Telehealth Newsletter
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
August has been a pivotal month for India’s Telehealth landscape. Here are some noteworthy developments:
1. On 3rd August, the National Medical Commission approved the updated Telemedicine Guidelines as part of the Ethics and Medical Registration Notification.
2. The DIGITAL PERSONAL DATA PROTECTION ACT (DPDP) received Parliament’s nod on 13th August.
3. Despite these advancements, the Indian government remains hesitant to legislate e-pharmacies.
In response to significant opposition from the medical community, primarily concerning the prescription of generic medicines, the Health Minister paused the Ethics and Medical Registration Board Notification. While issues around generic medicines are being addressed, it is anticipated that the telemedicine guidelines will remain intact. We encourage our members to familiarize themselves with the notification. Key topics such as patient consent, the role of healthcare workers, follow-up consultations, and clarity on medication dispensation via tele-consultation have been elaborated upon.
This edition offers a concise overview of the Personal Data Protection Act, an insightful article on the ethics of ChatGPT and an article on patient perspective of Psychiatry, and more.
We cordially invite you to register for TELEMEDICON2023 and eagerly await your abstract submissions.
Thank You
Dr. Sunil Shroff
Chief Editor
President – TN Chapter – TSI
ChatGPT and Ethical Issues
Dr. K. Ganapathy
Distinguished Visiting Professor IIT Kanpur | Distinguished Professor The Tamilnadu Dr MGR Medical University | Emeritus Professor National Academy of Medical Sciences | Adjunct Professor, SIPA Columbia University | Director Apollo Telemedicine Networking Foundation &, Apollo Tele Health Services
ChatGPT (Chat Generative Pre-Trained Transformer) is an AI chatbot developed by OpenAI and launched on November 30, 2022. Eventually ChatGPT could be a major integral component, in a doctor’s training and armamentarium. For this to happen, real time and continuous retraining is mandatory. This implies updating with accurate, reliable, unbiased data from the real world of healthcare. The ability of ChatGPT to think, analyse and behave like a healthcare provider in 2030 would certainly be much more related to the then real world. Understanding the complex relationships between different co existing clinical conditions and different management strategies alone is not enough. Also to be taken into account is the patient’s specific desires and unfortunately his/her socio-economic status. In a publication “When Doctors Use a Chatbot to Improve Their Bedside Manner” the authors point out that doctors were asking ChatGPT to help them communicate with patients in a more compassionate way. In fact, an emotional letter generated by ChatGPT made an insurance provider reconsider the original decision of denying benefits ! Users may also blindly trust ChatGPT due to its incredible capabilities. Potential for bias and discrimination in the initial training material used, in creating ChatGPT, may generate outputs that reflect and perpetuate these biases. This could lead to unfair treatment or negative consequences for specific groups. Regular audits, ongoing monitoring, and adopting fairness-aware, Machine Learning techniques, are necessary. ChatGPT unfortunately may even have the potential to propagate disinformation. Training data is essentially from pre-2021, not taking into account the considerable progress since then. Ethically, even the predominance of whites constituting the ethnic composition of the OpenAI team has been questioned !! Meticulous attention to data privacy, quality and quantity, security, regulations, integration with existing systems and ensuring constant human oversight are bothersome ethical issues. Though ChatGPT can generate human-like text, at present it does not have the ability to think, reason, or understand the context of the information generated. ChatGPT adheres to European Union’s AI ethical guidelines, concentrating on human oversight, technical robustness and safety, privacy and data governance, transparency, diversity and non-discrimination, societal and environmental well-being, and accountability. Healthcare in the next decade could be totally different. New codes of conduct need to be evolved. An AI influenced Hippocratic Oath may well be called “The Robocratic Oath”. Would not deploying AI be considered malpractice? Machines, like humans, can also commit errors. “To err is ChatGPT, to forgive is human”. This would be the adage of the future !!

