Advancing Telepathology: Experience from a Tertiary Care Centre of Excellence
Brijdeep Singh*, Uma Nahar Saikia, Harpreet Kaur, Biman Saikia, Amit Agarwal, Nainesh Joshi
Department of Telepathology, Postgraduate Institute of Medical Education and Research, Chandigarh
brijdeep@gmail.com
Aims and Objectives: To assess the implementation of Telepathology services at PGIMER-Centre of Excellence for Telepathology, Department of Telemedicine, launched on November 1st, 2023.
The study outlines the methodology, case diversity, platforms used, and the impact on diagnostic efficiency and accessibility.
Methodology: Telepathology services are delivered through three platforms: email submissions, the GOI’s e-Sanjeevani portal, and Onward Assist Telereporting system, a private enterprise specializing in Telepathology and AI solutions. These services offered free during a One year trial period, receive cases from Punjab, Haryana, Himachal Pradesh and New Delhi. Referring pathologists submit photomicrographs, videos, along with detailed requisition forms. A Telepathology (TP) number is assigned after verifying image quality. The targeted turnaround time is 24-48 hours post-assignment of the TP number. A digital report is generated for each case.
Results: A total of 380 Telepathology consultations have been conducted, with 285 cases (75%) from private hospitals and 95 cases (25%) from government institutions. The subspecialties covered include Ocular Pathology (102/380), Head and neck pathology (56/380), Dermatopathology (55/380), Gastrointestinal Pathology (41/380), Gyanepathology (21/380), Pulmonary Pathology (16/380), Neuropathology (13/380), Musculoskeletal Pathology (12/380) Genitourinary Pathology (10/380), Breast Pathology 10/380), Cytopathology (33/380) and others. 12 cases were initially deemed unsatisfactory due to poor image quality but were later reported upon receiving better images. Comprehensive diagnoses were rendered in 90% (340) of cases, while 10% (40) required descriptive reports due to insufficient diagnostic material or inadequate information.
Conclusion: Telepathology is a transformative tool in digital pathology, enabling expert opinions across wide geographic regions, reducing turnaround time, and facilitating remote teaching and training. It significantly enhances diagnostic accuracy, improves clinical management, and contributes to better healthcare outcomes.
*************************************************
Revolutionizing Home Healthcare: Smartphone -Based Video-Electroencephalography for Neurological Disorders
A Kumar* , A Kadambi
Director – Mocxa Health Private Limited
ankita.kumar@gmail.com
Aim: Despite the established advantages of home-based long-term Electroencephalography (EEG) monitoring, with studies demonstrating a 72% sensitivity compared to only 11% for routine EEGs in detecting abnormalities (Hernandez-Ronquillo et al., 2023; Beckerman et al., 2013), there is no availability of home based monitoring in India. This study aimed to evaluate the feasibility and effectiveness of a novel smartphone-based video EEG system for conducting home EEG procedures in India.
Methods: Twenty patients were referred for home EEG monitoring by neurologists in Bengaluru. Qualified EEG technologists performed the setup including electrode placement at patients’ homes. They also remotely monitored EEG quality during the procedure and collected data upon completion. A qualified epileptologist remotely reviewed and interpreted the EEG data and provided the final diagnosis and recommendations.
Results: The smartphone-based system proved highly feasible, with patients successfully undergoing procedures in the comfort of their homes. The system’s user-friendliness and convenience reduced the need for frequent in-clinic visits.Key benefits of home EEG monitoring include improved access to neurological care, early detection of seizures or other neurological events, and reduced healthcare costs.
Conclusion: This study highlights the potential of smartphone-based video EEG systems to revolutionize neurological care in India by enhancing patient outcomes and improving efficiency.
*************************************************
Improving Thyroid Nodule Evaluation Using Deep Learning and Ultrasound Imaging
Jatinder Kumar*, Devi Dayal
PGIMER, Chandigarh
kumar.jatinder@pgimer.edu.in
Introduction: The thyroid is a small, butterfly-shaped gland in the neck that produces hormones essential for regulating various metabolic processes. Common thyroid conditions include thyroid nodules abnormal growths or lumps within the thyroid as well as hypothyroidism and hyperthyroidism.
