Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
I am pleased to inform you about the online telemedicine course from TSI for the RMPs. This self-learning course with live interaction with the course faculty became operational this month. The course is called ‘Train to Practise Telemedicine’ and is housed on the learning management platform called MOODLE. In the near future ‘Telehealth speciality courses’ will also be developed. Please visit https://tsi.org.in/courses to view all the courses. If you wish to contribute as a TSI member you are most welcome to join us in development and delivery of these courses.
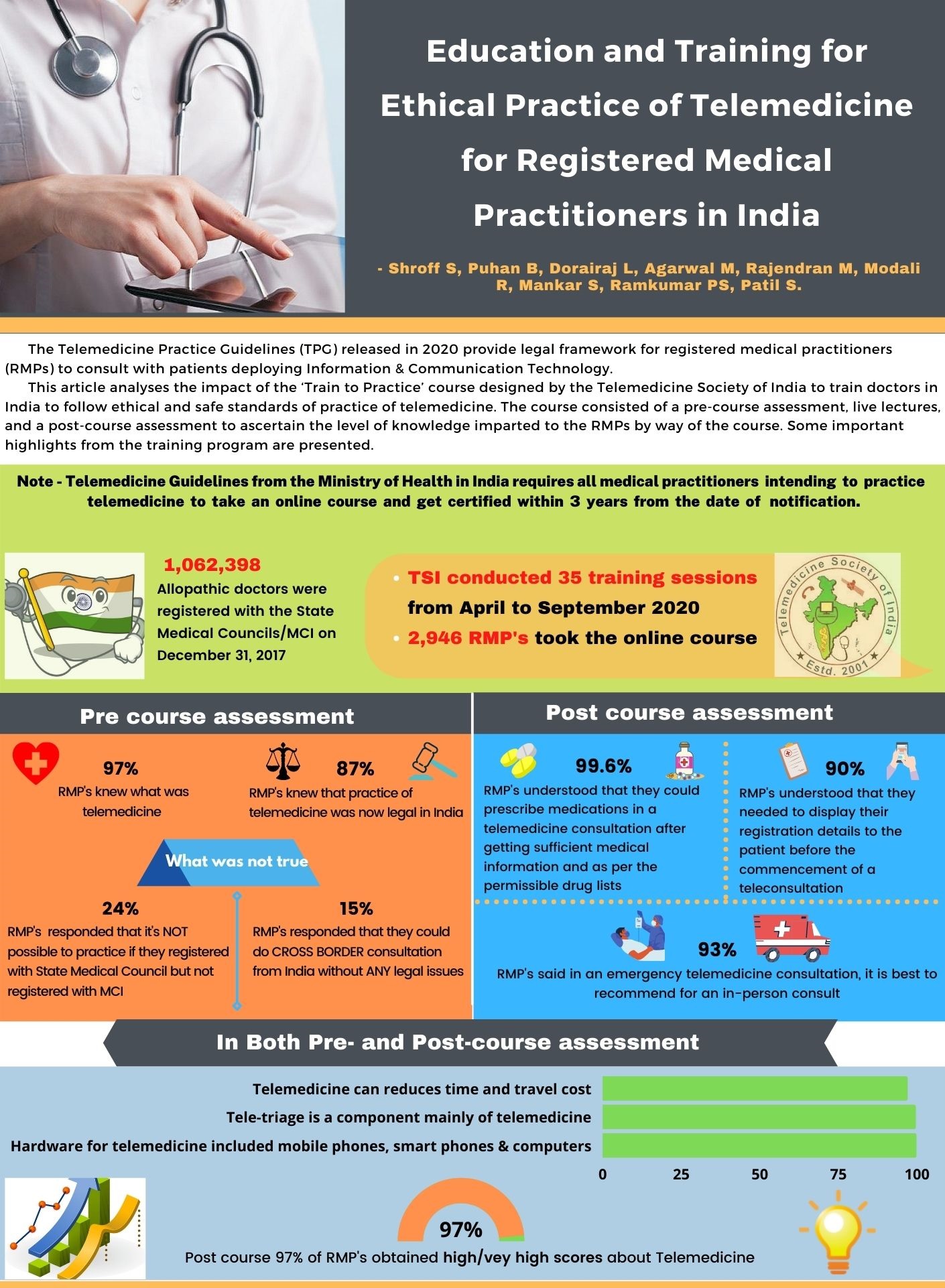
With the last issue of the Newsletter we have introduced visual abstract of articles. Please find the second visual abstract from TELEMEDICON2020.
We have also shared the Telemedicine course video – we request you to forward this in your groups to make the course popular.