Patient’s Perception of Telepsychiatry in India
Dr. Vikrant Mittal
MBBS, MD (Psychiatry), MHA, FACHE, FAPA
Rahul Talwar
BA, MSc. Clinical psychology
Background:
Telepsychiatry services had been growing pre-pandemic but was sporadic and scattered in India. After the COVID-19 pandemic telepsychiatry has led to integration of telepsychiatry services into many clinics and hospitals across India. This has led to a shift in the model of telepsychiatry services toward contemporary views of integrated care (collaborative care model) and transition consultation clinic models (Naik et al., 2020). Dynamic changes in the field affect both clinicians and patients. Psychiatrists and healthcare systems will be better able to customize their approaches in order to respond to the patient’s perceived needs if they are aware of the patient’s perspective on telepsychiatric services.
Progress:
There are various facets of telepsychiatry that have been studied in multiple areas from patient perspective. Few of those are discussed here.
Acceptance: The privacy and easy access to telepsychiatric services have resulted in over 90% of patients reporting “very much” and “high” acceptability of them. However, these reports of satisfaction and acceptability are only in online follow-up sessions. These results indicate the need and effectiveness of transition consultation clinic models. (Das, 2020)
Cost-Effectiveness: Both integrated care (collaborative care model) and transition consultation clinic models of telepsychiatry were found to be economically sustainable in a study by Moirangthem et al. (2017). The same study also states that in comparison to tertiary care facilities and community outreach programs, telepsychiatry implementation cost are anywhere from 4 to 50 times more economically, depending upon individual practitioner’s pricing and other socio-economic determinants. Additional benefits felt by patients and practitioners are an increased frequency of consultations, with a reduced consultation time which also leads to better monitoring of symptoms and drug titration.
Barriers: A practitioner who cannot speak the patient’s language or dialect causes a lot of misinformation and miscommunication between the parties. This causes frustration, and hampers therapeutic alliance. An alternative to this is having an interpreter present within the session. This is generally not preferred by patients. A study showed that instead of conversing with an interpreter, patients preferred to use teleconsultation with a psychiatrist who is located far away and speaks their original tongue, an option made easy through telepsychiatry. (Mucic, 2008)
Age-based perspectives: Children and adolescent populations view technology-assisted consultations as novel and intriguing. They also proved to be more proactive in the telepsychiatry process and appreciated the sense of control that it offers to a patient (Boydell et al., 2010). Furthermore, the parents also reported increased satisfaction as they did not have to skip work to take their child to a clinic. However, patients of geriatric populations reported hesitance to an almost non-modifiable level with respect to telepsychiatry services. (Gardner et al., 2015)
Conclusion:
Patients’ perception towards psychiatry/ psychotherapy may be hesitant in the beginning. Yet it is progressively positive, especially in transition consultation clinic models. It is increasingly used for providing psychological services in disaster areas, rural, semi-urban areas. Thus, this model of providing psychiatry/ psychology services/ practice has the most beneficial effects for both patients and clients.
References:
Boydell, K. M., Volpe, T., & Pignatiello, A. (2010). A qualitative study of young people’s perspectives on receiving psychiatric services via televideo. Journal of the Canadian Academy of Child and Adolescent Psychiatry, 19(1), 5.
Das, S., Manjunatha, N., Kumar, C. N., Math, S. B., & Thirthalli, J. (2020). Tele-psychiatric after care clinic for the continuity of care: A pilot study from an academic hospital. Asian Journal of Psychiatry, 48, 101886.
Gardner, M. R., Jenkins, S. M., O’Neil, D. A., Wood, D. L., Spurrier, B. R., & Pruthi, S. (2015). Perceptions of video-based appointments from the patient’s home: a patient survey. Telemedicine and e-Health, 21(4), 281-285.
Moirangthem, S., Rao, S., Kumar, C. N., Narayana, M., Raviprakash, N., & Math, S. B. (2017). Telepsychiatry as an economically better model for reaching the unreached: A retrospective report from South India. Indian journal of psychological medicine, 39(3), 271-275.
Mucic, D. (2008). International telepsychiatry: a study of patient acceptability. Journal of Telemedicine and Telecare, 14(5), 241-243.
Naik, S. S., Manjunatha, N., Kumar, C. N., Math, S. B., & Moirangthem, S. (2020). Patient’s perspectives of telepsychiatry: the past, present and future. Indian journal of psychological medicine, 42(5_suppl), 102S-107S.