Methods– Thyroid ultrasonography (USG) imaging is widely used to detect and categorize thyroid abnormalities, which can significantly impact metabolism and overall health. Advances in artificial intelligence (AI), especially deep learning (DL), have enabled the identification and analysis of patterns in clinical images due to DL’s ability to extract hierarchical feature representations from images without the need for annotated data. Accurate identification of malignant thyroid nodules, distinguishing them from benign ones, is crucial in reducing unnecessary fine needle aspiration (FNA) procedures. This study presents a technique for thyroid nodule detection in USG images using DL for feature extraction. Two pre-trained DL models ResNet-18 and VGG-19 were fine-tuned for classifying thyroid USG images. Both models were trained and tested on the Digital Database of Thyroid Ultrasound Images (DDTI), a gold standard dataset.
Results showed classification accuracies of 97.13% for ResNet-18 and 90.31% for VGG-19, with ResNet-18 demonstrating superior performance in classification accuracy over VGG-19.
*************************************************
Tele-Ocular Pathology: Evaluating Remote Diagnostic Accuracy through Email Submissions
Brijdeep Singh*, Uma Nahar Saikia, Arpan Gandhi, Nainesh Joshi, Biman Saikia
Department of Telemedicine, Post Graduate Institute of Medical Education and Research, Chandigarh
brijdeep@gmail.com
Aims and Objectives– This study evaluates the effectiveness and diagnostic concordance of ocular pathology cases from over 400 telepathology referrals received at PGIMER, Chandigarh’s Centre of Excellence in Telepathology at the Regional Resource Centre (North). The study highlights how email-based telepathology supports rapid, high-quality diagnostics, enhancing patient convenience and clinical decision-making.
Methodology– A retrospective analysis of 104 ocular pathology cases reviewed from November 1st 2023 to October 31st 2024, was conducted. The workflow included an initial assessment of image quality for photomicrographs, clinical images, and videos for quality and reportability, with follow-ups as needed for optimization. Each case was assigned a TP number and categorized by diagnostic parameters to establish concordance between the provisional diagnosis of the referring pathologist and the final telepathology report. Ancillary tests such as special stains and immunohistochemistry (IHC), were recommended, as required, to enhance diagnostic accuracy.
Results– Among the 104 ocular telepathology cases analysed, 67 (64.4%) were neoplastic (36 malignant, 31 benign) and 37 (35.6%) were non-neoplastic. Topographic distribution included 32 eyelid, 29 conjunctiva, 13 enucleation, 13 orbit, 8 lacrimal gland, and 8 other cases. Concordance between the provisional and final diagnoses was achieved in 79.8% of cases, underscoring the reliability of this model. Static images sometimes proved limited, particularly in enucleation cases, where video submissions provided crucial diagnostic context. On average, each case included 7.4 photomicrographs, 1.8 clinical images, and 1.65 videos. Recommendations for ancillary tests were provided selectively. The model achieved an average turnaround of 12-18 hours, providing significant time and cost savings for patients and aiding therapeutic decision making.
Conclusion– Email-based ocular telepathology presents a robust and efficient model for remote diagnostics, delivering high diagnostic concordance and substantial patient benefits. This framework establishes a standard for image quality and reporting formats, ensuring high-quality diagnostic support across remote and underserved areas.
*************************************************
Serious Games in Healthcare: A New Frontier for Indian Healthcare Innovation
Gaurang Baxi*, Kamakshi Baxi
Game Designer Volunteer, Friends N Smile Foundation
baxigaurang@outlook.com
Serious games, designed with the purpose of addressing real-world issues through interactive gameplay, incorporate educational, therapeutic, and motivational elements to positively impact health behaviors and encourage healthy lifestyles. In the context of healthcare, serious games offer a unique opportunity to revolutionize the sector by making health-related tasks both engaging and educational. With India’s rapidly expanding digital reach and gaming industry, the healthcare sector presents fertile ground for serious games. Serious games in healthcare have been applied previously in various clinical trials as an intervention, where they were proved to be effective in a variety of diseases such as cancer, asthma and mental health disorders. However, challenges persist, including the need for culturally sensitive design and the active involvement of healthcare professionals in development, which is crucial for ensuring credibility and effectiveness. In India, serious games face additional hurdles such as regional diversity and cultural norms. Nevertheless, the potential for growth is significant, with India poised to become a leading hub for digital health games, spurred by increased internet access, the advent of 5G, and evolving consumer behaviors. The Indian government’s support for the gaming industry, including 100% foreign direct investment, further bolsters growth prospects. To fully leverage the potential of serious games in Indian healthcare, strategies must be culturally relevant and socially acceptable to ensure their impact. With thoughtful implementation and increased collaboration between the healthcare and gaming industries, serious games can help with improving level of knowledge, changing behaviours, improving motor skills and managing emotions.