Thank You. Dr. Sunil Shroff
Chief Editor
President – TN Chapter – TSI
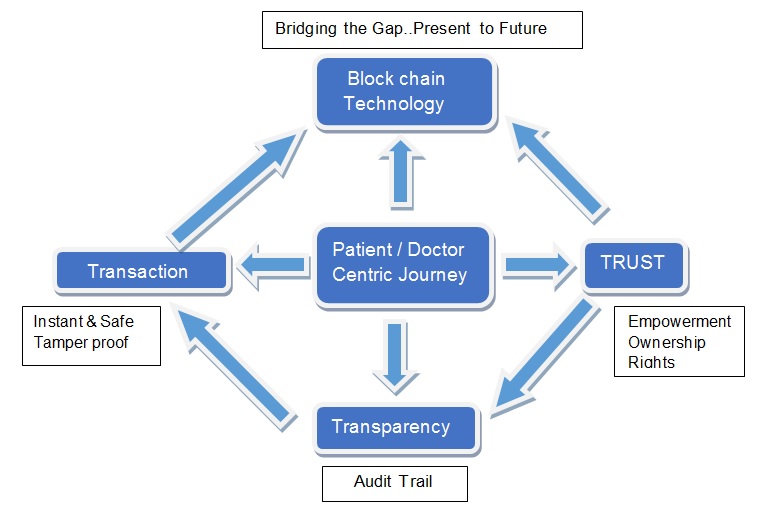
Towards Blockchain Based Secure Healthcare Information Systems
Prof. Prabhu Rajagopal Faculty-in-charge, CFI, IIT Madras, Associate, Center for Non-destructive Evaluation
A team guided by Prof. Prabhu Rajagopal, Lead Faculty – Remote Diagnostics at the Center for Nondestructive Evaluation (CNDE), Department of Mechanical Engineering, IIT Madras (IITM) has developed a first-of-its-kind Blockchain-based secure medical data and information exchange mobile application “BlockTrack” currently out on trial at IITM Institute Hospital. The BlockTrack project aims to securely digitize Healthcare Information Systems while ensuring protection of sensitive personal information and medical records by decentralizing the control and ownership of patient data, through a Blockchain-based innovation. Additionally, the algorithm to generate identification codes for users ensures uniqueness across boundaries with very little chance for duplication.
This disruptive innovation opens up the promise of a universal and transferable Healthcare Information Management with a strong emphasis on data privacy, and tracking the spread of infectious diseases across geographies. The Android version of the application has been developed separately for both patients as well as doctors.
(L) Dr. Rebecca Punithavalli, CMO, IITM Institute Hospital with the Doctor app. (R) Team member at the hospital with the Patient app.
Key outcomes from this project are:
Universally Unique Identification: Blockchain-based identifiers that are nearly impossible to duplicate
Interoperability of Systems: multiple hospitals, institutes, and healthcare organizations can join the system.
Single point records: The patient can choose to visit any healthcare facility which is on Blocktrack’s Blockchain Network without having any concerns about duplication of records or re-registrations. The consistency of the data flow is maintained without any branching issues.
This Blockchain platform developed by the team can further be used to integrate medical supply chain management and proactive tracking of the spread of contagious infections.
(L) Team members Selva and Ramashankar assisting the patients with app installation and user registration. (R) The Blockchain network running behind the application makes the entire system decentralized and secure.
Reflecting on this innovation, PI Prof. Prabhu Rajagopal said “Initiated at the height of the COVID pandemic, BlockTrack is an exciting project close to my heart, as this work showed that engineering innovations have disruptive potential to transform multiple domains. This is one of the first implementations of Blockchain technology for securing Healthcare Data management systems and we see the immense impact this approach can make in securely digitizing and maintaining unique patient records across the country and indeed across the world eventually. The system of permissions natural to Blockchain based distributed ledgers allows editability while maintaining privacy, opening up the possibility to integrate this system across primary healthcare, prescription, pharmacy, distribution and even insurance networks.We are grateful to Dr Sapna Poti at the office of Principal Scientific Adviser (PSA) to Government of India who brought the opportunity for funding this project under COVID themed support, and Infosys Limited for backing our vision. Dr Ravi Kumar of Infosys has been a gracious and supportive patron for this effort”
Prof. K. VijayRaghavan, PSA to the Government of India said “The National Digital Health Mission launched by the Government of India last year had the secure processing of individual data, and the easy accessibility of digitalized personal and medical records by individuals and health service providers, as its two important objectives. Effective implementation of these objectives will require leveraging emerging technologies. BlockTrack is a step in the right direction and I congratulate the team from IIT Madras for developing an innovative solution for a complex health information system. This will enhance and enable the efforts of health systems to efficiently track disease spread, and maintain confidentiality while storing personal data in a network.”
