digitise their in-clinic practice and adopt paperless diagnostic reports, discharge summaries, prescriptions, etc which can be e-signed. This will provide for a seamless hybrid practice where the doctor can consult patients both in-clinic and through a teleconsultation, as per the patient’s convenience, without having to assume additional difficulties with documentation and accessing records.
Fourth, the doctor will have access to all the historic records of patients who have opted for the ABHA scheme and consented to have their data shared. This will reduce the dependence on the patient to furnish their records to enable the doctor to gain a holistic understanding of the patient’s condition prior to proceeding with a diagnosis and treatment plan. As per Telemedicine Guidelines, doctors are required to ensure that they have all the information required as per standard treatment guidelines before proceeding with a treatment plan for a patient. Access to past records will help doctors meet this requirement.
Finally, the drug registry (once operationalised) will offer access to a single, up-to-date, centralized repository of all the drugs across all systems of medicine which are approved and are available in the Indian market, which will provide a treasure trove of information that will help doctors while issuing prescriptions.
The implementation of the digital health ecosystem is presently still at a primitive stage, and the full potential of it is yet to be realised. That being said, it is clear that it will prove highly advantageous for doctors who are looking to take or grow their online practice. Thus, while enrolment with the HPR is voluntary, it may be a pragmatic step to take for doctors who offer teleconsultation.
Telemedicine Practice Guidelines (Accessible here)
TELEMEDICINE IN INDIA: A CRITICAL ANALYSIS OF THE EXISTING LEGAL FRAMEWORK – A Summary
Dr. Karan Shekar MBBS, PGDMLE (NLSIU)
Resident, Department of Cardiothoracic Surgery, Narayana Health, Bangalore.
Contact: +91-9108158715/+91-9110622903,Email ID: drkaranshekar@gmail.com
Dr. Arpita H.C,
Assistant Professor,Centre for Health Law and Ethics,
National Law School of India University,Bengaluru. Email ID: arpithahc@nls.ac.in
Introduction:
Healthcare sector is an 8.6 trillion dollar industry having major economic influence in our developing country. However, India still ranks 145th out of 195 countries in terms of quality and accessibility of healthcare. The calling of WHO for “Universal Health Coverage – Health for everyone, everywhere” has a huge potential to be realized through the recent implementation of Telemedicine in India. The author in this paper attempts to summarize the Critical analysis of telemedicine guidelines article from UPES Law review: Vol. VI 2021, ISBN 2347-9620; which dwells on effective regulatory Framework for Telemedicine implementation.
Telemedicine has existed since decades. From the early 1990s, due to a rapid rise in the usage of the internet brought about a huge dependence on telemedicine for immediate healthcare assistance and has been utilized, however without legal framework. In different countries practicing telemedicine, there were hardly any standards for medical practitioners to follow and patients to expect during a teleconsultation process. Issues such as personal data privacy, security, lack of a legally accepted prescription, lack of doctor credentialing, and liabilities, standard operating protocols, malpractice and negligence, duty of care were paramount. Without addressing them with statutory guidelines, it was impractical to implement the practice of telemedicine to serve the country’s healthcare needs.
During the peak of COVID pandemic, much to the relief of many healthcare professionals, the Ministry of Health and Family Welfare in partnership with NITI Aayog released the “Telemedicine Practice Guidelines” which therefore legalized the practice. The guidelines are patient-friendly but comprehensive and cater to the interests of all the concerned stakeholders, including the RMP, patient, and technology and cuts across all digital platforms
Critical Analysis of the guidelines:
Cross jurisdictional Consultations:
Having provided different opinions regarding the practice of medicine among different states as observed by the high court in two separate occasions12 puts the guidelines in ambiguity regarding the inter-state practice of telemedicine.
Registration of Complaints:
The ambiguity as to where to register a complaint would bother all three parties i.e. The RMP, the patient and the telemedicine provider. If the patient wishes to register a complaint against a doctor for negligence, there is no clear guideline as to where should the patient place the complaint. Would the complaint be taken up at the location where the patient resides or whether it is at the doctor’s location or is it at the location from where the telemedical platform operates?
Patient confidentiality and Data privacy:
The guidelines are clear that the patient may use any platform to connect with the doctor for a teleconsultation. It mentions the use of WhatsApp, Facebook messenger, Google Hangouts, Skype, email, fax, etc. However, due to lack of contract between parties providing such mediums and the healthcare practitioner, there is high chance of data breach with sensitive medical information.
Incorporation of these guidelines into public healthcare:
Ensuring that the benefit of telemedicine reaches the corners, institutional incorporation is necessary.
Research and Evaluation:
As practitioners of modern medicine, RMPs believe in evidence-based medicine. The novel clinical practice is cost-effective and convenient. Yet, it must also be proved to be safe, efficient, based on empirical, unprejudiced, and convincing evidence.
Recommendations to the guidelines:
Institution of a regulatory authority:
Establishing a competent, independent authority to oversee the process of telemedicine in general digital health is essential. A pre-existing competent authority such as Telemedicine society may overlook the needs and demands of this novel practice.
Institutional incorporation:
Telemedicine should be a department of its own in all government primary health centers, community health centers, and tertiary care hospitals.
Telemedicine in healthcare curriculum:
Medical schools and nursing schools should develop comprehensive telehealth curricula, including lecture series, clinical clerkships, and rotations.
Licensure to practice telemedicine:
Teleconsultants should be verified by a single authority undergoing uniform training, and certification process for the practice. They must be allowed practice without cross-border jurisdiction which creates an obstacle in delivering teleconsultations.
Accreditation and audit:
A competent authority can ensure access, affordability, efficiency, quality and effectiveness of the practice of telemedicine. Regular audits and certification stimulates continuous improvement within the organization. This too, can be overseen by the Telemedicine society.
Insurance coverage:
All insurance companies, government, and private must recognize and acknowledge telemedicine and adopt policies emphasizing telemedical care for ease of healthcare access to the public.
Technical aspects:
A separate technology department with a sole focus on tele-medical services for data privacy and protection needs to be instituted.
Research in Telemedicine:
Enabling research and funding for research to advance implementation, resource utilization, identify populations with increased healthcare demands, quality improvement, and clinical outcomes.
Furthering telemedicine:
Exploring opportunities for utilizing telemedicine by forming partnerships with interdepartments or centers of telemedicine to increase access to expert clinical advice from specialist doctors.
Public awareness:
Ministry of health associated with its healthcare functionaries to promote and educate people to embrace telemedicine for all primary consultations and to minimize visits to hospitals.
*Complete Article is available at UPES Law review: “Telemedicine in India: A critical analysis of the existing legal framework.” Vol. VI 2021, ISBN 2347-9620
Artificial Intelligence (AI) Helps Detect Cancer from Patient Data Securely
Researchers developed a novel way of using artificial intelligence (AI) to predict cancer from patient data without putting personal information at risk…..Readmore
Robots may Now Mimic Humans in Performing Tasks
Robots can now adapt to their working methods to solve complex tasks — similar to humans as per a study at the Chalmers University of Technology, Sweden, presented at the robot conference IROS 2021……Readmore
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
This March 2002 issue of the Telehealth newsletter has an important contribution about the role of digital signatures for e-prescription from Mr. Anay Shukla and Ms. Saloni Kedia.
The current Telemedicine Practice Guidelines on e-prescriptions mentions that they can be dispensed in the form of a photo, scan, or digital copy via email or any messaging platform to the patient. A photo, scan or digital copy of a prescription, is technically only a copy of the prescription, and not the original prescription. If we apply the requirements of the IT Act to e-prescriptions, it should have digital signature to be valid and to ensure that they are not misused. The Information Technology Act (IT Act) of 2000 gave digital signatures the same legal recognition as handwritten ones. Therefore, as a practice, while offering teleconsultations and issuing e-prescriptions, it may be prudent to use a digital signature to authenticate the e-prescription.
Continuing our articles on Tele-ICU, this issue brings a nursing perspective of tele-ICU care from Saudi Arabia. The last piece is the integration of Ayushman Bharat Digital Mission with Hospital Management system of SHER-I-KASHMIR INSTITUTE OF MEDICAL SCIENCES (SKIMS). This is an important step in digitising the health care system in this large govt. hospital in Srinagar and hopes to improve overall care and bring efficiency.
We do require more contributions from members, do remember documenting your work helps in ensuring that there is a point of reference for others and also creates visibility about your work.
Do remember that on the 7th April, we will be celebrating the World Health Day. Do celebrate with a tele-health activity. The theme this year is ‘Our Planet our Health’. The COVID pandemic has made us realise how interconnected we are. And the only way to ensure health access to all is through Tele-health.
