Telehealth Newsletter
Official Newsletter of Telemedicine Society of India

What is New?
We are excited to inform you that TELEMEDICON2024 is rapidly taking shape and will be held in Chandigarh from November 28th to 30th, 2024. We encourage all members to register promptly and take full advantage of the ‘subsidized registration fees’ for this prestigious international event. Stay informed about the latest program updates by visiting our official website – https://www.telemedicon2024.com
Happy to report our TSI member Dr.Haleema Yezdani, has been elected to WHO Federated Digital ID for Sustainable Development (FIDES) committee. In this issue, she writes about how this WHO body seeks to revolutionize the way healthcare is delivered, tracked, and improved using digital identity systems and health data. Dr.Raghavan, our member has been selected as a Fellow of the Society for Biomaterials and Artificial Organs in India and TSI congratulates him.
As the theme of TELEMEDICON is AI in Healthcare and Virtual Clinic we are carrying articles related to these subjects in the next two issues and the first is on the Evolution and History of AI in Healthcare.
On another note, a recurring issue we face is the lack of proper documentation of our events. Despite numerous reminders, many TSI members who dedicate considerable time and effort to organizing their events do not report or share their achievements in our newsletter. This oversight diminishes the visibility of all the hard work being done.
India still lacks a dedicated digital health journal, and for the past four years, our newsletter has been the sole platform available online for the world to witness the progress in the field of digital health within the country. I urge members to reflect on this and consider the importance of documenting and showcasing their contributions.
Finally, don’t forget to start submitting your abstracts for the conference. Wishing everyone happy festivities!
Thank You
Dr. Sunil Shroff
Chief Editor
Vice President, TSI

WHO FIDES: Empowering Global Health through Digital Innovation
Dr. Haleema Yezdani
General Physician, Diabetologist
Vice President, HIMSS India
Consultant, Apollo Sugar Clinic Electronic City Phase 2 Bengaluru
The World Health Organization (WHO) has long been a guiding force in global health initiatives, striving to ensure that every individual has access to the highest standards of healthcare. A significant step towards achieving this vision is the Federated Digital ID for Sustainable Development (FIDES), which seeks to revolutionize the way healthcare is delivered, tracked, and improved upon, using digital identity systems and health data.
WHO FIDES: A Vision for the Future
The WHO FIDES initiative is designed to support the 2030 Sustainable Development Goals (SDGs) by improving the integration of health data across borders, creating robust digital identities for individuals, and fostering more equitable access to healthcare services. FIDES aims to bridge gaps in healthcare, ensuring that marginalized and vulnerable populations are not left behind in the pursuit of universal health coverage.
The vision of WHO FIDES is clear: a world where every individual can securely access their health data, regardless of location, fostering improved health outcomes and greater trust in global health systems. This is achieved through interoperability between systems, data privacy safeguards, and a user-centered approach that empowers patients and health workers alike.
Mission: Transforming Health Systems
The mission of the WHO FIDES project is multifaceted:
- Data Integration and Accessibility: To create an integrated and scalable digital identity system that allows health data to be securely accessed and shared across borders, improving the efficiency of care.
- Equitable Access: To close the gap between different regions and communities, ensuring equal access to health services for all, especially those in underserved areas.
- Sustainability: To establish systems that are not only effective in the short term but are sustainable in the long run, contributing to the health sector’s resilience in addressing global challenges, such as pandemics and health crises.
- Interoperability: To create systems that communicate across various health platforms, ensuring that data is shared seamlessly and securely.
- Empowerment of Individuals: To ensure individuals have control over their own health data, promoting agency and informed decision-making in healthcare.
My Involvement
With my strong background in digital health, telemedicine, data privacy, and healthcare innovation, WHO wanted me to play a role in FIDES. And help in driving forward the project’s mission of equitable healthcare access through digital innovation.
I have always worked for health equity by advocating for vulnerable populations in global health policy forums. My membership in WHO FIDES focuses on ensuring that digital identity systems prioritize patient confidentiality, while also facilitating the efficient exchange of health data to improve patient outcomes.
WHO FIDES continues to explore innovative approaches to digital health, from telemedicine to digital health wallets, ensuring that all individuals have access to the care they need, wherever they are in the world.
Conclusion
The WHO FIDES initiative stands as a pivotal force in transforming healthcare delivery through the power of digital identity and data integration. With a mission aligned with the Sustainable Development Goals and a vision of accessible, equitable healthcare for all, FIDES is shaping the future of health systems globally.
It ensures in merging multiple powerful voices in health care into a single voice under the banner of WHO fides whom everyone can trust.