Teleophthalmology Adoption – Barriers and Solutions
Dr. T. Senthil MBBS DO FICO Ophthalmologist and CEO Welcare Health Systems Chennai Honorary Secretory, Telemedicine Society of India Tamil Nadu Chapter
With the COVID-19 Pandemic, as with any other modality of Telemedicine, Teleophthalmology Teleconsultations also saw a huge uptake initially- but as time progressed, the no of Teleophthalmology consults gradually came down to almost precovid levels. This article would evaluate the barriers and possible solutions for Teleophthalmology revival.
Teleophthalmology is done through the following modalities:
Teleophthalmology Consultation between Patient and an Ophthalmologist,
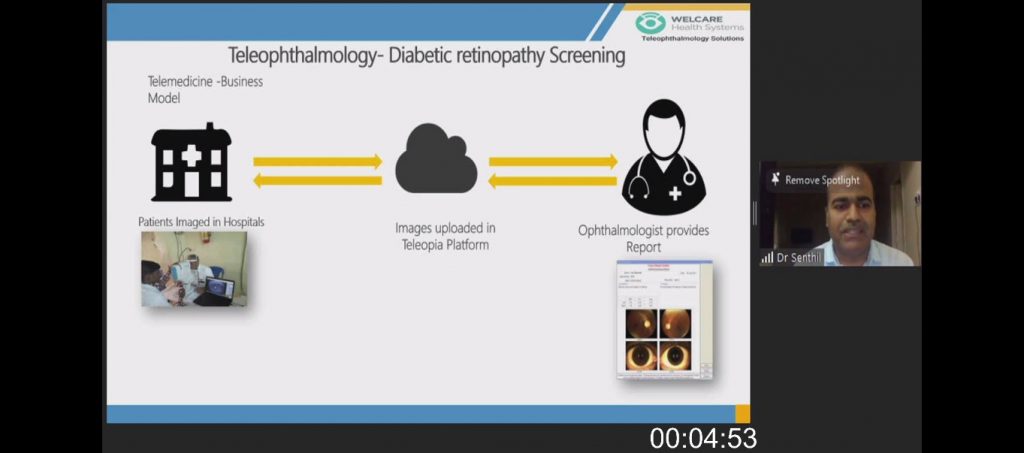
Image Based Teleophthalmology for Diabetic Retinopathy Detection,
Teleophthalmology for Retinopathy of Prematurity.
This article mostly covers the Teleconsultation part of Teleophthalmology.
Acceptance by Ophthalmologists and Patients
Teleophthalmology adoption by Ophthalmologists was very minimal before COVID, but once the pandemic struck and lockdown announced, Ophthalmologists started reaching out to their patients using Digital modalities, and patients also were accepting this newer modality. According to a study done by All India Ophthalmic Society only 17.5 % of Ophthalmologists were using Teleophthalmology currently, in another study 98.6 % of Ophthalmologists were willing to incorporate Teleophthalmology in their practices. There was an initial hesitation for the patients to make payment for Tele consults, but as time progressed patients started paying and this barrier was overcome.
The pandemic has hence created good acceptance level of Teleophthalmology among Patients and Doctors.
Dependence on Diagnostic Tests and Equipment’s
This is the most Important barrier to Ophthalmic Teleconsultations, since unlike psychiatry or dermatology, an Ophthalmic examination involves various tests right from testing Visual acuity, Intraocular pressure, anterior segment imaging and fundus evaluation. An Ophthalmic examination on a patient can only be done, if we get lot of information about the condition of the eyes, for which all these equipment’s are invaluable, it may not be possible to conduct these tests at patients houses, hence the number of conditions which can be treated by just doing a tele consult and seeing images of the Eye through regular computer or mobile cameras becomes grossly limited. This barrier can be addressed when there is app-based tests of visual acuity and mobile cameras getting in higher quality images etc. Till that time a model wherein patient can reach a nearby centre (Example an Optometry clinic, or Optical shop) where these equipment’s are available and tele consult done from that centre may be a viable option.
High Cost of Equipment’s and Poor Quality of Images
Other challenges
Lack of Trained Staff
Policy and Regulatory barriers
Privacy and Security concerns
With Innovations in Ophthalmic Devices and with advancements in machine learning and Artificial Intelligence, Image based Teleophthalmology will definitely see a growth in the coming years, Ophthalmic Tele consult will take its time, but as home-based devices are improved and available for a lower cost, there will be increase in Teleconsultations in Ophthalmology in the coming years.