Thank You Dr. Sunil Shroff Chief Editor President – TN Chapter – TSI
Prescriptions and Digital Signatures
Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist Law Firm
Saloni Kedia
Associate, Arogya Legal – Health Laws Specialist Law Firm
Digital signatures have been legally recognised in India for more than two decades now. The Information Technology Act (IT Act) of 2000 gave digital signatures the same legal recognition as handwritten ones. In course of offering tele-consultation over the internet, registered medical practitioners (RMP) routinely issue prescriptions in digital format (hereinafter referred to as “e-prescriptions”).
Under Indian law, in order for a prescription to be valid, it must carry signature of the RMP. This requirement is easily met for physical prescriptions. However, in context of e-prescriptions, it is unclear whether scan or photo of physical prescription meets the threshold of a valid prescription, or whether an electronic signature is required to be affixed in an e-prescription, or whether a digital signature is required to be affixed in an e-prescription, in order to ensure that the e-prescription generated by the RMP is lawful and valid.
The IT Act provides that, if any law requires any information to be validated by affixing a signature of any person, then such requirement is deemed to have been satisfied if the information is authenticated by means of a digital signature affixed in the manner provided by the Central Government. Thus, because of the IT Act, e-prescriptions have the same legal recognition in India as physical prescription, provided they are affixed with a digital signature.
Under the IT Act, “digital signature” is a signature which is supported Digital Signature Certificate (DSC). A DSC is a secured digital key provided by certifying authority to validate and confirm the identity of the person who holds the certificate. A DSC includes information such as the user’s name, pin code, country, email address, certificate issue date, and name of the certifying authority. The certifying authority provides three different classes of DSCs i.e. Class1, Class 2 and Class 3. The fundamental difference between the three classes is the level of validation of the subscriber (i.e. author) of the digital signature that has been undertaken by the certifying authority. Under Class 1 DSC, the authority does not undertake verification of the identity of the subscriber through video verification. Under Class 2 DSC, the authority requires the subscriber to prove his or her identity through video verification, but without remaining physically present before the authority. Under Class 3 DSC, the authority requires the subscriber to be physically present before it in order to ascertain the identity of the subscriber.
In most common use scenarios, including for the purpose of issuance of e-prescription, a Class 2 DSC should suffice.
It should be noted, however, that there is an apparent contradiction with respect to validity of e-prescription in the Telemedicine Practice Guidelines, 2020 (TPG). The TPG provides that e-prescriptions can be dispensed in the form of a photo, scan, or digital copy via email or any messaging platform to the patient. A photo, scan or digital copy of a prescription, is a copy of the prescription, and not the original prescription. Therefore, as a practice, while offering teleconsultations and issuing e-prescriptions, it may be prudent to adopt a Class 2 DSC to authenticate the e-prescription.
Tele–ICU and Tele-ICU Nursing
Mr. Ajo Jose RN Head Nurse, Tele-ICU Riyadh, KSA
Tele-ICU is a diagnosis and treatment method that makes use of videoconferencing and internet technology to provide intensive care services to patients in a remote or a location where there is shortage of intensive care doctors. It makes it possible for patients and critical care specialists in the ICU to be face-to face within seconds with high risk patients to receive medical care easily and quickly.
Most tele-ICU programs have a command center that are staffed with highly trained intensive care doctors and critical care nurses who aid patients electronically either with the help of audio connections or videoconferencing. This allows healthcare professionals to get patient data in real-time and resolve issues as soon as they arise.
Intensivists are generally very experienced in diagnosing how critical a patient’s condition is, which is helped greatly by access to vital information that is provided through the technology used in tele-ICU equipment. This helps dramatically reduce ICU complications. They are also extremely well-versed and experienced in different kinds of critical care areas that extend to pediatric critical care or pulmonary critical care.
Tele-ICU solutions can also reduce the cost of providing healthcare to those in acute need of care where there is no access to tertiary care due to lack of experienced intensivist. Providing this service also gives an additional revenue stream for the remote hospital. Overall tele-ICU care is a win-win for all be it the hospitals, doctors and patients. During the COVID pandemic tele-ICU saved millions of patients in all parts of the world and has grown exponentially.
What’s is the role of a Nurses in Tele–ICU? From my experience I can define Tele- ICU Nursing as a combination of informatics nursing and critical care nursing. Telehealth nursing is a method of delivering care remotely through the use of technology, including mobile devices, tablets, and computers. Sophisticated telehealth encompasses more than digital appointment reminders and confirmations—it is a way to offer real healthcare assistance and support from a distance. Let’s look what are the Nursing Jobs can do from Tele-ICU Command center. Essentially a tele-ICU nurse can lessen the burden of a critical care doctor by performing certain task and constantly monitoring patients.
Triage: usually we consider all the ICU Patients are critical patients however there are some more critical than others. Triage of patients from most sick to less sick is defined by certain para-meters. Patients who are very sick require more close monitoring and more coordination with the doctors both at the command and remote center.
Patient Family Education: Basically all the Tele-ICU Nurses are well experienced nurses in critical care nursing. They have good knowledge about what happens in the ICU. Tele-ICU Nurses can conduct regular virtual conference with family members and explain about the procedures, medication being given, the ICU equipment and why they are used and the patient’s conditions. This helps the Tele-ICU specialist to devote more timein decision making and look after more patients.
Quality Monitoring: tele-ICU is always connected with remote ICU Medical record (EMR). Most of the Tele-ICU in the world use advanced HIS system which will shows the documentation of multi-disciplinary team. Tele-ICU Nurses can be trained to perform regular audits on these documents. In the long term this helps with standardize care, evolve protocols and improve care. This would help with the documentation for accreditation requirements ( Eg, NABH or JCI) for the hospital.
Monitoring and Reporting of Key Performance Indicator (KPI): ICU KPI is a well-defined performance measure that is used to observe, analyze, optimize and transform a health process. Tele-ICU Nurses can maintain statistical data of their remote ICU on daily basis, statistics includes total admissions, discharge, and average length of stay, occupancy rate, infection and mortality. All these reflect the performance of ICU and how Tele-ICU is effective. This again would help with the accreditation requirements ( Eg, NABH or JCI) for the hospital.
The above mentioned points are some of the daily routine jobs for a Tele-ICU Nurse however there are others many like updating live census, supply chain coordination between remote Projects and many others.
Tele nursing is growing along with telemedicine. Telehealth eases the impact of the nursing shortage because it provides easier access to professionals for patients.
SHER-I-KASHMIR INSTITUTE OF MEDICAL SCIENCES (SKIMS) Integrated with Ayushman Bharat Digital Mission
SKIMS in Srinagar integrated its Hospital Information System with Ayushman Bharat Digital Mission (ABDM). It is a major step towards digitized and integrated healthcare services and will benefit general public to draw benefit of healthcare facilities in a seamless digital manner.
On the occasion SKIMS also signed MOU with J&K Bank for starting online payment system which is seen as another big step towards digitization for better patient care.
Shri. Vivek Bhardwaj (IAS), Additional Chief Secretary, Health & Medical Education who was Chief Guest on the occasion lauded the SKIMS for its robust Health Information System and said the integration of SKIMS HIS with Ayushman Bharat Digital Mission will mark a new beginning and the SKIMS will become a role model for the entire country. He emphasized the digital revolution in various aspects of life is making huge strides to ease our lives.
Director SKIMS/ EOSG Prof. Parvaiz A Koul in his address said that integration of existing HIS at SKIMS with Ayushman Bharat Digital Mission as part of Digital India Program will undoubtedly make healthcare delivery services easy and more accessible. Professor Koul while dispelling the apprehensions about digital health records said it is absolutely safe and protects privacy of the patient and will enhance efficiency of the healthcare system. He congratulated IT team SKIMS for their services and developing sound Hospital Information System which he said is one of its kind in the country.
He further added that SKIMS will soon have fully cashless transaction system and thanked J&K Bank for their constant support. He said signing of MoU with the J&K bank on this platform is the final step towards it.
Mr. Syed Shafat Hussain Rufai, Zonal Head Kashmir Central, J&K Bank who was present on the occasion assured full support and said J&K Bank will facilitate SKIMS at every step for better patient care delivery.
Mr. Farooq Ahmad Wani, Superintendent Engineer IT & Electronic Communications SKIMS highlighted the role of IT systems in SKIMS and said the department has come a long way in making system robust and efficient through IT solutions. He acknowledged the role of IT professionals in SKIMS which he said are working at multiple levels and strengthening healthcare services at SKIMS.
Dean Medical Faculty Prof. Tariq A Gojwari, Mohd Yaseen Choudhary (IAS) Mission Director, National Health Mission J&K, Medical Superintendent SKIMS Dr. Farooq A Jan , Nodal officer Ayushman Bharat Dr. G.H Yatoo and Assistant Professor Ms. Samina Mufti also spoke on the occasion.
Issued through, PR Office SKIMS
Tripura tribal council inks deal with Apollo Hospitals for tele-medicine services
ADC executive member Kamal Kalai said, “This agreement will provide tele-medicine, tele-consultation and tele-emergency services; a tele-ICU facility administered by experts; and ambulatory services by Apollo specialists during health camps or outreach initiatives in far-flung areas. This is the first phase of our cooperation and understanding”, Kalai said.