Government Reluctant to Formalize Online Drug Sales
Dr. Pavithra
Assistant Editor, Medindia.net
In a significant setback for the ePharmacy sector, government officials have displayed reluctance in formalizing the online sale of drugs and medications. A meeting between industry representatives and officials, held at the office of the Drugs Controller General of India (DCGI), aimed to address concerns related to the regulation of ePharmacies.
Insiders familiar with the matter have revealed that the government remains unconvinced by the proposals presented by ePharmacy representatives and intends to maintain the current state of affairs. A high-ranking official stated, “The government is not inclined towards endorsing ePharmacies; instead, they wish to maintain the current mode of operation. The government has informed them that the sector will not be formalized in its present structure.”
Prioritizing Safety and Authenticity in ePharmacy Sector
This discussion followed a previous interaction between ePharmacy stakeholders and Health Minister Mansukh Mandaviya earlier this month. The government’s primary objective in regulating online drug sales is centered around mitigating risks such as the circulation of counterfeit medicines, addictive narcotics, and potential national security concerns.
During the meeting with leading ePharmacy entities, Mandaviya expressed reservations about the existing model of online drug sales and stressed the necessity for enhancing the approach to address these concerns. Prominent companies such as Tata 1mg, Netmeds, Amazon, Flipkart, Practo, Apollo, and PharmEasy were among the participants.
To combat illicit online drug sales, the health ministry is reportedly planning to introduce a national portal for ePrescriptions. It is anticipated that doctors will be required to register on this platform to provide online prescriptions, thereby enabling patients to purchase their prescribed medications.
The government’s aim is to discourage the misuse of prescriptions by implementing an ePrescription network for the online sale of drugs and medicines. “The government envisions a Zomato-Swiggy model for medicine delivery, where delivery personnel would collect medicines from physical stores and deliver them to customers.
E-pharmacies can lead to potential drawbacks such as misuse of antibiotics, lack of proper medical recording and potential ethical legal concerns. Earlier this year, the ministry issued notices to 31 firms for selling medicines online without the necessary permissions.
The government’s commitment to regulating the online pharmaceutical sector stems from its dedication to ensuring the safety and authenticity of medications accessible to consumers. However, the potential drawbacks outlined above highlight why some doctors are wary of ePharmacy and its potential impact on patient care and safety.
As deliberations continue between ePharmacy stakeholders and government officials, the future of the online drug sales industry remains uncertain.