The Evolution of AI in Medicine: From Early Expert Systems to Modern Breakthroughs
Dr. Sunil Shroff
Vice President, Telemedicine Society of India | Consultant Urologist & Transplant Surgeon
The history of artificial intelligence (AI) in healthcare is a story of innovation, gradual development, and challenges.
It began in the 1960s, when AI’s early focus was on diagnostic support through expert systems such as MYCIN. Over time, the scope of AI has expanded to include areas like predictive modeling, clinical decision support, drug discovery, and administrative tasks, deeply influencing modern healthcare.
Despite these advancements, challenges such as data privacy, ethical concerns, and algorithmic bias persist.
This summary explores the evolution, key milestones, and the future of AI in healthcare.
Early Developments
AI in healthcare took its initial steps during the 1960s with the development of problem-solving programs, specifically expert systems. One of the earliest notable applications was ‘Dendral’, designed for organic chemistry, which paved the way for MYCIN. MYCIN was developed in the 1970s to assist clinicians in diagnosing infectious diseases by recommending antibiotics based on the patient’s symptoms. Alongside MYCIN, systems like INTERNIST-1 and CASNET aimed to help clinicians by providing diagnostic insights, though none of these early systems saw widespread clinical adoption. This lack of adoption was primarily due to the limitations in computing power and the complexity of translating medical knowledge into programmable rules.
Growth of AI in the 1980s and 1990s
The 1980s and 1990s were transformative years for AI in healthcare due to the rise of microcomputers and enhanced network connectivity. During this period, researchers focused on developing AI systems that could operate with incomplete data, thus mirroring the uncertain conditions healthcare professionals often face. Techniques like Fuzzy set theory, Bayesian networks, and artificial neural networks became prevalent. These advancements allowed AI to improve its decision-making processes, particularly in medical fields where data could be ambiguous or incomplete.
AI made its mark in diagnostic pathology through digital pathology tools, enabling the scanning and analysis of microscopy slides to diagnose diseases. This innovation led to AI’s use in diagnosing conditions such as breast cancer, gastric cancer, and hepatitis B. These AI systems not only improved diagnostic accuracy but also reduced the workload for pathologists by automating large-scale data analyses.
Predictive Modeling and Clinical Decision Support
AI in healthcare has seen significant growth in predictive modeling. Algorithms can analyze patient data to predict disease risks and possible outcomes. These predictions are often based on electronic health records (EHRs), which contain a wealth of patient data. For instance, a rule-based AI system could follow decision trees, linking specific symptoms and observations to potential diagnoses.
AI’s ability to use large datasets for predictions has contributed to more personalized medicine, where treatment strategies are tailored to individual patients based on their history and genetic data.
AI has also been instrumental in clinical decision-making. Its role has expanded beyond basic diagnostic aid to include support in emergency departments, where AI algorithms can prioritize cases and reduce wait times by processing data faster than humans.
The 2000s: EHRs and Telehealth Integration
The 2000s marked a critical turning point for AI in healthcare, particularly with the growing adoption of electronic health records (EHRs). The widespread use of EHRs facilitated the integration of AI systems into clinical workflows, providing a vast pool of data for analysis. AI algorithms began using EHRs to predict treatment outcomes, detect disease patterns, and even recommend care plans tailored to patient needs.
AI also began to enhance telehealth services, making healthcare more accessible, especially in remote areas. Through telemedicine, AI-supported platforms allowed real-time monitoring of patient health, creating opportunities for remote diagnosis and consultation. This integration was especially useful during the COVID-19 pandemic, as the need for virtual healthcare delivery grew.
Ethical Challenges and Regulatory Concerns
Despite the promising advances, AI in healthcare faces significant ethical challenges. A key concern is the lack of transparency in AI decision-making processes, often referred to as the black box problem. Clinicians may hesitate to trust AI recommendations if they cannot understand how the AI arrived at its conclusions. Moreover, algorithmic bias poses another challenge. AI systems are only as unbiased as the data they are trained on, and datasets lacking diversity can lead to biased outcomes that disproportionately affect underrepresented populations.
Data privacy is another critical issue. With the vast amounts of patient data needed to train AI systems, safeguarding this information is paramount. Stricter data protection regulations, such as GDPR in Europe and HIPAA in the U.S., are necessary to ensure patient confidentiality. Regulatory frameworks must also evolve to address the liability concerns that come with AI-driven clinical decisions.
Recent Developments and Future Directions
Recent years have seen exponential growth in the application of AI technologies in healthcare. ‘Machine learning’ (ML) and ‘deep learning’ (DL) models, such as convolutional neural networks (CNNs), have significantly improved diagnostic accuracy in areas such as ‘medical imaging’. AI now assists radiologists in detecting anomalies in X-rays and MRIs, speeding up diagnoses and reducing human error.
AI has also made breakthroughs in ‘drug discovery’. Algorithms can rapidly analyze molecular structures and predict how new drugs might interact with biological systems. This capability has the potential to shorten the drug development cycle and lower research costs. AI-driven drug development was notably accelerated during the COVID-19 pandemic, when researchers used predictive models to identify possible treatments.
In the field of ‘robotic surgery’, AI has enabled more precise, minimally invasive procedures. Robots guided by AI can perform delicate surgeries with a level of precision that surpasses human capabilities. Additionally, AI-powered prosthetics and rehabilitation technologies have improved patient outcomes in post-operative recovery and physical therapy, enhancing mobility and independence.
Future Trends and Implications
Looking ahead, AI is expected to play an increasingly central role in healthcare delivery. The integration of ‘precision medicine’—which uses patient-specific data to tailor treatments—will become more widespread as AI systems become better at analyzing complex genetic, lifestyle, and environmental factors. In ‘telehealth’, AI-driven tools like Chabot’s and personalized health information will continue to improve patient-provider communication and enable more effective monitoring of chronic conditions.
However, to realize AI’s full potential in healthcare, ‘collaborative ecosystems’ between healthcare providers, AI developers, and regulatory bodies are essential. Interdisciplinary partnerships will be needed to address both technological and ethical challenges, fostering a smoother integration of AI into daily healthcare practice.
Conclusion
The history of AI in healthcare is one of continuous progress, characterized by groundbreaking innovations and critical challenges. From its early beginnings with diagnostic tools like MYCIN to its current applications in telemedicine, robotic surgery, and drug discovery, AI has transformed healthcare practices. However, as AI becomes more embedded in healthcare, ethical concerns, data privacy issues, and the need for regulatory oversight will remain crucial. As the technology evolves, striking a balance between innovation and patient safety will be key to ensuring that AI improves both medical practices and patient outcomes.