The Tripura Tribal Areas Autonomous District Council (TTAADC) has signed a memorandum of understanding (MoU) with Apollo Hospitals to set up tele-medicine services at the tribal council-run Kherengbar Hospital at Khumulwng, 25 km from Agartala.
Speaking to IndianExpress.com, Tripura ADC executive member Kamal Kalai on Friday said the MoU was partially signed by Apollo Hospital authorities in February, when a team of the ADC visited Hyderabad. However, the TTAADC chief executive office, who was in Uttar Pradesh as the Returning Officer for the Assembly elections, returned recently and completed the MoU signing yesterday.
“This agreement will provide tele-medicine, tele-consultation and tele-emergency services; a tele-ICU facility administered by experts; and ambulatory services by Apollo specialists during health camps or outreach initiatives in far-flung areas. This is the first phase of our cooperation and understanding”, Kalai said.
Kalai also said doctors and nurses from Kherengbar Hospital will be trained in Hyderabad to learn to coordinate in virtual mode while offering treatment.
He also said Apollo is in discussion with ADC authorities to set up a unit of the hospital at a later stage in Khumulwng.
Since royal scion Pradyot Kishore Manikya Debbarma-led TIPRA Motha’s assumed power in the state’s tribal council last year, the ADC has been trying to develop its public healthcare infrastructure, including equipping Kherengbar Hospital and different healthcare installations with oxygen concentrators and other modern healthcare facilities.
“This MoU would give the ADC a special opportunity to acquire advanced medical services, especially in far-flung rural areas,” the ADC executive member said.
Tripura Chief Minister Biplab Kumar Deb inaugurated a 150 LPM oxygen plant at Khumulwng last year as part of the state government’s initiatives to build healthcare infrastructure amid the Covid-19 pandemic. The state government also announced Rs 30 crore to ensure quality public healthcare for the tribals living in the ADC areas.
One-third of Tripura’s 37 lakh population are from 18 tribal communities. Most of them live in the TTAADC, which is spread across 7,132.56 square km and covers nearly 68 per cent of the state’s geographical area…Readmore
By utilizing artificial intelligence (AI) and robotics, Rutgers researchers have stabilized an enzyme that can degrade scar tissue resulting from spinal cord injuries and promote tissue regeneration…..Readmore
Artificial Intelligence Shows Promise in Cancer Diagnosis
Scientists have explored the use of artificial intelligence (AI), deep learning (DL), and machine learning (ML) to enhance the precision and predictive power of cancer biomarkers…..Readmore
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
This issue contains two important reports about the remarkable progress.made with Tele-ICU care during the ongoing pandemic. Tele-ICU is the best example of telemedicine not only saving lives but also making access to acute care possible in remote locations at an affordable cost.
The average cost of care is atleast 50 to 60% less than the cost of care in a tertiary set up. However there are some challenges with the tele-ICU care as the current telemedicine guidelines falls somewhat short for this type of care and require more clarity on the regulations in areas such as the consent process and also provide a list of life saving medications that can be administered by remote trained health care workers (not RMPs) under the instructions of the ICU specialists. This empowerment will truly benefit the telemedicine ecosystem and the large rural population of the country.
Thank You Dr. Sunil Shroff Chief Editor President – TN Chapter – TSI
Technology Transformation of Critical Care
Dr. Dhruv Joshi, M.D. ABIM (Pulmonary, Critical Care, Internal Medicine) CEO & Co-Founder, Cloudphysician
Introduction
Cloudphysician is a healthcare delivery company that leverages technology to provide access to high-quality critical care to hospitals across the country using technology. Shortage of trained medical personnel and gaps in the delivery of high-quality critical care are a universal problem. Cloudphysician’s Care Center in Bengaluru is staffed 24/7 with a highly qualified and trained critical care team that includes trained intensivists, critical care nurses, pharmacologists and dieticians. The multidisciplinary clinical team uses RADAR, their smart ICU platform, to connect to hospital bedside teams in ICUs to oversee and manage the care of critically ill patients across multiple regions.
RADAR incorporates automation, communication, real time video, data analytics and AI/ML to help expert care providers connect to and improve the quality of care for patients.
Success stories
Hospitals served by Cloudphysician’s highly specialized team have seen an improvement in quality of care. For instance, a multispeciality hospital in North India collaborated with Cloudphysician to manage their patients. The hospital had a high patient intake and were facing difficulties with nighttime patient care. Cloudphysician tele-critical care team worked hand in hand with consultants and nurses at the hospital to provide quality and evidence based care. Availability of an intensivist 24/7, proactive monitoring and institution of quality protocols with respect to antibiotic usage, infection control practices and hand hygiene led to an improvement in patient outcomes including reduction of ICU mortality rate by half.
In another example at a multispeciality hospital in a tier 2 city in South India, an elderly woman was admitted with an altered level of consciousness. Her work of breathing (WOB) was very high, and she was immediately intubated and shifted to the ICU. An incorrectly placed endotracheal tube led to a collapsed left lung. The vigilant eye of the tele-critical care team immediately asked for an X-ray and picked up the incorrectly located tube, following which the intensivist immediately guided the hospital team to reposition the tube and re-expand the lung. Within 30 minutes of corrective actions the vital functions returned to normal. The collaborative effort saved the patient’s life who went on to make a full recovery.
National presence
Across 15 states in India, Cloudphysician has taken care of over 30,000 patients in critical care settings. To date, we have successfully equipped healthcare providers with advanced adult critical care support in not just multi-specialty hospitals but also medical and surgical focused single-specialty hospitals. The model is designed for easy adoption even in resource-constrained settings. We have collaborated with over 65 hospitals serving over 1000 ICU beds ranging from community hospitals in tier 1 cities like Bengaluru and Mumbai to hospitals in remote areas of Assam. The solution includes extensive upskilling and training programs. The clinical teams at our partner hospitals undergo regular upskilling programs allowing them to manage more complex critically ill patients and ensures better patient outcomes.
The model has resulted in the creation of centers of critical care excellence, where the partner hospitals have been able to serve the communities, reducing the need for patients to be transferred to other locations and making quality care more accessible for patients and their families. The 24/7 intensivist led vigilance and evidence-based treatment plans allow peace of mind for the hospital consultants and specialists. Overall, a reduction in medical errors was observed; better and faster response to emergencies and better implementation of protocols that are appropriate to the setting were seen.
Cloudphysician had onboarded 14 hospitals during the first and second wave of COVID-19 pandemic in India managing over 400 ICU beds. We have been a proud recipient of CAWACH grant from the Department of Science and Technology, GoI, for supporting COVID-19 response. We were also the finalists at Ayushman Bharat startup challenge and Market Access Program. For connecting COVID-positive ICUs during the second wave in India, we were felicitated by the Government of Maharashtra and the Maharashtra State Innovation Society.
About the author:
Dr. Dhruv Joshi is the co-founder and CEO of Cloudphysician. He trained in Pulmonary and Critical Care at the Cleveland Clinic Foundation, USA.
eACCESS : Surfing the stormy waves of the pandemic
Dr. Sai Praveen Haranath MBBS,MPH,FCCP American Board Certified in Internal Medicine, Pulmonary and Critical Care Medicine Senior Consultant Pulmonologist & Critical Care Specialist Medical Director, Apollo eACCESS TeleICU Service, Apollo Hospitals, Jubilee Hills, Hyderabad, India.
The eACCESS program (Apollo Electronic Critical Care and Emergency Services) at Apollo Hospitals has been managing critically ill patients remotely for several years. During the COVID pandemic a rapid pivot was made to assist in COVID triage, monitoring and treatment of patients who were positive for the SARS-COv2 infection.
Patients all over India were evaluated for COVID symptoms using the same national consensus protocol to manage our bedside patients within the hospital group. Over 50 versions of the treatment plan were used as the evidence and science of COVID care evolved. Remote sites benefited from the advances instantly and knowledge sharing and transfer was immediate. While the eACCESS program managed traditional ICU patients, during COVID many new innovations were designed and tested. The ecosystem had the support and guidance of upper management and allowed the group to function in a nimble manner despite being a part of a large corporate hospital group with multiple stakeholders and processes.
There were three key areas that we focused on which allowed the concept of tele-ICU care to become socialized and accepted even in areas that had rudimentary critical care.
1. Education on critical care principles 2. Management of the spectrum of respiratory failure 3. Advanced consultation with coordination of escalation in care
Education of external non-Apollo remote sites as well as internal sites has been ongoing since the evolution of the tele-critical care program. During COVID this took on an urgency due to the rapid change in treatment protocols. Large public sector units required remote guidance for COVID triage and care. On a national scale we coordinated with the different units of Apollo Hospitals Group including remote care, bedside care, paramedics, lab services and information technology . Using this process we had regular didactic as well as on the job training of nurses, junior doctors and ancillary personnel located in over 27 locations around India.