TAKING YOUR PRACTICE ONLINE (PART 2): LEGAL COMPLIANCES AND GOOD PRACTICES
Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist
Eshika Phadke
Associate, Arogya Legal – Health Laws Specialist Law Firm
In our last article, we wrote about general considerations to be kept in mind before venturing into telemedicine. In this article, we will discuss important legal considerations to be kept in mind for operating a virtual clinic.
The Telemedicine Guidelines published last year recognize voice-video and text-based modes of consultations, so a doctor may choose to offer teleconsultation over any telemedicine apps, messaging/videocall app, SMS, email, or even set up a personal website for teleconsultations. But, while offering teleconsultations, it is important to be clear about legal dos and don’ts.
Registration of Online Clinic A common question that doctors have is whether they ought to register their work premises (or home) with any government body since they are offering medical services from the premises. In other words, does a doctor need to obtain a registration from a government department to operate a telemedicine “clinic”? The answer is NO, at least not at the moment. The existing clinical establishment or nursing home laws in various states in India regulate only those premises which receive patient footfall. By definition, virtual consultations between patient and doctor do not involve patient footfall at the premise from where the doctor is offering medical consultation. Therefore, clinical establishment or nursing home laws are presently not triggered by medical teleconsultations. Needless to say, if the venue is also used for in-clinic consultations, it would require registration under applicable clinical establishment/nursing home law.
Please note that this position may change in future if the law starts recognizing telemedicine-focused clinics as “clinical establishments”.
Website and privacy-related compliances If a doctor decides to offer teleconsultation through his or her own website, then there are certain legal requirements that must be complied with. The most important requirement would be to put in place a privacy policy. The exhaustiveness of the privacy policy would depend on the type of website that the doctor is operating. For example, if a website’s sole purpose is to enable patients to book an appointment, which is then conducted off the website (on a call, WhatsApp, Zoom, etc), a basic privacy policy specifying that the patient’s information is being collected so that the doctor can set up the appointment, would suffice. In such a case, the doctor should refrain from using a form on the website to collect information about the patient’s health condition since it would invite more stringent data privacy related compliances.
If a doctor is operating a website through which he/she can directly consult with the patient, the privacy policy would need to specify what kind of data (e.g. mental health data, physiological data, diagnostic reports, discharge summary etc.) is being collected, the purposes for which the collected data will be used and for how long will the patient’s data be stored, at the minimum.
The website should also have a term of service available as a link on the website itself, which outline the conditions under which services are being made available to the patient. An appropriate legal disclaimer should also be put on the website as applicable, such as that the telemedicine services over the website are not intended to be used in emergency situations.
Furthermore, a website or an app that offers teleconsultations would be considered as an e-commerce entity and as per the Consumer Protection (E-Commerce) Rules, 2020, an e-commerce entity must compulsorily be a company. Thus, a doctor has to incorporate a company if the doctor wishes to offer telemedicine services through the doctor’s own website to his or her patients.
Non-Solicitation The MCI (Professional Conduct, Etiquette and Ethics) Regulations, 2002 explicitly prohibits doctors from soliciting patients by “inviting attention to him or to his professional position, skill, qualification, achievements, attainments, specialties, appointments, associations, affiliations or honors and/or such character as would ordinarily result in his self-aggrandizement”. The Telemedicine Guidelines also specify that a doctor may not solicit patients for telemedicine through any advertisements or inducements. Therefore, whenever a doctor lists his or her experience and expertise on a telemedicine website or application, it should be limited to a description of the doctor’s recognized qualifications and years of experience only. The use of the expressions such as “expert”, “gold-medalist”, “best”, “leading” etc., may be held to be instances of solicitation and are best avoided.
While individual doctors (or groups of individual doctors) cannot advertise, clinical establishments can. Therefore, doctors who wish to market and advertise a telemedicine website or platform should do so through a separate legal entity such as a company or a limited liability partnership only.
When was the Term Telemedicine first used?(History and Evolution of Telemedicine – 8th Milestone)
Dr. Sunil Shroff, MS, FRCS, Dip. Urol (Lond.)
President, Tamil Nadu Telemedicine Society of India,
Editor, www.medindia.net,
Consultant Urologist & Transplant Surgeon,
Madras Medical Mission Hospital, Chennai, India (shroffmed@gmail.com).
