Click Here to Download PDF Version

Telehealth Newsletter
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
| What is New?
This issue reports the highlights of the annual conference of Indian Society of Lifestyle Medicine. A society that will play stellar role in the development of tele-health space. Tele-health is ideally placed to treat most of the Non-Communicable disease that now makes up the major reason for morbidity and mortality of our global population. TSI itself is now undertaking the amendment of its constitution after 20 years, all members should contribute to this endeavour by sending their recommendations to our hon secretary. We finish another year of uncertainty with the Omicron variant. From the editors of this newsletter our best wishes for a safe and happy holiday season and a very happy and healthy 2022 to all TSI members. Thank You |

 ‘A Paradigm Shift in Healthcare’ theme of the Second annual conference of Indian Society of Lifestyle Medicine
‘A Paradigm Shift in Healthcare’ theme of the Second annual conference of Indian Society of Lifestyle Medicine
Dr. Ravi Modalli
Treasurer, Indian Society of Lifestyle Medicine
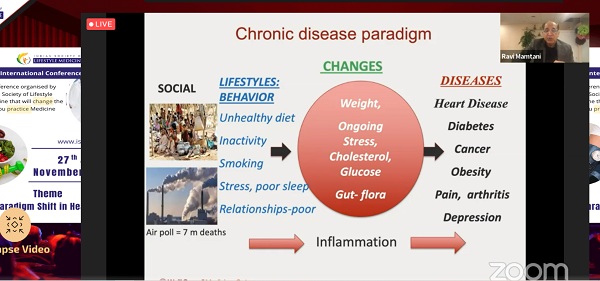
The second International Conference i.e. ISLM2021 was conducted on the 27th and 28th November 2021 by Indian Society of Lifestyle Medicine (ISLM – www.islm.org.in). Under the conference theme ‘A Paradigm Shift in Healthcare’, deliberations of ISLM2021 established the value of Lifestyle Medicine in bending the trajectory of healthcare towards positive health and well-being among physicians, their patients & people in general.
Dr. Ravinder Mamtani, MBBS, MD, MSc, FACPM, FACOEM, ABoIM, DipABLM, Prof of Population Health Sciences, Weill Cornell Medical College, NY, USA, in his key note message extended his full support to ISLM leadership & highlighted that reforms of modern healthcare must hold it’s progressive path by adopting lifestyle medicine approaches to control the burden of lifestyle diseases and reduce the incidence of premature deaths. Lifestyle medicine offers a breath of fresh air. Providing patient-centred evidence based lifestyle medical care, when warranted, is a step in the right direction. He summarised saying ‘This year’s ISLM2021 conference on changing the paradigm of healthcare will shed light on how lifestyle medicine can positively impact healthcare delivery in India.
Ms. Preetha Reddy, Executive Vice Chairperson, Apollo Hospitals Group, in her key-note message commended the organisation of ISLM2021 and prompted the entire medical fraternity to champion the healthy way forward and mitigate the burgeoning threat of lifestyle related chronic diseases, thereby contributing to the making of a healthy economy.
Dr. Sheela Nambiar, President, ISLM, presented the conference theme of ISLM2021 highlighting ISLM’s approach to reduce burden of the already overloaded healthcare system & making care systems more conducive to wellbeing and quality life for physicians and their patients.
She spelt ISLM’s 8 point vision:
1. To educate medical students on principles and practices of Lifestyle Medicine
2. To motivate and inspire young physicians to adopt health promotion & personal protective practices including preventive medicine using lifestyle modifications
3. To create strategic alliances between healthcare systems and other organizations, corporates, communities, companies and interested individuals to help the cause of ‘health promotion’, ‘disease prevention & control’ and improved longevity using the principles of Lifestyle Medicine.
4. To continue collaborating with senior physicians in India who are integrating lifestyle medical protocols in their clinical practices.
5. To establish standards of education and service protocols for Lifestyle Health Management.
6. To amass more indigenous research, improving the understanding of our own population and better control of lifestyle related diseases.
7. To take social responsibility by educating people on healthy choices & empower control on their personal health.
8. To make India a forerunner to contend with global movement of Lifestyle Medicine in lines with Sustainable Developmental Goals
Over 40 speakers including Padmashrees, Padmabhushans, Academicians & Practitioners of International repute shared evidence on alignment of Lifestyle Medicine with over 22 topics of mainstream clinical disciplines like Endocrinology, Gastroenterology, Gynaecology, Paediatrics, Oncology, Cardiology, Neurology, Psychiatry, Adolescent Medicine, Obesity, COVID19 care, Sleep medicine, etc.
Dr. Sunil Shroff, Renowned Urologist, Transplant Surgeon & President, TN – Telemedicine Society of India, enlightened on the prospects of delivering lifestyle medical care through tele-health & tele-medicine especially on reaching the masses, keeping people engaged in personal health & also enabling long-term treatment follow-ups. Tamil Nadu Medical Council permitted CME credit hours for the conference.
The conference also featured two workshops on Stress Management and Culinary Medicine. Participants enjoyed the morning exercise sessions. Series of virtual networking meets allowed attendees to interact with the faculty, discussing topics of interest like Telemedicine, Mindfulness, Principles of Lifestyle Medicine, Nutrition, Obesity, Positive Psychology. A panel discussion on Lifestyle Medicine in Clinical Practice brought forth the experiences of leading Lifestyle Medicine Physicians in India.
Thirty physicians and licensed dietitians appeared for the certification examination conducted by the International Board of Lifestyle Medicine through ISLM. Scores of researchers participated in the research presentations highlighting the adoption of principles of lifestyle medicine in mainstream healthcare.
Lifestyle Medicine, being a vital clinical area of work promoted by the Indian Society of Lifestyle Medicine, the new members joining ISLM enjoy continued learning opportunities through the monthly academic & research activities of ISLM.
A world full of compliments for ISLM2021, sponsors messages, abstracts, recipes are captured in the form of a souvenir that is accessible at www.islm.org.in