*************************************************
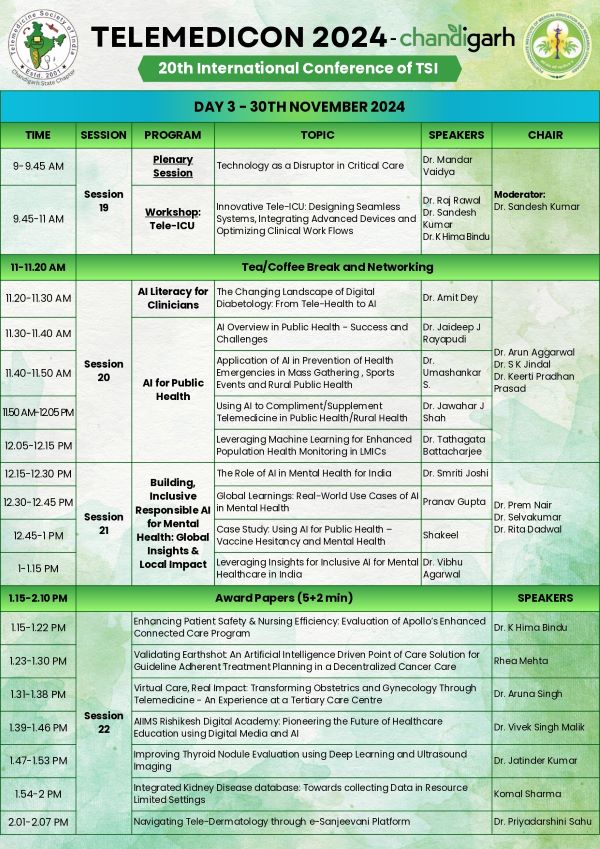
The first survey on nurses knowledge attitude and practice on connected care monitoring in wards
K Hima Bindu*, Sai Praveen Haranath, Manohar Prasad, Ananthalakshmi
Apollo Hospitals, Jubliee Hills, Hyderabad
himabindukotamarthy@gmail.com
Introduction: Enhanced Connected Care (ECC) is transforming healthcare by integrating technology to advance patient monitoring and safety. Through continuous tracking of vital signs—heart rate, blood pressure, Saturation, temperature, and respiratory rate—medical devices transmit data to a nursing station dashboard, enabling prompt nurse response. Nurses play a vital role in detecting early signs of patient deterioration, making their knowledge, attitudes, and practices (KAP) critical to ECC’s success and effective patient care.
Aim of the Study: To evaluate confidence in using ECC technologies, time savings, perceived benefits and challenges, and the need for further training.
Results: The study surveyed 125 participants involved in ECC care, with 61% rating their confidence as 10/10 in using ECC technologies. Younger nurses (18-34 years) showed higher confidence, and increased nursing experience was significantly correlated with higher confidence. ECC monitoring saved 5-10 minutes per shift for 47.2% of respondents, with more than 10 minutes saved mostly during night shifts. A significant correlation was found between knowledge and confidence (p=0.009).
Discussion: Lower confidence levels among nurses aged 35-44 indicate a need for targeted support through workshops or additional training to enhance their comfort with ECC technology. The positive link between knowledge and confidence suggests that regular training could enhance nurses’ proficiency with ECC tools. Greater time savings were noted during night shifts, aligning with the increased need for continuous monitoring during non-peak hours. Alarm fatigue was reported by 42% of ECC-using staff.
Conclusion: This study shows ECC technology’s broad use and perceived benefits in improving patient outcomes. Nurses view ECC as a valuable tool that saves time, allowing for more direct patient care rather than manual vitals recording. Nonetheless, challenges remain. Targeted workshops, support teams, and improved resources could further support ECC integration in healthcare practice.