14th HealthCare 360 Summit 2024
Rajarajan S
Group Chief Operating Officer, Alluri Sitarama Raju Academy of Medical Sciences
The 14th HealthCare 360 Summit 2024, held on 27th September 2024 at the Radisson Blu Hotel, Chennai, was an outstanding gathering of over 150 senior healthcare professionals. Organized by ET Business Consulting, the summit provided a robust platform for industry leaders to engage in deep discussions on the current and future state of healthcare, with a special emphasis on emerging trends and technological advancements. The event saw participation from top healthcare executives, thought leaders, and decision-makers, all aiming to reshape the healthcare ecosystem for a more resilient and patient-centric future.
Event Highlights
Opening Session
The summit commenced with a Keynote Address and Welcome Speech at 9:30 AM, setting the tone for the day. It was followed by a series of meticulously curated panel discussions and networking opportunities. The opening sessions framed the central theme of the event: “Healthcare Vision 2024-2030: Designing, Planning, and Executing the Future of Hospitals.” This session, which ran from 10:00 AM to 11:00 AM, explored the strategic outlook for the healthcare sector in India over the next decade, including plans for integrating cutting-edge technologies with patient care to elevate hospital operations.
Panel Discussions
The summit featured a diverse lineup of panel discussions, each addressing critical aspects of the healthcare sector:
1. Healthcare Vision 2024-2030: Senior executives, including Dr. Ilankumaran Kaliamoorthy (CEO, Rela Hospital) and Mr. Rajarajan S (Group COO, ASRAM) and Mrs. Monika Kejriwal Director – Healthcare, RSP Design Consultants (India) Pvt. Ltd. and, contributed their insights on how hospitals can prepare for the future by focusing on innovation and sustainability.
2. Profitability, Social Responsibility, and Clinical Care in Private Hospitals: Held between 11:00 AM to 11:45 AM, this panel delved into the challenges of balancing financial sustainability with ethical medical practices. Executives from KG Hospital, MGM Healthcare, and others shared their perspectives on how healthcare institutions can maintain high clinical standards while staying financially viable.
3. Exploring New Models in Healthcare Delivery: Moderated by Mr. Rajarajan S Group Chief Operating Officer Alluri Sitarama Raju Academy of Medical Sciences and Dr. Suresh Vishwanathan (Managing Director, SKS Hospital), this session at 12:40 PM to 1:30 PM explored alternative delivery models in healthcare, such as telemedicine, home healthcare, and mobile health units, offering a glimpse into the future of healthcare access in both urban and rural areas.
4. Tech Revolution in Healthcare: The final panel, from 2:30 PM to 3:30 PM, focused on the latest technological trends, including cloud computing, data security, artificial intelligence (AI), and the Internet of Medical Things (IoMT). Mr. Venkata Phanidhar (CEO, Medway Hospitals) and Dr. Stephen Mathew (COO, Sringeri Sharada Equitas Hospital) highlighted the role of AI in optimizing patient care and improving operational efficiency.
Networking Opportunities
The summit offered structured networking breaks, including a speed networking session from 3:30 PM to 4:00 PM, which allowed participants to establish meaningful connections with industry peers. These interactions fostered collaboration and cross-pollination of ideas among hospital leaders, architects, technologists, and consultants.
Key Takeaways
1. Sustainability and Innovation: The overarching theme was the need for sustainability-driven innovations in hospital infrastructure and operations, with an emphasis on energy efficiency, patient safety, and clinical outcomes.
2. Balancing Profitability and Care: Executives stressed the importance of finding equilibrium between profitability and ethical healthcare delivery, ensuring that patient welfare remains at the forefront of healthcare strategies.
3. Technology as a Catalyst: The consensus was clear—technology will play a pivotal role in transforming healthcare delivery models. From AI to IoMT, digital tools are seen as critical for enhancing both clinical and operational processes in the years ahead.
4. Patient-Centered Approaches: Several discussions highlighted the shift toward patient-centered care, with hospitals focusing on personalized services, data-driven decision-making, and remote care models to meet evolving patient needs.
Conclusion
The 14th HealthCare 360 Summit 2024 was a resounding success, bringing together a formidable array of healthcare leaders committed to shaping the future of the industry. The exchange of knowledge, ideas, and solutions during the summit underscored the importance of collaboration in navigating the challenges ahead. The event not only provided deep insights into the direction healthcare is heading but also created a solid foundation for future initiatives that will define the next era of hospital and healthcare excellence.
The event concluded with closing remarks at 4:00 PM, leaving attendees inspired and motivated to implement new strategies within their respective organizations.