Almost 17,000 tele-critical care patients have been managed in one external hospital group alone. Internal monitoring of isolated COVID patients was also done for our own hospital system .The acuity of illness as expected fluctuated with the waves of the pandemic. Respiratory failure was widespread but many patients only required oxygen and titration of treatment based on oxygen saturation was made. Likewise evaluation of cause of hypoxia especially related to the possibility of coagulopathy was also done using point of care diagnostics. High flow oxygen titration, non-invasive ventilator initiation as well as adjustment of invasive ventilators were managed remotely. Using high fidelity cameras ventilator waveform troubleshooting was routinely done. Direct interaction with registered medical practitioners and nurses at the bedside has been an integral part of the process.
There were many remote sites with complex respiratory failure including ARDS with septic shock who had no prior experience handling such sick patients. Ad hoc rapid connectivity was established and triage for ECMO as well as stabilization prior to transfer was arranged. Several centres around India were able to save patients with expert help in evidence based critical care and standard of care measures. Many referrals were initiated by patient relatives themselves and eACCESS teams would contact the bedside providers for permission to virtually manage their patients in coordination with the existing team. Fortunately all locations were open to coordination and communication.
I bring up this point because the key to a successful tele-critical care program is open communication and redundant systems. In a traditional business development process there was a linear approach where remote sites or our program would discuss the feasibility and need for remote critical care. This required a certain amount of education and awareness at both sides. Remote doctors who were often the owners of the hospitals needed to see value that was financial as well as adding to the services provided from their site. Our program likewise had to understand the niche needs of each center and communicate this effectively.
The latest in this progressive remote care process has been the desire to reach out to as many smaller sites as possible to begin a process of improved equity in critical care access. With this in mind we have enrolled over 180 hospitals nationally with a comprehensive care model where critical care is one part of this engagement. Covering over 600 ICU beds the model seeks to be inclusive as well as cost efficient. The definition of critical care may need to change as patients may need intensive care anywhere, anytime. Using remote technology as well as a user friendly intuitive electronic medical record, we are now able to deliver world class care.
Our current focus is on standardization of care protocols and incorporating into workflows. We are also actively evaluating our outcomes and processes and trying to share our learnings through publications and other venues. The core value of delivering exceptional care to everyone is possible with remote care and especially remote critical care when lives are truly at stake. Doing this with empathy is an art and a skill that will be great to disseminate widely as the need is immense and immediate.
Reports By – Ms. Harshini & Ms. Sumithra Lead Program Managers,
Indian Institute of Technology Madras, Healthcare Technology Innovation Centre Email – impact@htic.iitm.ac.in
The HTIC Healthcare Conclave is conducted once in every quarter. The aim of this series is to bring successful entrepreneurs, Technical and Business experts from different domains under health care to share insights and to discuss the upcoming trends, Innovation, technologies, and bottlenecks. The conclave brings best minds in the medical and healthcare industry, to share the progress and the challenges in the different sectors.
The January 2022 conclave was conducted in collaboration with TSI – TN chapter, comprised of two panel discussions, two expert sessions and start-ups demonstrations in Tele Health. (see poster below)
A Keynote Address was delivered by Dr V Mohan, Chairman, Dr Mohan’s Diabetes Specialities Centre & Director, Madras Diabetes Research Foundation, Padma Shri Awardee in which he gave an overview on the Role of Telemedicine in Diabetes. The next part of the session included Panel Discussion on the topic Telehealth – Practitioner’s perspective and Patient experiences where we had diverse set of speakers from doctors to Startups, chaired by Dr T. Senthil, Founder & CEO, Welcare Health Systems Pvt Ltd. The panellists included Prof. K.Ganapathy, Member of Board of Directors. Apollo Telemedicine Networking Foundation & Apollo Telehealth Services, Dr.S. Dheeraj Krishnaa,Head Telemedicine-Star Health Insurance & Dr Dhruv Joshi, CEO & Co-founder, Cloudphysician. The discussion included the impact of Telemedicine in our day-to-day life and milestones that it must overcome for better performance. Further to that we had Expert Talks by Dr.Sunil Shroff, President, TSI TN Chapter, Senior Consultant Urologist & Transplant Surgeon and Prof Dr S.Natarajan, Chief Clinical Services & Chief Vitreo Retinal Services, Aditya Jyot Eye Hospital (A unit of Dr Agarwal’s Eye Hospital) Mumbai, President Teleophthalmology Society of India, Padma Shri Awardee on Understanding Telemedicine Requirements & Regulations and Teleophthalmology for Blind Free India respectively. The last part of the session included a panel discussion on the topic Innovation & Practices in Telemedicine chaired by Ms Padma Chandrasekaran, Angel Investor and Management Advisor. This panel was designed in a way to bring out the use of Telemedicine in various fields which included Radiology, Ophthalmology, ICU, ENT, etc. The panel included Dr Amit Gupta, Radiologist, Founder, AIRMED PATHLABS, Dr. T. Senthil, Founder & CEO, Welcare Health Systems Pvt Ltd, Dr.Sheila John, Head of Teleophthalmology, Sankara Nethralaya, Dr.Vidya Ramkumar, of Speech, Language & Hearing Sciences, Sri Ramachandra Faculty of Allied Health Science and Mr Harsha Muroor, Founder & CEO, Teslon Technologies Pvt Ltd. We also had start-up demonstrations where we had 4 start-ups to show a demo of their product to the crowd.
The Conclave gave an overall view on how the pandemic has changed life digitally and adoption in healthcare in Telemedicine.
Rights of Patients vs. Rights of Doctors in Online Consultation
Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist Law Firm
Saloni Kedia
Associate, Arogya Legal – Health Laws Specialist Law Firm
Telemedicine was measured experimental few years ago but with the progression in technology it is a reality today. However, it has its own shortcomings. One of the crucial hurdles is the lack of awareness and certainty of rights amongst the patients and doctors in the practise of telemedicine. Both the patient and the physician are unclear about the standard of care to offer and how to defend his or her rights when using telemedicine. Below given are some of the rights that can be exercised by patients and doctors while interacting.
Patient and doctor identification
During the first consultation with the doctor, the doctor has a right to verify the patient’s identity to his or her confidence by asking for the patient’s name, age, address, contact, email address or any other relevant identification. However, the same is not required under a follow-up teleconsultation but, if in question; the doctor should authenticate the patient’s identification, just as he or she did during the initial visit.
Moreover, it is also the duty of the doctor to inform patient of his/her identity and qualifications before beginning any teleconsultation which in turn is the absolute right of the patient to identify the credibility of the treating doctor.
Right to choose the appropriate mode of consultation
For patient consultation, a doctor can choose any medium as a matter of right. However, before commencing with the teleconsultation, the doctor should use his or her prudent judgement to determine if such medium is suitable and in the patient’s best interests. Although patient has complete right to opt for teleconsultation, but it is again the right and liberty conferred to doctor to choose the appropriate medium for teleconsultation and decide whether to evaluate the patient in person or remotely on case to case basis.
Right to second opinion and discontinuance of teleconsultation
The patient has an absolute liberty to go for second opinion for the line of treatment or diagnosis offered by the treating doctor and the treating doctor has no authority to question for the same. Further, the patient also has a right to discontinue the teleconsultation at any time if they wish to do so.
Right to access to relevant medical information
The doctor has a complete right to ask for pertinent information from the patient during the teleconsultation before making any diagnosis or treatment decision. On the other hand, it is the patient’s duty to provide enough correct information to the doctor as it is the patient who will be accountable for the authenticity of the information exchanged with the doctor. Moreover, the doctor also has right to obtain additional medical information from the patient during the course of treatment if needed.
Patient’s sensitive data and consent
It is patient’s right to have its personal sensitive medical information to be protected when shared with doctor during teleconsultation. The doctors as a mandatory obligation should never divulge or share any patient’s information with any third party without the patient’s prior written consent.
Right to verification of the Caregiver
Before giving teleconsultation for a minor or incapacitated person, the doctor has a right to verify the caregiver’s identification and authorisation by way of any signed authority letter given by the patient or his/her legal representatives or any government proof that verifies patient’s relationship with the caregiver for ethical teleconsultation and in the best interest of the patient.
Rights under emergency situation
Needless to mention, it is the right of the patient to have access to teleconsultation in emergency situation. However, this mode can only be used if it is the only method to deliver timely care. Further, it is also the right inferred to the doctor to restrict its emergency teleconsultation to first aid, life-saving procedures, counselling, and referrals thereby giving recommendation or directive to the patient or his/her caretaker to check with the doctor in person as soon as possible.