 ISO 13131 Certification for Telehealth Services
ISO 13131 Certification for Telehealth Services
Prof. K. Ganapathy
Past President, Telemedicine Society of India & Neurological Society of India | Hon Distinguished Professor The Tamilnadu Dr MGR Medical University | Emeritus Professor, National Academy of Medical Sciences | Formerly Adjunct Professor IIT Madras & Anna University | Director Apollo Telemedicine Networking Foundation &, Apollo Tele Health Services | URL: www.kganapathy.in
December 10th 2021 is indeed a Red letter day for Indian Telehealth. On this day the ISO 13131-2021, certification for Telehealth Services was obtained for the first time anywhere, by Apollo Telehealth Services . This brief note points out the necessity for raising the bar and setting high standards, so that the world will strive to achieve India class.
For decades, Telemedicine/Telehealth services was not centre stage in the healthcare delivery system. COVID-19 changed this. The world has now accepted that the forced lockdown- enforced acceptance of Remote Health Care will become the new normal even after the pandemic is de notified. Universal acceptance, increases the responsibility of all health care providers deploying technology, to ensure constant high quality while bridging the urban rural health divide.
Quality is never an accident. It is always the result of deliberate intention, sincere effort, intelligent direction and skillful execution. Though Henry Ford opined that quality means doing it right when no one is looking, in the real world this is difficult to implement. ISO certification ensures that “Big Brother” is watching all the time. The necessity for re certification is like the Sword of Damocles hanging above us. However it drives home the message that Quality is everyone’s responsibility at all times and not during the audit alone. One has to keep running to stay where you are. To maintain the initial global recognition, maintaining quality needs to become a habit, a unique opportunity to transform one’s DNA if necessary!! Success is the sum of small efforts, repeated day-in and day-out. Standardising systems, processes, documentation and re documentation alone will ensure providing quality remote healthcare for anyone, anytime anywhere.
International Organization for Standardization (ISO) – An OVERVIEW
The, International Standards Organization, TC 215 Health Informatics Committee developed a Technical Specification, ISO/TS 13131 Telehealth services, based on a risk and quality management approach. This standard, supports healthcare planning, service and workforce planning, organization responsibilities, financial and IT management. ISO was established in 1947 in Geneva, Switzerland. An Independent, non-governmental international organization it develops standards that are recognized and respected globally. It brings experts together to improve quality and provide world-class healthcare services. Experts are from 166 national standard bodies. ISO standards are developed by various advisory groups. Presently ISO has 255 technical committees, 515 subcommittees, and 2498 working bodies. Since 1947, ISO’s technical experts have created more than 18,800 standards for all possible business. ISO standards ensure that administration and product/work flow systems are carried out legally, safely and effectively. ISO technical experts have developed several assessment protocols to ensure that certified organizations apply these guidelines in their workplace. The approved protocols aid organisations to ensure that their frameworks, devices and workforce are actually in compliance with ISO standards. ISO 13131 provides recommendations on guidelines for Telehealth services deploying Information and Communication Technology (ICT) to deliver quality healthcare services.
Implementing ISO/TS 13131 means facilitating cooperation and interoperability of its different health systems to ensure quality telehealth services. It also ensures a reliably high standard of service, irrespective of where a person lives, across the globe. This standard provides guidelines for developing quality plans and managing company resources, while putting the right policies in place to safeguard clients’ private data. Securing ISO 9001 for quality management and ISO 27001 for information security management reduces the complexity involved in getting the IOSO 13131 branding. Realising that excellence is always a moving target it was the logical next step in the company’s journey to go (to paraphrase Captain Kirk of Star Trek)“ where no Man had ever gone before”.
The decision to get certified though it was time consuming, labor intensive and expensive was the determination to set a benchmark for the whole telehealth sector. A leading market player faced with competition, the company needed reassurance that its high-quality standards would provide a stamp of recognition and help distinguish it from its competitors. As a pioneer in the field, it was important to set the conditions of competition, to prevent some potentially harmful practices of others, from compromising the reputation of all. Considering the high risks involved in securing patients’ data privacy, it was crucial for the organization to be sure it’s IT systems and processes were stringent, fulfilled the highest expectations in this sensitive sector and conformed to security legislation.. A preliminary gap analysis was conducted and where ISO/TS 13131 provided more specific criteria than the ones actually in place, these were ear marked for improvement. Consumers draw confidence from the stringent certification process. ISO standards will help organisations comply with new regulatory requirements, enhancing efficiency of internal processes and quality of remote health services provided. Documenting the much needed framework necessary for supply of services, improves value of the product. The more diverse and competitive the market, the more guidance consumers need, to be sure they are purchasing the service they want at the best price. International Standards helps maintain a healthy competition in the marketplace.
We need to identify the right quality metrics, and ensure that the information is readily available to patients, health systems and providers themselves. Consumers should be helped to gauge telehealth providers, and provide healthcare workers/systems with feedback for continuous improvement. Best practices for virtual care need to be standardised, notified and applauded so that it will be increasingly sought after. As the pandemic further disrupts the balance between in-person care and telemedicine, we no longer have the luxury of waiting. The time to define, implement and enforce quality in all aspects of telehealth is not tomorrow but today. Formal certification by an international organisation requires hundred percent fulfilment of stringent criteria. This pre supposes commitment of a very high order and the realisation that excellence is always a moving target. One can never ever rest on one’s laurels. We need to keep running to stay where we are.