Join Us for the Next Healthcare Summit 2024: Innovating for a Healthier Future
We are excited to announce the Healthcare Summit 360 2024,Bengaluru, where industry leaders, innovators, and professionals will come together to shape the future of healthcare! This year’s theme, “Transforming Healthcare Delivery through Innovation,” will focus on cutting-edge technologies, new care models, and solutions to improve patient outcomes, accessibility, and hospital efficiency.
Event Details:
Date: [06.12.2024]
Location: Bengaluru
Theme: Transforming Healthcare Delivery through Innovation
Audience: Healthcare professionals, hospital administrators, technology experts, policymakers, and investors.
Key Topics:
Hospital Infrastructure & Technology: How IoT, AI, and Smart Hospitals are changing the landscape.
Telemedicine and Virtual Care: Revolutionizing healthcare delivery for patients everywhere.
Healthcare Delivery Channels: Innovative models like mHealth, home care, and retail clinics.
Data-Driven Healthcare: Harnessing Big Data and AI for better patient outcomes.
Patient-Centered Care: Delivering healthcare that’s accessible, efficient, and personalized.
Why Attend?
Network with top healthcare leaders and innovators
Gain insights from cutting-edge case studies and expert panels
Explore emerging technologies that are reshaping the healthcare industry
Collaborate on solutions to the most pressing challenges in healthcare delivery
Speakers:
We’ll feature a lineup of renowned speakers, including:
Mr. Rajarajan Sathymurthy, COO, Alluri Sitarama Raju Academy of Medical Sciences
Dr. Vijay, Partner Integra Ventures
Mr. Deepu Prakash, Managing Partners Aedium Design
Mrs. Monika Kejriwal Director Healthcare Director, RSP Design Consultant India
Who Should Attend?
This summit is designed for healthcare executives, hospital administrators, physicians, technologists, policy makers, and anyone passionate about advancing healthcare delivery through innovation.
How to Register:
Visit https://etbusinessconsult.com/register to secure your spot today.
Early bird registration discount are available until 6:11:2024
Let’s work together to innovate, collaborate, and build a healthier tomorrow!
::ANNOUNCEMENTS::