E-Pharmacy: Why Is India Still Waiting to Legalize Its Regulation?
Dr. Krishanga Srivastava
Associate Editor, Medindia.net
Dr. Sunil Shroff
President, Tamil Nadu Telemedicine Society of India | Consultant Urologist & Transplant Surgeon
In a world racing towards digital dominance, where convenience wears the crown and efficiency holds the scepter, the concept of e-pharmacy is seen as the logical next step. However, in a stark demonstration of how the regulatory system struggles to keep pace with ongoing technological advances, the state of the Indian pharmaceutical industry has been in a turmoil carrying the legacy of the past and unable to make the change to embrace the future.
The problem stems from the fairly big underground market of counterfeit medication, ease of purchase of prescription medicines in India and unqualified quacks practicing as doctors.
Is India Compromising the Healthcare Sector?
India’s healthcare sector is subject to complex regulations to ensure the quality and safety of medications. Age old practices refer to the manufacture, sale, and distribution of drugs. But with the rise of online sales, these laws lack any clarity and falter in handling the complexity of e-pharmacies, sending the regulators into a legal spin.
The lack of a clear rulebook has created a series of problems for e-pharmacies. Chief among these are the locations of the search results. Under current legislation, pharmacies must have a physical infrastructure. This stifles innovation for e-pharmacies and stalls their development. It’s like telling a digital virtual object to stay in the physical realm, and they miss what’s really important.
The interstate drug trade is another quagmire. State laws mean that drugs that are legal in one region can be illegal a few miles away. This legal confusion not only confuses consumers but also cripples e-pharmacies in the legal conundrum.
The economic side is equally murky. While some laws only require payment upon shipment, countless online payment methods tend to work outside these limitations. This confusion enhances concerns about liability and consumer safety, putting buyers and sellers in dangerous situations.
Immediate concerns involve the sale of prohibited Schedule H and X drugs. These drugs should be strictly regulated, but e-pharmacies have the danger to open the door for its abuse. The potential for online re-use of a prescription highlights the need for rigorous checks and random audits by oversight committee.
Verifying patient identities is another glitch. The online realm struggles to authenticate prescriptions, risking the sale of prescription drugs without medical oversight. And with no regulations barring sales to minors, the threat to public health multiplies.
Even as the standard rules have been around for years, brick-and-mortar establishments continue to compete with digital entrants. Reports say that delivering drugs home disturbs legitimate concerns and threatens their turf. However, disruption in others sectors too has changed the way business is done and pharmacies should be ready to accept these challenges.
One solution to check for quality and also improve supply chain would be to use bar codes on medication packaging. This could easily be implemented and ease many concerns of patient safety.
While e-pharmacies promise to democratize healthcare, especially in remote locations but the lack of cold-chain logistics if required, can limits accessibility, leaving this section of the population unserved.
It’s time India recognizes tech’s power and the potential of e-pharmacies and this will require a foolproof regulatory framework, not just for progress but also to create access to the last mile. The digital age craves modern solutions, not archaic rules. The government must champion innovation, support technological advances, and find the right balance between regulation and advancement with an overall objective for a safe, efficient, and affordable healthcare for all.
Forecasts have already predicted India’s e-pharmacy sector having touched Rs 25,000 crore in 2022. The urgency for clarity prodded FICCI to push for e-pharmacy regulations, calming stakeholder jitters. Sector specialist Dr. B R Jagashetty insists the government should hasten the finalization of these rules.
E-Pharmacy’s Legal Framework
Few key areas for e-Pharmacies include the following:
Only registered pharmacies can sell medicines.
Certain drugs need valid prescriptions.
Exporting medicines is illegal.
Registered practitioners can only sell on prescriptions.
Selling prescription drugs to minors is forbidden.
The sale of banned drugs is strictly prohibited.
The Flawed Draft of E-Pharmacy Rules
Draft rules from 2018 cover e-pharmacy operations, like registration, distribution, and inspection. But, they’re flawed.
They don’t tackle prescription verification or misuse.
Privacy and storage concerns loom large.
The government’s role in customer data remains hazy.
The draft misses the privacy policy display and customer data retention guidelines.
In conclusion, e-pharmacies could reshape healthcare accessibility and affordability. Robust regulations are vital for safety and function. Stricter licensing, verification logos, barcoding, digital data storage, and integration with health schemes would go a long way in making it a safe way forward.
There is an urgent requirement for the government requires to invest more in cleaning up the current state of how the physical pharmacies operate. No pharmacy should dispense drugs without a valid prescription and all counterfeit drug operations need to be stopped.
Given our reliance on e-commerce and events like COVID-19, we require clear e-pharmacy rules. By studying global models, India can regulate e-pharmacies smartly, reaping the benefits while securing public health and accessibility.
But unless the government acts on this draft and indulges in further meaningful deliberations, we will never be able to regularize healthcare and instead of promoting good health in the community, we might end up granting them access to dangerous drugs including narcotics and dangerous prescription drugs.
Source: Medindia.net
Salient Features of the Digital Personal Data Protection Bill, 2023
The Bill provides for the processing of digital personal data in a manner that recognizes both the rights of the individuals to protect their personal data and the need to process such personal data for lawful purposes and for matters connected therewith or incidental thereto.
- The Bill protects digital personal data (that is, the data by which a person may be identified) by providing for the following:
- The obligations of Data Fiduciaries (that is, persons, companies and government entities who process data) for data processing (that is, collection, storage or any other operation on personal data);
- The rights and duties of Data Principals (that is, the person to whom the data relates);and
- Financial penalties for breach of rights, duties and obligations.
The Bill also seeks to achieve the following:
- Introduce data protection law with minimum disruption while ensuring necessary change in the way Data Fiduciaries process data;
- Enhance the Ease of Living and the Ease of Doing Business; and
- Enable India’s digital economy and its innovation ecosystem.
- The Bill is based on the following seven principles:
- The principle of consented, lawful and transparent use of personal data;
- The principle of purpose limitation (use of personal data only for the purpose specified at the time of obtaining consent of the Data Principal);
- The principle of data minimisation (collection of only as much personal data as is necessary to serve the specified purpose);
- The principle of data accuracy (ensuring data is correct and updated);
- The principle of storage limitation (storing data only till it is needed for the specified purpose);
- The principle of reasonable security safeguards; and
- The principle of accountability (through adjudication of data breaches and breaches of the provisions of the Bill and imposition of penalties for the breaches).
- The Bill has few other innovative features:
The Bill is concise and SARAL, that is, Simple, Accessible, Rational &Actionable Law as it—
- Uses plain language;
- Contains illustrations that make the meaning clear;
- contains no provisos (“Provided that…”); and
- Has minimal cross-referencing.
- By using the word “she” instead of “he”, for the first time it acknowledges women in Parliamentary law-making.
- The Bill provides for following rights to the individuals:
- The right to access information about personal data processed;
- The right to correction and erasure of data;
- The right to grievance redressal; and
- The right to nominate a person to exercise rights in case of death or incapacity.
For enforcing his/her rights, an affected Data Principal may approach the Data Fiduciary in the first instance. In case he/she is not satisfied, he/she can complain against the Data Fiduciary to the Data Protection Board in a hassle-free manner.
- The Bill provides for following obligations on the data fiduciary:
- To have security safeguards to prevent personal data breach;
- To intimate personal data breaches to the affected Data Principal and the Data Protection Board;
- To erase personal data when it is no longer needed for the specified purpose;
- To erase personal data upon withdrawal of consent;
- To have in place grievance redressal system and an officer to respond to queries from Data Principals; and
- To fulfill certain additional obligations in respect of Data Fiduciaries notified as Significant Data Fiduciaries, such as appointing a data auditor and conducting periodic Data Protection Impact Assessment to ensure higher degree of data protection.
- The Bill safeguards the personal data of children also.
- The Bill allows a Data Fiduciary to process the personal data of children only with parental consent.
- The Bill does not permit processing which is detrimental to well-being of children or involves their tracking, behavioural monitoring or targeted advertising.
- The exemptions provided in the Bill are as follows:
- For notified agencies, in the interest of security, sovereignty, public order, etc.;
- For research, archiving or statistical purposes;
- For startups or other notified categories of Data Fiduciaries;
- To enforce legal rights and claims;
- To perform judicial or regulatory functions;
- To prevent, detect, investigate or prosecute offences;
- To process in India personal data of non-residents under foreign contract;
- For approved merger, demerger etc.; and
- To locate defaulters and their financial assets etc.
- The key functions of the Board are as under:
- To give directions for remediating or mitigating data breaches;
- To inquire into data breaches and complaints and impose financial penalties;
- To refer complaints for Alternate Dispute Resolution and to accept Voluntary Undertakings from Data Fiduciaries; and
- To advise the Government to block the website, app etc. of a Data Fiduciary who is found to repeatedly breach the provisions of the Bill.
Telemedicine – News from India & Abroad
Balancing Precision and Missteps in Cancer Treatment Through ChatGPT
ChatGPT’s capacity to suggest evidence-based cancer therapies is restricted, with accurate and erroneous suggestions intertwined in approximately 33% of its responses, posing challenges in error identification….. Readmore
Is Your Age No Longer a Secret to AI?
Scientists from Osaka Metropolitan University have created an advanced artificial intelligence (AI) system that employs chest X-rays to precisely predict a patient’s chronological age…….Readmore
Harnessing Nanotechnology to Help Treat Blindness
Researchers have harnessed nanotechnology to develop a 3D “scaffold” for growing retinal cells, opening up possibilities for new approaches in treating macular degeneration, a prevalent cause of blindness….Reademore
‘Eye-Opening’ Inaccuracy of ChatGpt Discovered Over Its ‘Eye-ronic’ Medical Advice
A cross-sectional study reveals that an AI chatbot, ChatGPT, provided inappropriate and potentially harmful medical advice about vitreoretinal disease in response to patient questions. ….Readmore


TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TN TSI Newsletter-
- Report can be from 500 to 600 words
- Report Should be relevant to Telemedicine or Medical Informatics
- No promotion of self or any product
- Avoid plagiarism
- All references should be included
- Provide any attributions
- Visuals are welcome including video links
- Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com
Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff
Editors – Dr. Senthil Tamilarasan & Dr. Sheila John
Technical Partner- https://www.medindia.net


































 Faculty Empowerment Program on Telemedicine and Health Care Research
Faculty Empowerment Program on Telemedicine and Health Care Research






 DCGI issues notice to e-pharmacies for online sale of drugs without a license
DCGI issues notice to e-pharmacies for online sale of drugs without a license Satellite to Block Chain – A new paradigm in Covid care delivery through Telemedicine under India’s Health care Mission “Ayushman Bharat“
Satellite to Block Chain – A new paradigm in Covid care delivery through Telemedicine under India’s Health care Mission “Ayushman Bharat“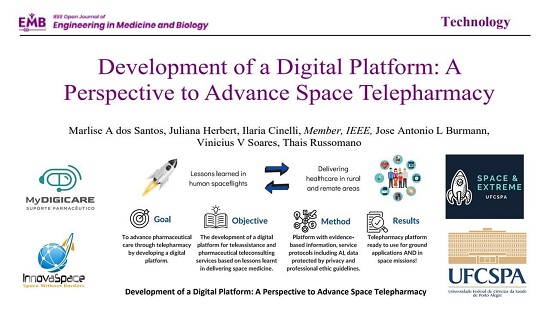

 Telemedicine Workshop for Trauma & Stroke
Telemedicine Workshop for Trauma & Stroke 



 Global Recognition received for Safe Delivery of Tele mental health services following legal and ethical Standards
Global Recognition received for Safe Delivery of Tele mental health services following legal and ethical Standards

 A Journey Into Space
A Journey Into Space
 Virtual healthcare in the new normal
Virtual healthcare in the new normal
 Uttarakhand Chapter of Telemedicine Society of India, inaugurated at AIIMS, Rishikesh
Uttarakhand Chapter of Telemedicine Society of India, inaugurated at AIIMS, Rishikesh


 Digital Health Course Launched by IIM Raipur in collaboration with the Digital Health Academy
Digital Health Course Launched by IIM Raipur in collaboration with the Digital Health Academy