Right to prescription, invoice and fees
The doctor has a right to charge for Tele-consultation at a reasonable rate and in turn it is the right of the patient to have a receipt or invoice issued in exchange of the fees. The patient also has the implied right to have appropriate prescription from the treating doctor with respect to diagnosis, treatment or medication, if any.
Cabinet approves implementation of Ayushman Bharat Digital Mission with a budget of Rs.1,600 crore for five years
Highlights:
ABDM will improve equitable access to quality healthcare by encouraging use of technologies such as telemedicine and enabling national portability of health services
Citizens will be able to create their ABHA (Ayushman Bharat Health Account) numbers, to which their digital health records can be linked
The Union Cabinet, chaired by Prime Minister Shri Narendra Modi has approved the national roll-out of Central Sector Scheme, Ayushman Bharat Digital Mission (ABDM) of Ministry of Health and Family Welfare, Government of India, with a budget of Rs.1,600 crore for five years. The National Health Authority (NHA) will be the implementing agency of Ayushman Bharat Digital Mission (ABDM).
Digital health solutions across healthcare ecosystem have proven to be of immense benefit over the years, with CoWIN, Arogya Setu and eSanjeevani further demonstrating the role technology can play in enabling access to healthcare. However, there is a need to integrate such solutions for continuum of care, and effective utilization of resources.
Based on the foundations laid down in the form of Jan Dhan, Aadhaar and Mobile (JAM) trinity and other digital initiatives of the government, Ayushman Bharat Digital Mission (ABDM) is creating a seamless online platform through the provision of a wide-range of data, information and infrastructure services, duly leveraging open, interoperable, standards-based digital systems while ensuring the security, confidentiality and privacy of health-related personal information.
Under the ABDM, citizens will be able to create their ABHA (Ayushman Bharat Health Account) numbers, to which their digital health records can be linked. This will enable creation of longitudinal health records for individuals across various healthcare providers, and improve clinical decision making by healthcare providers. The mission will improve equitable access to quality healthcare by encouraging use of technologies such as telemedicine and enabling national portability of health services.
The pilot of ABDM was completed in the six Union Territories of Ladakh, Chandigarh, Dadra & Nagar Haveli and Daman & Diu, Puducherry, Andaman and Nicobar Islands and Lakshadweep with successful demonstration of technology platform developed by the NHA. During the pilot, digital sandbox was created in which more than 774 partner solutions are undergoing integration. As on 24th February 2022, 17,33,69,087 Ayushman Bharat Health Accounts have been created and 10,114 doctors and 17,319 health facilities have been registered in ABDM.
Not only will ABDM facilitate evidence-based decision making for effective public health interventions, but it will also catalyse innovation and generate employment across the healthcare ecosystem…Read More
Telemedicine – News from India & Abroad
India
Ayush Ministry Gets Rs 3,050 Crore in Union Budget FY23
Ayush Ministry has been allocated about Rs 3,050 crore this year in the Union Budget 2022-23. The Budget 2022-23 was presented by Union Finance Minister Nirmala Sitharaman on Tuesday. The budget allocation will help the Ayush in the upgradation of its hospitals and dispensaries…..Readmore
Indian Government Mandates QR Codes for Drug Packages
Indian government has made QR (quick response) codes mandatory on packages of drug manufacturing ingredients to crack down on fake medicines. The Union health ministry gazette notified guidelines, saying “every active pharmaceutical…Read More
International
Artificial Intelligence (AI) — Future of Neurosurgery?
Technical performance and learning outcomes during simulated brain tumor removal may be enhanced by artificial intelligence (AI) as per a study at the Neurosurgical Simulation and Artificial Intelligence Learning Centre at The Neuro (Montreal Neurological Institute-Hospital,…Read More
Advancements in Facial Recognition Technology
Neural processing techniques allowed capturing three facial expressions by triggering actions in a VR setting as per a study published in the International Journal of Human-Computer Studies. Our face can unlock a smartphone, provide access to a secure building…Read More
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
The Omicron wave is yet another reminder that the uncertainty of this pandemic continues to haunt us but now with tele-health ecosystem getting established, the challenges are less in managing and providing care.
The importance of telemedicine for Indian healthcare sector was further stressed by our Union Minister Dr. Jitendra Singh says and he said ‘Tele-medicine Technology is going to be the Main Pillar of India’s Future Health Care System.’
The Consultation Paper on Proposed Health Data Retention Policy that opened out the discussion and asked for suggestions and Recommendations last month was an interesting exercise. We from Tamil Nadu & NCR Chapter of Telemedicine Society of India sent our recommendations to the National Health Authority. It makes interesting reading hence we have enclosed it in the newsletter.
Thank You Dr. Sunil Shroff Chief Editor President – TN Chapter – TSI
Union Minister Dr Jitendra Singh says, Tele-medicine technology is going to be the main pillar of India’s future health care system
Highlights:
Dr Jitendra Singh launches Tele-digital Health Pilot Program at BHU, Varanasi
The project starting in three districts of Varanasi, Gorakhpur and Kamjong in Manipur will cover 60,000 patients in the initial phase
Minister says, project to generate Electronic Health Record (EHR) for Indian population
Tele-medicine could save India between 4-5 billion US dollars every year: Dr Jitendra Singh
Union Minister of State (Independent Charge) Science & Technology; Minister of State (Independent Charge) Earth Sciences; MoS PMO, Personnel, Public Grievances, Pensions, Atomic Energy and Space, Dr Jitendra Singh today said that Tele-medicine technology is going to be the main pillar of India’s future health care system.
Launching the Tele-Digital Healthcare Pilot Program at BHU, Varanasi, Dr Jitendra Singh said, innovative healthcare solutions like Tele-medicine could save India between 4-5 billion US dollars every year and replace half of in-person outpatient consultations. The Minister said that Prime Minister Narendra Modi’s Digital Health Mission is the next frontier to ensure healthcare delivery is accessible, available, and affordable to all, particularly the poor living in rural and inaccessible terrain. He said, Telemedicine in the country has proven to be cost effective by about 30% less than equivalent in-person visits.
Dr Jitendra Singh said that though Telemedicine technology was in vogue for quite some time in the country, but it got a fillip in post-COVID era and in the wake of PM Modi’s push to Digital Health Ecosystem in India.
Referring to Drone delivery of vaccines in some parts of India, the Minister said, with rapid advancement in technology, Robotic Surgery will also become a reality very soon and future doctors will increasing don the mettle of Tele-Doctors.
Pointing out to very low doctor-patient ratio in India that is about one per 1,457 Indian citizens, Dr Jitendra Singh said, Tele-medicine is no longer an option but a necessity. He said, about 65 percent of India’s population that lives in rural villages, where the doctor-patient ratio is as low as one doctor per 25,000 citizens and therefore they must get best of medical advice from doctors based in towns and metropolitan cities. He said, Telemedicine will not only help the patients save their time and money, but also the doctors who can quickly assist their patients over a call for the same and actively engage in promptly treating patients with major ailments.
Dr Jitendra Singh said, the project starting in three districts of Varanasi, Gorakhpur and Kamjong in Manipur will cover 60,000 patients in the initial phase and it will be scaled up gradually to cover the entire country in the coming years. Technology Information, Forecasting and Assessment Council (TIFAC), an autonomous body of Department of Science and Technology at the Centre has designed a pilot Tele-diagnostics project in collaboration with IIT Madras-Pravartak Foundation Technologies & CDAC Mohali. This will also generate Electronic Health Record (EHR) for Indian population.
The Minister said, the project is a scalable pilot PLUG and PLAY model oriented to provide quality medical care to underprivileged women and children living in remote areas at affordable costs. The key activities include examination of the patients: women/ children with wearable devices, transferring the health data record through the e-sanjeevani cloud to a pool of doctors for analysis, and concurrently for development of EHR. The parameters that would be analysed include: ECG, Heart Rate, Blood Pressure, Lipid Profile, Haemoglobin & Foetal Doppler.
It may be recalled that Dr Jitendra Singh has established tele-consultation facility in his Lok Sabha Constituency of Udhampur-Kathua-Doda from his MP-LAD Fund, in the District Hospital Udhampur with all the Panchayats connected with it and it is being monitored on a regular basis.
Dr Jitendra Singh said that Prime Minister Narendra Modi has given very high priority to the Health Sector and this year’s budget increased the spending on healthcare by 137%, which is in line with industry expectations of 2.5%-3% of the GDP. The Minister informed that India will spend Rs 2.23 lakh crore on healthcare this fiscal including Rs 35,000 crore on Covid-19 vaccines.