Professor S. Raghavan Elected as a Fellow of the Society for Biomaterials and Artificial Organs, India
Professor S. Raghavan is elected as FBAO in recognition to his lifetime contributions in the area of biomedical engineering, biomaterials, bioMEMS and Nano materials, as evident from his research publications and relevance to patient care technologies.
TSI congratulates Prof Raghavan for this prestigious honor.

To Register for the conference visit https://www.telemedicon2024.com/


To know more about CAHOTECH 2024 visit
https://www.linkedin.com/posts/nostethbutscope_cahotech24-blr-hospinnov-pitchfest-delegate-activity-7225805311683485696-Nkg0
Telemedicine – News from India & Abroad
AI-Powered Systems Sets a New Frontier in Hospital Patient Care
Artificial intelligence ( AI) can help reduce unexpected deaths in hospitals by accurately identifying patients at high risk of health deterioration as per research published in CMAJ…….. Read More
AI-Powered Tutors: A New Era in Brain Surgery Training
Neurosurgery is a demanding field where precise surgical skills are crucial for patient outcomes. While surgical errors are uncommon, they can have severe………. Read More
Stay Energized in a World of Videoconferences
With videoconferencing still a major part of life post-pandemic, as people work remotely, socialize online, and attend virtual events…… Read More
Beyond the Human Touch: The Rise of Robotic Surgery in Orthopedics
Robots have often been portrayed negatively in science fiction and the public imagination, even by the people who invented them……… Read More
Telemedicine Practice Guidelines – A Foundation Course for RMPs by TSI Faculty
To know more about the Telemedicine Foundation Course click on the link below:
https://tsitn.org/tpg-course/
TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TSI Newsletter-
- Report can be from 500 to 600 words
- Report Should be relevant to Telemedicine or Medical Informatics
- No promotion of self or any product
- Avoid plagiarism
- All references should be included
- Provide any attributions
- Visuals are welcome including video links
- Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com
Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff
Editors – Dr. Senthil Tamilarasan & Dr. Sheila John
Technical Partner- https://www.medindia.net










































































