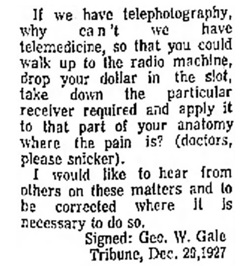
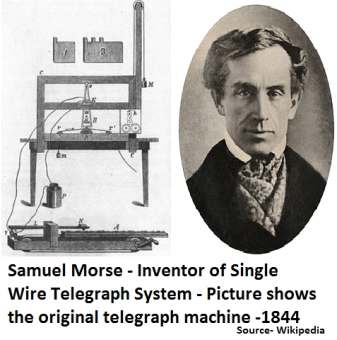
Telemedicine was used for the first time in a publication in December 1927
Geo W. Gale’s Article “Wants Plane to Change Weather Here”
“If we have telephotography, why can’t we have telemedicine, so that you could walk up to the radio machine, drop your dollar in the slot, take down the particular receiver required and apply it to that part of your anatomy where the pain is?
The cited article was dated December 29, 1927.
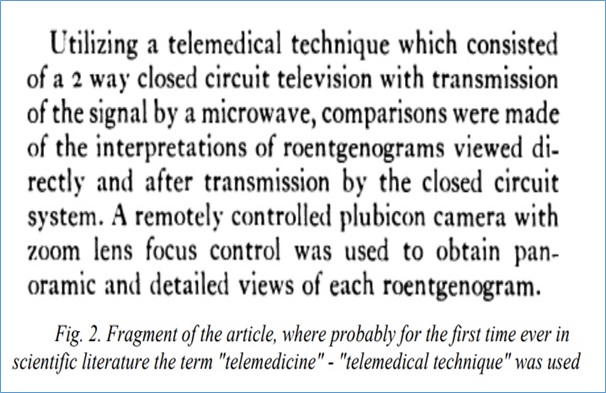
When was the Term Telemedicine first used in Scientific Literature? • Telemedical technique – 1970
• Telemedicine – 1972
The term “telemedicine” appeared in the description of the telemedical project of the Arizona Medical University in an article – Arizona TeleMedicine Network: Engineering Master Plan, 1972.
Telemedicine Practice Guidelines – A Foundation Course for RMPs by TSI
New Software Identifies Patients Who may Require Ventilator Support A new software helps identify whether a patient will require ventilator support in an ICU or referral, and will make necessary arrangements before emergency sets in. At a time when sudden ICU and other emergency requirements during the pandemic have been a challenge for hospitals to manage, timely information about such situations.….. Read More
International
Omron, Kyoto University team up to study AI use for early cardiovascular disease prevention Omron Healthcare and Kyoto University are set to undertake a study under a joint research programme to use artificial intelligence and home-recorded health data in predicting early signs of cardiovascular diseases.Their upcoming study under the Healthcare Medical AI research programme will focus on two themes…..….. Read More
Ophthalmology: A pioneer in the field of artificial intelligence Ophthalmology, with its heavy reliance on imaging, is an innovator in the field of artificial intelligence (AI) in medicine.Although the opportunities for patients and health care professionals are great, hurdles to fully integrating AI remain, including economic, ethical, and data-privacy issues… Read More
Life Whisperer launches its third global IVF clinic collaboration at ESHRE to apply Artificial Intelligence to Oocytes LONDON, June 25, 2021 /PRNewswire/ — Life Whisperer, fertility arm of AI healthcare company Presagen, will invite clinics to participate in its third global IVF clinic collaboration at the 37th European Society of Human Reproduction and Embryology (ESHRE) Annual Meeting in June 2021.….. Read More
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
What is New?
I am pleased to inform you about the online telemedicine course from TSI for the RMPs. This self-learning course with live interaction with the course faculty became operational this month. The course is called ‘Train to Practise Telemedicine’ and is housed on the learning management platform called MOODLE. In the near future ‘Telehealth speciality courses’ will also be developed. Please visit https://tsi.org.in/courses to view all the courses. If you wish to contribute as a TSI member you are most welcome to join us in development and delivery of these courses.
With the May Newsletter there are two additional features being introduced:
1.With this issue we are introducing visual abstracts and articles to make the newsletter more appealing and easy to read.
2.We have also introduced a new medico-legal digital health section and welcome contributions in this area. Mr. Anay Shukla from Arogaya Legal has agreed to contribute a short article for the next few issues.
Thank You. Dr. Sunil Shroff
Chief Editor
President – TN Chapter – TSI
Publication of TELEMEDCION2020 Abstracts and Select Articles in ‘Telehealth and Medicine Today’ Journal
Prof. K. Ganapathy
Guest Editor, Special issue on TELEMEDCION2020 in ‘Telehealth and Medicine Today’ Journal
Past President, Telemedicine Society of India & Neurological Society of India | Hon Distinguished Professor Tamilnadu Dr. MGR Medical University | Director Apollo Telemedicine Networking Foundation & Apollo Tele Health Services
The 16th International Annual Conference of the ‘Telemedicine Society of India’ (https://telemedicon2020.com/) was held virtually from 18th to 20th December, 2020.