The Use of Fitness Trackers for Telemedicine
Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist Law Firm
Eshika Phadke
Associate, Arogya Legal – Health Laws Specialist Law Firm
Fitness trackers are increasingly being relied upon by people to monitor factors such as temperature, pulse rate, respiration rate, blood oxygenation, sleep patterns and exercise levels. Concurrently there has been a significant rise in remote consultations between patients and doctors. As a result, data from patients’ fitness trackers are making their way into telemedicine. However, doctors must proceed with caution while placing reliance on vitals that have been obtained from a fitness tracker.
First and foremost, even though fitness trackers offer medical device-like functionalities, they may or may not actually be medical devices. While a medical device is subject to regulatory scrutiny and has to undergo extensive clinical testing to ensure it’s accuracy before it is launched in the market, a fitness tracker does not undergo similar testing. Fitness trackers are, as the name would indicate, meant to track fitness levels and are targeted at healthy individuals. The manufacturers consciously elect to not pursue the medical device route, and do not intend for the device to be used to monitor vitals in a “patient”. They contain an explicit disclaimer on the packaging itself stating that the product is not a medical device and is not intended to be used for the diagnosis, treatment, cure or prevention of any disease. In addition, unlike a medical device, the health data of individuals collected by these trackers can be accessed by the manufacturer, and therefore while choosing a fitness tracker, doctors and patients should make an informed choice from data protection perspective on use of such health data by the manufacturer.
Second, the fitness trackers are not subject to conform with any uniform quality standards in India, and every fitness tracker uses a different technology and algorithm for tracking data and thus, hardly ever will two fitness trackers report similar numbers.
Further, fitness trackers are highly susceptible to human error and external conditions, and individuals are generally unaware of how to use the function correctly, so the data derived from a fitness tracker is not reliable. The reading would be affected by where the person is wearing it, how tight or loose the strap is, whether the person is wearing accessories that may hinder the sensor, whether the person is perspiring, whether they are correctly positioned, movement, the charge or the device, etc.
Therefore, while the utility of these devices is undeniable, their utility in medicine warrants abundant caution. The responsibility of a doctor to exercise great caution and professional discretion increases while discharging their professional services via telemedicine due to lack of physical contact with the patient. If a patient does use a fitness tracker and relays information from it to a doctor during teleconsultation, the doctor should refrain from taking the reading at face value or basing decisions solely on them. That being said, they may take it into consideration in combination with other symptoms and the patient’s history. The doctor could also peruse historical data from these devices to identify any patterns in the patient’s readings.
If a doctor does rely on any data that the patient obtained from a tracker, they should also note down the make and model of the device in their notes, if possible, so that they can also verify whether the tracker is a medical device or not. If it is, the doctor should also confirm with the patient that they used the device as per the manufacturer’s instructions.
Irrespective, before commencing a treatment plan on the basis of a information that had been obtained from a patient-operated device the vital signs of a patient should direct the patient to visit a doctor for and have their vitals measured and verified on a reliable device.
Telehealth and Medicine Today (TMT) Journal
Tory Cenaj
Founder and Publisher, Partners in Digital Health
Telehealth and Medicine Today (TMT) is an open access international peer reviewed journal examining the value of telehealth and clinical automation, its use and scalable developments, business process guidance, market research and the economic impact of digital health innovations in an evolving health technology sector. A world-class review board includes constructive commentary through rapid and rigorous peer review.
TMT’s audience includes leadership at hospitals and medical research centers, universities, payor organizations, IT/IS, healthcare providers, consultants, companies (early and more established), entrepreneurs, developers & start-ups, life sciences and device companies, pharmacy, NGO, government, and policy leadership around the globe.
For a complimentary subscription, register at:
https://telehealthandmedicinetoday.com/index.php/journal/user/register
Telemedicine Practice Guidelines – A Foundation Course for RMPs by TSI Faculty
To know more about the Telemedicine Foundation Course click on the link below:
https://tsi.org.in/courses/
Telemedicine – News from India & Abroad
India
Vyomanauts
Dr. Ganapathy strongly believes that the ultimate in Telehealth where the sky is no longer the limit (pun intended) will be a reality even in India in the next decade. The MoS Space has announced that India’s first International Space Station will be launched in 2030. ISRO hopes to launch our own Vyomanauts in 15 to 18 months from now. It is therefore not surprising that the ever future ready IIT Alumnus Club invited Dr. Ganapathy to give a talk on Extra terrestrial Healthcare. Profusely illustrated this talk gives several examples of technology transfer – tools planned to withstand microgravity and irradiation have resulted in better less expensive armamentarium for health care providers on earth. The full talk is available @….Readmore
Artificial Intelligence Helps Doctors With Patient Diagnoses
Artificial intelligence (AI) can facilitate a faster, automated route in decisions doctors need to take, ultimately meaning quicker answers and patient recovery….Readmore
International
British Man Receives World’s First 3D-Printed Eye
World’s first 3D-printed eye has been fitted to a middle-aged man in the UK, as part of a trial. reports media. Doctors at Moorfields Eye Hospital in London fitted the first ever 3D-printed eye… Read More
Machine Learning Predicts Death Risk in Heart Disease Patients
A new machine learning/artificial intelligence score provided an accurate forecast of the likelihood of patients with suspected or known coronary artery disease dying within 10 years…. Read More
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TN TSI Newsletter-
|
Submission may be sent to – tsigrouptn@gmail.com
Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff
Editors – Dr. Senthil Tamilarasan & Dr. Sheila John
Technical Partner- www.medindia.net