The Minister said that various health care schemes launched by Modi Government such as PM Ayushman Bharat Health Infrastructure Mission, Ayushman Bharat Jan ArogyaYojana, Ayushman Health and Wellness Centres, Pradhan Mantri Bhartiya Janaushadhi Pariyojana (PMBJP) and Ayushman Bharat Digital Mission have made healthcare facilities accessible and affordable to millions of poor people in the country. Read More
Consultation Paper on Proposed Health Data Retention Policy
Recommendations from Tamil Nadu Chapter & NCR Chapter of Telemedicine Society of India hat was sent to the Joint Director (Coordination),National Health Authority Delhi
2.4 Key Issues for Consultation
1. Whether there is a need for a Health Data Retention Policy and will Indian healthcare ecosystem benefit from such a Universal Data Retention Policy and what should be the key elements of this policy?
Ans. Yes this is indeed required with advent of digital health and to make it uniform. Though we have had a late start in India, however we can learn from experience of other countries and avoid their errors
The key elements of the policy should be as follows – Structure
Formulate an independent body with reps from govt and non-govt organisations
Invite a few stakeholders from some leading countries on the board Focus
Interoperability of such data
Define data types and subtypes and give each weightage for storage
Broadly define acute care vs chronic care – more so with the increasing burden of NCDs. There is a need to store chronic care data for longer
2. How should the guiding principle of this policy be determined for the benefit of stakeholders and ease of adoption by varying sizes of entities deciding to opt in for ABDM?
Keep the policy flexible with a review every five years,
Storage should be in digital format,
Irrespective of size of entity storage time should be the same especially if it means data sharing
3.2 Key Issues for Consultation
1. As per Option 1, it has been proposed that the policy would be applicable to all healthcare entities from health data retention perspective. As per Option 2, the policy will be applicable only to entities participating in ABDM? Which would be a better option for the scope of the health data retention policy?
Ans. This has to be work in evolution. Ideally option 2 should be possible but this can become a nonstarter considering the complexity of the current healthcare infrastructure and digitations and lack of standards
Our recommendation the policy will be applicable only to entities participating in ABDM to start with an objective to integrate other entities in future.
As GoI is going to be both the provider and the payer ( through its universal health insurance schemes) it will not be too difficult to set standards and have a uniform system.
After the initial learnings it can recommend other entities too join.
However an option can be provided to all entities to join without making it compulsory
2. How such a policy should be implemented given limitations in terms of infrastructure, capability, and sufficient understanding of health data in the healthcare ecosystem?
This will take time but then following would be required-
Regular seminars and educating healthcare professionals and managers
Setting minimum standards requirement and making this a requirement for accreditation for health insurance claims, NABH and NABL
3. As ABDM has a provision for opt-out, in such a scenario what may be the possible implications from the perspective of health data retention?
Ans. This has been answered in the first question. A flexible approach would help stakeholders understand and appreciate the importance of data harmonisation and data retention. It would help avoid fear psychosis, would give time and feedback of what is implemented and make changes in the policies.
Having the payers on the side of the GoI would also help entities to fall in line.
However, where ever the GoI is a stakeholder as a payer and provider – it should be made compulsory and no opt out option should be provided.
4.8 Key Issues for Consultation
This is the most important chapter of the current document. What must remember is that so far the hospitals have followed a physical format of preservation of data. While this has certain advantages in a hospital setting for a follow up system for medical professionals but it adds costs for physical storage, retrieval, classification and maintenance.
This has resulted in many hospitals not having a medical records section at all resulting in patients carrying their medical file from hospital/doctor to another hospital/doctor.
The digitation of records help the whole ecosystem and creates efficiency in the it.
1. Should a blanket retention duration be adopted for all health records in India or different schedules be defined as per a classification? Which is a better approach of retention?
Ans. If blanket retention is followed it would avoid much confusion and discussion.
The number of years for data retention are random and there are no studies that these periods make any sense in the context of data retrieval or other requirements and these are based to lessen the physical storage burden. However, with digitisation of data and the cost of the same coming down, a rethink is required as this is a new paradigm we are addressing and has no comparison to the physical world.
2. How granular should data classification be? Is more granularity required beyond that presented in the sections above? Addressing this aspect of the Health Data Retention Policy would help assess whether minimalist data classification – pertaining only to inpatients and outpatients – would suffice the purpose of health data retention. A minimalist data classification would have both advantages and disadvantages. Please suggest your view in this regard.
And 3. How in your view will a detailed granular data classification enable a better health data retention? Please suggest your view on the classification of health record types as proposed above or if any further granularity is necessary and what are the overarching benefits for different stakeholders?
Ans. Most health data are interlinked from point of patient care and really subclassifying again applies better when there is a physical need of storage of such data.
A new paradigm of data classification will emerge in the digital world. It may be defined as a health condition being cured or not cured. Being acute and cured or acute and not cured or chronic and cured or chronic and not cured.
Again, if blanket retention is followed granularity of data would have not much meaning
4. What should be the ideal duration for these different health data types?
Ans. Different countries follow different timelines and this is random depending on investment in medical record section.
It is generally recommended that the Personal health record should be available for lifetime hence why should other data retention be looked at differently.
UK follows 20 to 25 years. We currently feel this should be the minimum time of retention with a recommendation for it to be ideally for lifetime.
We need to look ahead and serve the new generation borne in the digital age. For a child born today, 10 years of data retention would be meaningless. For someone with chronic care one can’t delete data that goes beyond 10 years.
At this stage as said earlier, the minimum period should be defined as not less than 20 years and recommended for lifetime. A review should be possible in time to come. 10 years is too short a time.
5. While ABDM proposes that all entities opting to join NDHE must be able to retain health data in electronic format, and other entities of the healthcare ecosystem may consider physical or original formats, what options should be made allowable as part of the policy being proposed? Health data records can be only digital, only physical, or combination in any hospital. Accordingly, the question arises whether all the above considerations should fall under one policy or under separate/independent policies?
Ans. Digital format should be compulsory and physical should be optional. A uniform policy would cause less confusion and also be a trigger for the much required change.
6. Should there be a provision for extension of duration or retention of health data under the policy being proposed? What considerations should be made in defining the guidelines, allowing for such an extension?
Ans. Keeping it flexible is the key as time would be required for change. However, at the same time to quicken the process Incentives or a reward system could be created to hospitals, entities, states, cities etc that adopt and implement the change.
In fact, as a starting point all smart cities policies should have this policy as one of the pre-requisites.
7. Who shall have the apex authority to oversee and implement health data retention? Which entity as part of the ecosystem should be rolling out this policy at the macro-level?
Ans. Initially the National Digital Health Authority should be in charge, however creating an independent body with key stakeholders would be ideal under the National Digital Health Authority.
8. How can smaller clinics or centres, both public and private, build capability in a timely and cost-efficient manner to take responsibility of data retention for long time periods?
Ans. The health insurance in the country already has certain requirements and many smaller clinics are slowly adopting some of these requirements. Most will eventually have to fall inline or the larger good.
Hospitals with less than say 25 beds maybe given a longer gestation period for adoption.
9. How can business continuity be ensured in case of fall of the establishment, platform or service providers?
Ans. This is going ot be challenge and requires further deliberation.
In case of closure of an establishment all the data should be transferred to a central repository which can be state or central driven and a mechanism would need to be devised.
Questions to be answered –
Format of such a body
If the data is in physical format who would bear the cost of digitisation
Method of usage of such data
5.5 Key Issues for Consultation
1. Will the governance model as per Health Data Management Policy be sufficient for the retention policy?
Ans. There needs to be audit system by third party that needs to be built in to ensure trust, compliance and accountability
2. How will the policy regulation be enforced and what should be the structure across relevant entities responsible for retaining the health data?
Ans. This would require to be implemented as addendum to many regulations.
Some of these would need to be part of the regulatory structure of PDP Bill on data protection after it is passed by the GoI
3. How should the implementation of the policy be done in case the policy is made applicable for the ecosystem beyond ABDM?
& 4. Is there an alternative model or policy approach which could be considered?
Implementation of the policy will happen if it becomes part of a regulatory requirement.
A start needs to be made and it needs to evolve and change from time to time. There are no perfect policies or perfect implantation and one cannot have all the answers to various questions that crop up.
A Unique Blended Mental Health Support Delivery Model
Smriti Joshi, MBPsS, M.phil in Clinical Psychology Advanced Certified Telebehavioral Health Professional (www.telehealth.org) | Lead Psychologist & Member Board of Directors, Wysa
In-person mental health support is not replaceable yet it cannot scale enough to address this rapidly increasing need to provide mental health support to this growing public mental health support crisis. (AI)-enabled, empathetic, and evidence-driven conversational agents are now being considered a way to rapidly scale mental health support provision, augmenting existing mental health services. Wysa is one of the world’s leading solutions in this space, with 4 million users served, who have had 485 million conversations in 65 countries.
Wysa was founded in 2016, and I am part of the 5 member founding team.
A. Wysa Introduction & Background
Wysa ‘s service model can be best imagined as a unique 3-layer ‘pyramid of care’, based on an anonymous, text-based app interface that can create custom care pathways. App users get help through –
(1) an emotionally-intelligent AI-CBT delivering chatbot providing 24X7 support,
(2) a library of evidence-based self-help tools and techniques to help build resilience.