The Tamil Nadu chapter of TSI under the leadership of Prof. Sunil Shroff, Organising Secretary along with four other TSI state chapters – Delhi-NCR, Rajasthan, Maharashtra and Karnataka organised this conference as a semi emergency, within 8 weeks. For the first time in two decades abstracts of papers presented have been published in a special issue of a US based journal Telehealth and Medicine Todayhttps://telehealthandmedicinetoday.com/index.php/journal/issue/view/20
This is in addition to the full text of nine papers presented at the conference (peer reviewed) besides two editorials.
John F. Kennedy in his inaugural address on 20th January 1961 remarked “ ……all this will not be finished in the first one hundred days. Nor will it be finished in the first one thousand days, not in the life of this Administration, nor even perhaps in our lifetime on this planet. But let it never be said that a beginning was not made “. I am much more optimistic. This optimism comes from the actions of my teacher Prof B. Ramamurthi. In the year 1951 four young men, driven by a passionate vision conceptualised, created and constituted India’s first ever neurological society. Dr. Jacob Chandy, Dr. B. Ramamurthi, Dr. S.T. Narasimhan and Dr. Baldev Singh brought all the disciplines associated with the science of neurology under one roof. The NSI was born. The four founding members were all office bearers !! This was audacity at its highest.
Within a year in March 1952, the society had its first meeting in Hyderabad, with 30 members from all over the country. The first presidential address was aptly titled “Neurology Comes To Life”. It was at this meeting the society decided to publish its own journal Neurology India. Today 69 years later Neurology India is a globally recognised journal with thousands of citations and 20% overseas contributions.
The world in April 2021 has turned upside down. If a journal could be started in 1952 in a then developing country in an unknown super speciality in the BC ( pun intended !) era with 30 individuals in the whole of India, I fail to see why we cannot start our own journal. Future Ready Next Generation Sequencing is now available across genetics labs in the country. It is time that the NG of Telehealth enthusiasts with access to all the resources in this planet step in and take over. Septuagenarians have shown the way.. “ Lead kindly light, lead thou me on, I do not ask to see the distant scene. One step enough for me” Saint John Henry Newman could very well have been referring to the Founding editors of TSI’s first journal.
I would like to once again place on record our thanks to the EC of the TSI to permit this exercise and also to Tory Cenaj and Prof Amar Gupta of Telehealth and Medicine Today for the unstinted support extended. HAPPY READING of the Special issuehttps://telehealthandmedicinetoday.com/index.php/journal/issue/view/20
Tele Ophthalmology Society of India – Launch Webinar on 1st May 2021
Dr. BNR Subudhi
I am happy to inform you that the Launching of Tele Ophthalmology Society of India was held on 4th April 2021 in Presence of President and Secretary of AIOS, President of Telemedicine Society of India and few international dignitaries working in the field of Teleophthalmology.
Padmashree Awardee Prof. S. Natarajan of Mumbai is the President of the Society I am the Hony Secretary, Dr. S. Pattanayak is the Treasurer and eminent Ophthalmologists of the country like Dr. R. Kim is the President elect, Dr. Rajeev Raman is the Vice President and Dr. Sheila John, Dr. Senthil, Dr. Abhesek, Dr. Ashok Nanda, Dr. Kavita Rao and Dr. Sandipak Ray are the executive members nominated to carry forward the objects of the Society which is primarily to provide Ophthalmic services to the needy rural and underprivileged people through tele consultation utilising digital technology, block chain and artificial intelligence.
As an initial step we have started collaboration with ECHO India, an organisation sharing their digital platform for Organising meeting, education, tele consultation facilities etc.
The first virtual Symposium of TOSI was organized on 1st May 2021 with Mr. Boman Irani, the Bollywood artist as the Chief Guest and other speakers from different fields of telemedicine and tele Ophthalmology like Dr. SB Gogia, Dr. K. Ganapathy of Apollo Telemedicine network, Dr. Sunil Shroff from Telemedicine Society of India, Dr. Ganesh Joshi from CRC Bhopal, Dr. Padmaja Rani from LV Prasad Eye Institute Telemedicine network and others. This gave us tremendous insight about planning ahead for the spread of Teleophthalmology systematically.
We have decided to have one monthly virtual symposium during this COVID time to interact with the members and the other stalwarts and Institutions and industry representatives to plan ahead for the members to reach the people through digital technology to prevent blindness.