 History of Telemedicine @ Apollo Hospitals India
History of Telemedicine @ Apollo Hospitals India Problems that exists in Rural India to Adapt Telehealth
Problems that exists in Rural India to Adapt Telehealth
 Webinar on ‘Ethical Issues in Telehealth Practice’
Webinar on ‘Ethical Issues in Telehealth Practice’

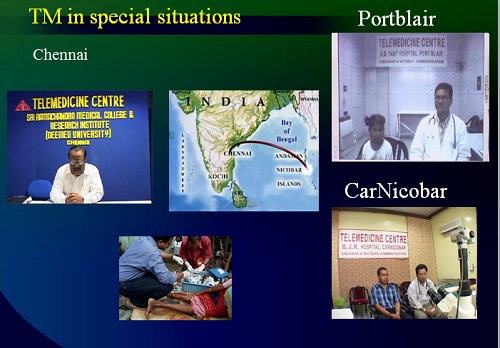
 ISRO’s contribution for Indian Telemedicine Program from Concept to completion – Towards National Adaptation
ISRO’s contribution for Indian Telemedicine Program from Concept to completion – Towards National Adaptation











 Dr. Sunil Shroff, MS, FRCS, Dip. Urol (Lond.)
Dr. Sunil Shroff, MS, FRCS, Dip. Urol (Lond.)







 Dr. BNR Subudhi
Dr. BNR Subudhi 