(3) online therapy with professional clinical and counselling psychologists.
The model is affordable (cost of triage can be 90% lower), scalable (It can support a 4 million user base with a 70 people team), and flexible to integrate with existing service ecosystems; so it is very suitable for early stage intervention, and support at a population level.
The AI is built inhouse, and tuned for emotional intelligence, delivering evidence-based AI-driven Cognitive Behavior therapy (AI-CBT). Wysa allows for free text input which makes the conversation empathetic allowing for a richer user experience. Wysa’s 100+ NLP models, built on 485 million+ conversations, make its ‘listening’ ability unique and the best in the world today. This AI meets global Clinical Safety standards, are ISO certified, and is explainable using non-generative models that can be audited for clinical safety.
B. Global Leadership
Wysa is a global leader in conversational AI for behavioral health and has already helped improve mental health care for over 4 million individuals across 65 countries. It is the preferred digital behavioral health partner for organizations like Accenture, Aetna, Travelers, and the National Health Service (NHS) in the UK, and the Ministry of Health in Singapore.
Wysa is rated #1 at 93% by ORCHA, the NHS digital app evaluation agency – the highest across all categories – including a 100% on clinical assurance.
It has recently won the NHS NIHR AI Award, aims to accelerate the testing and evaluation of AI technologies in the NHS so patients can benefit from faster and more personalized diagnosis and greater efficiency in screening services.
Wysa’s efficacy for managing depression has been established through a peer-reviewed study published in JMIR, the world’s top e-health journal. We are currently running clinical trials with Harvard Medical School, Columbia, Cambridge, Washington University and the NIHR in the UK: 10 other research papers are underway, and will be published in 2022.
C. My Role & Contributions
The last 6 years of working at Wysa have been the most productive and fulfilling years of my career as there has been immense learning around how AI and machine learning can make healthcare more accessible and scalable and bridge the existing gap in service provision due to various challenges.
Apart from being part of Wysa’s founding team and serving on the Board of Directors, I have set up a 30-people clinical and therapist team that supports clients from India and 30 other countries using Text based and Audio-video counselling and psychotherapy – starting in India, we now have clinical team members in the US and UK. In addition to clinical inputs for product design for our AI platform, the team has also completed more than 10,000 therapy sessions in the past 3 years with a 95% client approval rating.
In addition, I have been the company’s senior representative at Swasth Alliance, an public-private partnership between the Ministry of Health & Family Welfare, Govt of India, and a consortium of startups in the Indian ecosystem coming together to serve the country during Covid. I am also part of the leadership team driving Wysa’s response to the mental health challenge brought upon by India’s third Covid wave, through a partnership with ACT Grants (a multiparty donor consortium) and the Govt of India.
The burden of care on health care professionals is immense. While setting up a team for remote delivery services, especially during the recent covid-19 waves, where psycho-therapy providers themselves were struggling with covid-19 related concerns, I developed a keen interest in an area often neglected by practitioners themselves- compassion fatigue and burnout in health care providers.
Ensuring my team’s well being and building team resilience became my key focus and I ensured that this work was carried out via an action based research effort at Wysa.
We are creating new models of tele-therapy that combine human support with AI-led CBT, that are cutting-edge and unique and our unique culture, ethos and spirit of service are being recognised in clinical and practitioner communities within tele-therapy globally. I have been invited to offer mentoring and support to aspiring psychologists from across the world via this https://www.therapistsintech.com/ to assist them in their phase of transition from making a shift from in person clinical practice or academia to delivering services via online modalities and also helping platforms build resilient remote service delivery teams, especially in the wake of covid-19. These efforts were acknowledged by this international platform and I was awarded with “The outstanding mentor in tech award for 2021”.
A model for sustainable, partnership-based telehealth services in rural India: An early process evaluation from Tuver village, Gujarat
Shoba Ramanadhan 1, Krishnan Ganapathy 2, Lovakanth Nukala 2, Subramaniya Rajagopalan 3, John C Camillus 4
Prof. Krishnan Ganapathy Past President, Telemedicine Society of India & Neurological Society of India | Hon Distinguished Professor The Tamilnadu Dr. MGR Medical University | Emeritus Professor, National Academy of Medical Sciences | Formerly Adjunct Professor IIT Madras & Anna University | Director Apollo Telemedicine Networking Foundation & Apollo Tele Health Services | URL: www.kganapathy.in
Abstract
Background: Telehealth can improve access to high-quality healthcare for rural populations in India. However, rural communities often have other needs, such as sanitation or employment, to benefit fully from telehealth offerings, highlighting a need for systems-level solutions. A Business of Humanity approach argues that innovative solutions to wicked problems like these require strategic decision-making that attends to a) humaneness, e.g., equity and safety and b) humankind, or the needs and potential of large and growing markets comprised of marginalized and low-income individuals. The approach is expected to improve economic performance and long-term value creation for partners, thus supporting sustainability.
Methods: A demonstration project was conducted in Tuver, a rural and tribal village in Gujarat, India. The project included seven components: a partnership that emphasized power-sharing and complementary contributions; telehealth services; health promotion; digital services; power infrastructure; water and sanitation; and agribusiness. Core partners included the academic partner, local village leadership, a local development foundation, a telehealth provider, and a design-build contractor. This early process evaluation relies on administrative data, field notes, and project documentation and was analyzed using a case study approach.
Results: Findings highlight the importance of taking a systems perspective and engaging inter-sectoral partners through alignment of values and goals. Additionally, the creation of a synergistic, health-promoting ecosystem offers potential to support telehealth services in the long-term. At the same time, engaging rural, tribal communities in the use of technological advances posed a challenge, though local staff and intermediaries were effective in bridging disconnects.
Conclusion: Overall, this early process evaluation highlights the promise and challenges of using a Business of Humanity approach for coordinated, sustainable community-level action to improve the health and well-being of marginalized communities.
Publish or Perish
The Oxford Dictionary of Phrase and Fable, describes ‘publish or perish’ as an attitude or practice existing within academic institutions, whereby researchers are put under pressure to produce journal publications to retain their positions or to be deemed successful, The phrase is attributed to Coolidge who enunciated this theory in 1932. Successful publications draw attention to scholars and their sponsoring institutions. This , helps getting funds for research projects. However the pressure to publish also causes poor work being submitted to academic journals.
Publications in Telehealth have increased exponentially in the last 2 years. The author personally reviews at least one article a week from several international journals. Journals are measured by their impact factor (IF), which is the average number of citations per article published in that journal. Not many Indian journals have an impact index of even more than 2.5 .Neurology India for example has an IF of 2.7 . New England Journal of Medicine has an IF of 92 !! What is an author’s impact ?. This is traditionally measured using the number of citations a single article has received. Today this information can be obtained in real time. The impact of a publication can also be determined by the number of times a free access article has been downloaded.
Publishing a paper in a well known journal is time consuming and labor intensive. In academic institutions a good library, secretarial help and residents are available to help the faculty to put together a paper. As mentioned earlier it is part of their job profile and is essential for survival. Interestingly more services in various aspects of telehealth are offered in the private sector. Here the story is different. In large private institutions a P&L driving CEO has concerns, and rightfully so, in making available “confidential” data in the public domain. Top journals insist on full access to nitty gritty. There is a conflict of interests. Paper publication takes a back seat. HR are dedicated to managing the operations. They generally do not have a Paper publishing background. Not being a part of their KPI it is extremely difficult to make them do extra work.
Publishing papers in national / international journals in the field of Telemedicine do have a RoI. Unfortunately this takes considerable time. It is not a low hanging fruit. From a purely personal growth perspective, every time one writes a paper, one becomes a little more knowledgeable. Literature review ensures that we are up to date. Defining the problem, spelling out exact aims and objectives, documenting observations , extrapolating inferences, writing a discussion and making conclusions when repeatedly done becomes part of one’s DNA. Writing an article makes one see the Big Picture. Getting an article accepted for publication is an art and a science. : https://www.neurologyindia.com/text.asp?2021/69/6/1547/333463. Adopting a scientific approach means more business !
India is indeed a paradox. In terms of numbers we probably provide more teleconsultations every single day than most countries on this planet. It is often stated that the sheer volume of work prevents us from meticulous documentation and follow up which is the sine qua non of doing any impact study. Interestingly even politicians and administrators want hard core scientific evidence that our remote intervention is cost effective resulting in significant difference in the ultimate health care outcome. The only way to get this evidence is to plan a paper for the NEJM and be patient for 3 years !! A prospective multi institutional well designed and funded study resulting in multiple papers alone will enable India to take a leadership role in the comity of nations. Improbable Yes. Impossible No. Do hope the Next Generation will take this seriously and not treat it as the rumblings of a septuagenarian. 22 years after the birth of Telehealth in India we should no longer follow high standards. We must set them. We should not be talking of achieving world class. The world should talk about achieving India class. We have the potential to bring out at least 40 papers every year in journals with an IF of > 2.5 . Doing qood quality work alone is not enough. The world should know about it !!