The goal of Tele ophthalmology is to decrease the global burden of vision threatening diseases and improve the quality of life for patients worldwide. It will provide high quality, cost effective community eye care at the door steps of the community.
TAKING YOUR PRACTICE ONLINE (PART 1): LEGAL COMPLIANCES AND GOOD PRACTICES
Anay Shukla
Founding Partner, Arogya Legal – Health Laws Specialist
Eshika Phadke
Associate, Arogya Legal – Health Laws Specialist Law Firm
During the COVID-19 pandemic, telemedicine has proven itself to be a perfectly legal, effective and safe way for doctors to connect and consult with their patients.
However, before initiating a consultation over a phone call, email or through a mobile app with a patient, it is important that doctors familiarize themselves with the legal framework within which telemedicine can be safely practiced. In this article, we have enumerated key things to be kept in mind by doctors before they take their practice online-
Medical Council Registration. While a doctor does not need to be registered in every State where his or her patients are located for practicing telemedicine, a doctor still needs to have a valid registration with the medical council of the State in which he or she resides and practices.
Familiarity with Treatment Guidelines Every doctor must familiarize himself or herself with telemedicine-specific treatment guidelines applicable to his or her specialty. If no such guideline exists for a speciality in India, a doctor may refer to international guidelines that are easily available on the internet.
Exercising Professional Judgement with Caution. No guideline can substitute a doctor’s own professional judgement to treat his or her patient. However, as a thumb rule, it may be pragmatic to err on the side of caution while offering remote consultation given the lack of physical access to the patient.
Limitations of Technology and Communication Medium. A doctor should always be conscious of the limitations of today’ technology and the medium of communication – mobile network, WiFi, internet speed, camera quality, audio, video, text, email, etc. and should offer his or her services virtually with full awareness of these limitations. It is not wrong on the part of a Doctor to request his or her patient to switch to a different teleconsultation medium or an in-person visit, if the doctor desires so in the interest his or her patient’s health.
Maintaining Patient Privacy. A doctor’s virtual clinic should be conducive to maintaining the patient’s privacy, just like his or her actual clinic. As a good practice, a doctor should also ensure that his or her patient is present in a comfortable surrounding from which the patient can have an open discussion.
Identifying Oneself to the Patient. As in physical consultation, a patient should be able to verify a doctor’s credentials and contact details in a remote consultation. If the teleconsultation is through a reliable teleconsultation App, the App will most likely display the doctor’s name, registration number, qualifications and contact information. However, if a doctor is consulting through WhatsApp, email, videoconferencing service etc., he or she should consciously display his or her registration number and name. In cases where the doctor and patient are unknown to each other, it is expected that the doctor will introduce himself or herself along with his or her qualifications to a patient, and also confirm the patient’s identity by asking the patient’s name, age, and contact information. A doctor has the legal right to request that the patient displays/shares a proof of identity with the doctor before the start of consultation, if necessary.
Maintaining Records. Before venturing into telemedicine, every doctor should establish a process to maintain and preserve records electronically. For instance, a log book for each interaction with patient should be maintained. A record of patient history, diagnosis, prognosis and prescriptions issued, if any, should also be maintained. The patient’s consent for the consultation should also be recorded, if the patient has not initiated the consultation. It is a good practice to maintain these records for a minimum period of three years.
Prescriptions. A prescription generated in course of a telemedicine consultation should not be different from a physical consultation, and should contain all information as is associated with a prescription generated during a regular consultation (for example, patient identifiers, patient history, date of consultation, provisional diagnosis, investigations recommended, medicines prescribed etc.). The prescription may be handwritten or digital, but it should be signed by the doctors, preferably by hand.
Insurance. As a safeguard against consumer complaint or legal liability, doctors who offer remote consultations should ensure that they have purchased a professional indemnity policy that either explicitly covers teleconsultations, or does not explicitly exclude it. This is not to imply that telemedicine may result in a legal issue. It’s just one less thing to worry about!
Reference: Telemedicine Practice Guidelines
NEXT TOPIC- TAKING YOUR PRACTICE ONLINE (PART 2): LEGAL ISSUES AND CHALLENGES
Space Travel and Telemedicine (History and Evolution of Telemedicine – 7th Milestone)
Dr. Sunil Shroff, MS, FRCS, Dip. Urol (Lond.)
President, Tamil Nadu Telemedicine Society of India,
Editor, www.medindia.net,
Consultant Urologist & Transplant Surgeon, Madras Medical Mission Hospital, Chennai, India (shroffmed@gmail.com).