 9. Himachal Pradesh Chapter on May 13, 2023: With active support and lead role by Dr. Vikrant Kanwar of AIIMS Bilaspur and wishes of Dr. Vir Singh Negi, Executive Director AIIMS, Bilaspur, the HP chapter was inaugurated on May 13, 2023. This is personally special and dear to me as this is my birthday celebrated in a satisfying way with the inauguration of a new chapter in an important hilly state of India. Dr. Vikrant also came to Telemedicon2022 at Goa and joined a parallel meeting with me along with Dr Arti Pawaria of Haryana and got motivated to form a state chapter and continued the work soon after going back. Another pleasant news is the state chapter soon after formation has come forward to host 2024 Telemedicon at HP in Dharamshala (Kangda) in Nov 2024 which was ratified by the 2023 AGM.
9. Himachal Pradesh Chapter on May 13, 2023: With active support and lead role by Dr. Vikrant Kanwar of AIIMS Bilaspur and wishes of Dr. Vir Singh Negi, Executive Director AIIMS, Bilaspur, the HP chapter was inaugurated on May 13, 2023. This is personally special and dear to me as this is my birthday celebrated in a satisfying way with the inauguration of a new chapter in an important hilly state of India. Dr. Vikrant also came to Telemedicon2022 at Goa and joined a parallel meeting with me along with Dr Arti Pawaria of Haryana and got motivated to form a state chapter and continued the work soon after going back. Another pleasant news is the state chapter soon after formation has come forward to host 2024 Telemedicon at HP in Dharamshala (Kangda) in Nov 2024 which was ratified by the 2023 AGM.

 11. Jharkhand Chapter on Aug 18, 2023: With active support and membership drive by Dr.Maishraj of AIIMS Deogarh, the Jharkhand chapter of TSI was inaugurated on Aug 18, 2023 under the aegis of President TSI Dr. Meenu Singh and Dr. Saurabh Varshney, Director AIIMS.
11. Jharkhand Chapter on Aug 18, 2023: With active support and membership drive by Dr.Maishraj of AIIMS Deogarh, the Jharkhand chapter of TSI was inaugurated on Aug 18, 2023 under the aegis of President TSI Dr. Meenu Singh and Dr. Saurabh Varshney, Director AIIMS.

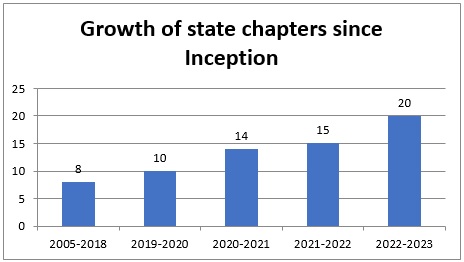
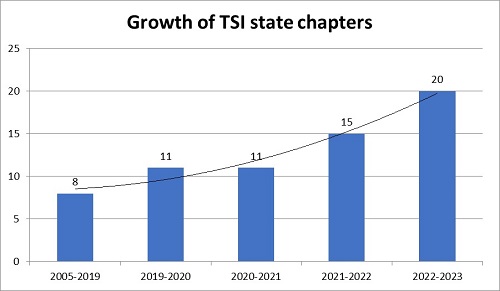 Though the growth of state chapters across the regions is increasing and pleasant to be noted, more and more activities are expected to be taken up under the aegis of these chapters with active participation by more members and particularly the younger generation. While conducting online/offline seminars and workshops or trainings is an initial and minimal activity to be taken up, the next and expected step in the journey is conducting some remote/rural camps with real usage and utilization of Telemedicine in practice.
Though the growth of state chapters across the regions is increasing and pleasant to be noted, more and more activities are expected to be taken up under the aegis of these chapters with active participation by more members and particularly the younger generation. While conducting online/offline seminars and workshops or trainings is an initial and minimal activity to be taken up, the next and expected step in the journey is conducting some remote/rural camps with real usage and utilization of Telemedicine in practice.



 Quiet unexpectedly but most pleasantly, the state chapter within a period of 9 months from the formation, came forward to successfully host the mid-term conference of 2022 on Aug 26, 2022 again at the prestigious SKIMS. The participation of several young doctors and particularly students and their presentation of high quality research papers was an added attraction in the mid-term conference.
Quiet unexpectedly but most pleasantly, the state chapter within a period of 9 months from the formation, came forward to successfully host the mid-term conference of 2022 on Aug 26, 2022 again at the prestigious SKIMS. The participation of several young doctors and particularly students and their presentation of high quality research papers was an added attraction in the mid-term conference.