Handling Sensitive Situations through Telemedicine
Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist Law Firm Eshika Phadke Associate, Arogya Legal – Health Laws Specialist Law Firm
The legalisation of telemedicine has been a boon for access to healthcare. However, the increased reliance on telemedicine has also been accompanied by unintended consequences: doctors may receive requests during consultations that are of a risky or highly sensitive nature, that they may not be comfortable handling.
For instance, a doctor may be consulted by a patient for a matter that requires an in-person examination, or it may be that the medication that the patient requires for their condition cannot be prescribed through telemedicine, but the patient refuses to visit a clinic or hospital and insists on receiving treatment through a teleconsultation only. In such a case, the doctor must inform the patient that a diagnosis cannot be arrived at or treatment cannot be commenced through a teleconsultation, and should meticulously record the patient’s refusal to seek a physical consultation. The doctor should inform them of the risks of not seeking proper treatment, and should record that the patient has been informed of the risks and is still refusing to seek proper treatment. Essentially, the doctor should capture that the patient was fully informed of the situation, and that he/she acted against medical advice.
In more extreme situations, a doctor may be consulted in an emergency situation where the patient requires urgent care. The doctor should advise the patient or caller to call an ambulance or rush to a hospital immediately. If required, the doctor may also inform the caller of the first aid measures that must be carried out.
There may be situation wherein a patient is verbally abusive or behaves inappropriately, perhaps even to an extent where the doctor feels uncomfortable or at risk. In such a situation, the doctor may advise the patient to consult with another doctor, end the consultation, and record his/her reasons for doing so. Depending on the severity, the doctor may also file a complaint with the police. If the doctor is consulting through a telemedicine service provider, he/she should also inform the management so that they can take appropriate actions.
If a patient is incoherent and appears to be either of unsound mind or inebriated, the doctor should ascertain whether there is a caregiver or trusted person whom the doctor may speak to for clarity and to give further instructions to. Doctors should exercise great caution while administering advice to a person who does not appear to be lucid.
A patient may display suicidal tendencies or even outrightly express that they intend to hurt either themselves or another person. In such situation, as with regular consultations, the doctor must promptly inform the authorities. Similarly, if the patient confides in the doctor that he/she is the victim of abuse or has been assaulted, the doctor should consider whether the authorities ought to be notified. Note that, to the extent that it is practical, guidelines for medicolegal cases should be adhered to for cases that are of a medicolegal nature.
Such situations are not specific to telemedicine, and may also occur with in-person consultations. Doctors should ensure that they apply at least the same level of prudence and professional judgment for remote consultations, and should ensure that they maintain meticulous records of such interactions (including any complaints made to authorities in relation to such interactions). Wherever possible, they should attempt to ensure that the records also reflect that the patient was made aware of the situation, and the patient concurs with what is being recorded in the doctor’s notes.
Telemedicine – News from India & Abroad
New Device Helps Measure Blood Pressure and Other Vitals
New ‘finger clip’ device has been designed to measure and monitor blood pressure consintuously, reveals a new study.Monitoring a person’s blood pressure on a regular basis can help health care professionals with early detection of various health problems such as high blood pressure…..Readmore
Artificial Intelligence (AI) Helps Improve Patient and Doctor Communication
Understanding between a patient with low health literacy and doctors can be improved with the help of artificial intelligence (AI) as per a study at the University of California – San Francisco, published in Science Advances.The study team performed a computer analysis of 250,000 … Read More
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- https://www.medindia.net




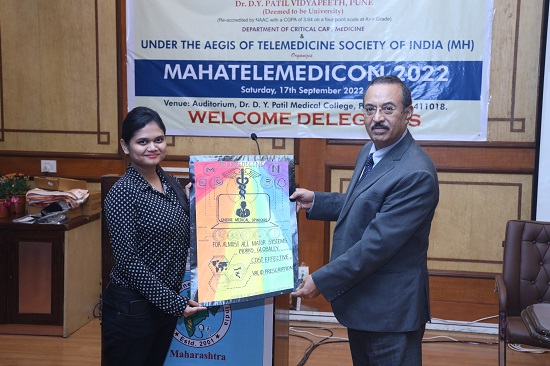




 Digital India Act and Pending Legislations
Digital India Act and Pending Legislations TSI Mid-Term Conference – Proceeding and Recommendation Thereof
TSI Mid-Term Conference – Proceeding and Recommendation Thereof



 TELE ICU – Challenges and Solutions
TELE ICU – Challenges and Solutions


 Teleconsultations between doctors
Teleconsultations between doctors Necessity for formally dually trained Clinician Scientists and Clinician Technologists
Necessity for formally dually trained Clinician Scientists and Clinician Technologists

 Mobile Teladoc Health Robots at MMHRC
Mobile Teladoc Health Robots at MMHRC









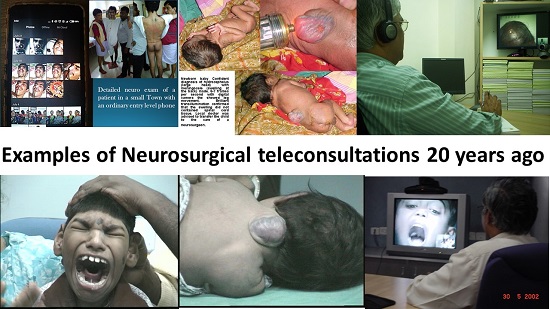
 Role of Telemedicine in Stroke
Role of Telemedicine in Stroke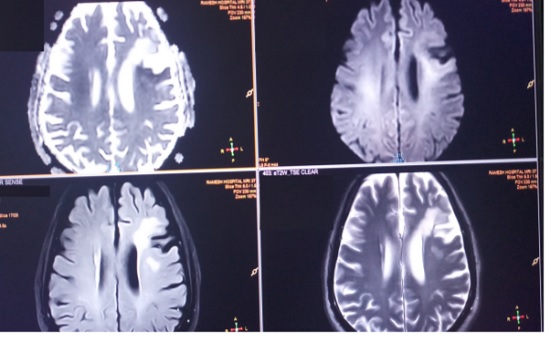
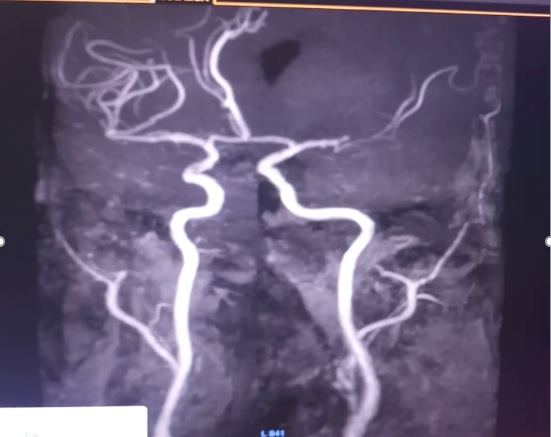
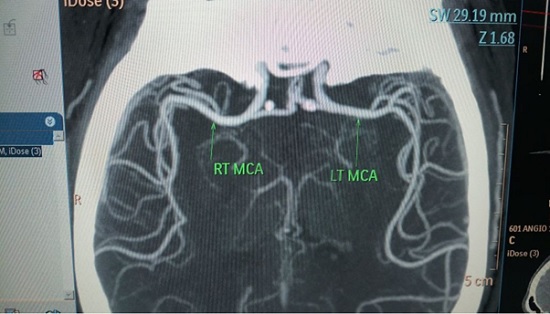
 Tele-Neurorehabilitation: A story from Mumbai
Tele-Neurorehabilitation: A story from Mumbai
 Understanding the implementation of telepractice in speech and language services for children and adults using a mixed-methods approach
Understanding the implementation of telepractice in speech and language services for children and adults using a mixed-methods approach

 Decoding the Healthcare Professional Registry’s Utility in Telemedicine
Decoding the Healthcare Professional Registry’s Utility in Telemedicine TELEMEDICINE IN INDIA: A CRITICAL ANALYSIS OF THE EXISTING LEGAL FRAMEWORK – A Summary
TELEMEDICINE IN INDIA: A CRITICAL ANALYSIS OF THE EXISTING LEGAL FRAMEWORK – A Summary
 Prescriptions and Digital Signatures
Prescriptions and Digital Signatures

 Technology Transformation of Critical Care
Technology Transformation of Critical Care

 eACCESS : Surfing the stormy waves of the pandemic
eACCESS : Surfing the stormy waves of the pandemic
 HTIC HEALTHCARE CONCLAVE – TELEMEDICINE
HTIC HEALTHCARE CONCLAVE – TELEMEDICINE