As space travel became a reality, scientists were curious in the 1960s to find out if the human body could function adequately in outer space or not. And this brought NASA contributing to the growth of telemedicine in 1960s. They first sent animals into space who were connected to medical monitoring systems and their biometric data was transmitted back via a telemetric link.
NASA soon established an Integrated Medical and Behavioral Laboratories and Measurement Systems (IBLMS) to study changes in human physiology in outer space with zero gravity and its effects on human body.
The report described the objective of this centre as – “..It was meant to develop a system that could acquire, display, analyze and record, “…a wide variety of medical, biochemical, microbiological, and behavioral, measurements and experiments designed to study in detail man’s well being and operational capability.
NASA also launched a program, called the Space Technology Applied to Rural Papago Advanced Health Care (STARPAHC). It leveraged the remote monitoring technology that they had developed for space travel to serve terrestrial, rural populations.
The project was conducted on the Papago Indian reservation in Arizona. It evaluated the practicality and efficacy of a large-scale telemedicine operation. This truly gave a new spin to telemedicine for ‘reaching the unreached population to provide healthcare.’
Telemedicine – News from India & Abroad
India
Need to take telemedicine to villages: PM In an interaction with doctors on Monday, PM Narendra Modi drew attention to the importance of telemedicine, how it has played a big role for patients in home isolation and asserted that it needs to be expanded in rural areas as well. The PM also urged doctors to include oxygen audits in their daily routine.….. Read More
80% diseases can be nipped with primary healthcare Healthcare workers, across country, with constant training, have the potential to de-clog and reset the healthcare system. Data Driven Decisions and support for carrying out their tasks should be one of the priority.….. Read More
International
Mental health chatbots might do better when they don’t try to act human Digital mental health platforms have seen something of a renaissance during the Covid-19 pandemic, as in-person appointments have been relegated to the digital sphere. For those who cannot access therapy from a human clinician, mental health chatbot platforms are an increasingly popular digital alternative…….. Read More
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Guidelines for submission to TN TSI Newsletter-
Report can be from 500 to 600 words
Report Should be relevant to Telemedicine or Medical Informatics
No promotion of self or any product
Avoid plagiarism
All references should be included
Provide any attributions
Visuals are welcome including video links
Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Registration for Telemedicine Online Course
Telemedicine Society of India runs regular courses on how to practice telehealth within the framework of ‘Telemedicine Practise Guidelines’ as notified by the Govt of India in the month of May 2020. Over 3500 doctors and other medical professionals have undergone the training so far. To know more about the course and view the feedback please visit https://tsi.org.in/learn
By registering here you would be able to book your space for the next available course. We are also in the process of starting a Speciality Course in Telehealth and will keep you updated if you are registered with us.
Click here to join ‘Train to Practise Telemedicine’ Course conducted by TSI.
Thank You. Dr. Sunil Shroff
President – TN-TSI
National Telemedicine Day of TSI Celebrated Virtually
In view of the ongoing pandemic, an abridged program was conducted on 25th April virtually to commemorate the National Telemedicine Day of TSI. This was decided 20 years ago on 25th April 2001, during the 1st National Telemedicine Conference held at SGPGI Lucknow, to raise a Society to promote Telemedicine in India and to name it Telemedicine Society of India (TSI).
A panel discussion that included all the Past Presidents (Margdarshaks) was organised with the theme – ‘A Perspective of Journey of Two decades of Telemedicine Society of India & The Road Ahead.’
The discussion was aimed towards TSI’s contribution towards the global effort to promote Telemedicine, roadmap for progress and increased footprint of TSI.
Dr. Mahendra Bhandari who was the director at SGPGI during the launch of TSI joined from USA and shared his fond recollections from the past.
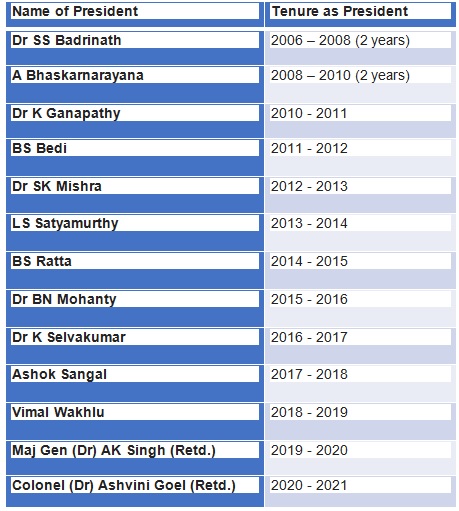
The presidents who joined included the following-
Dr. SS Badrinath, sent a short video of his tenure as he is not keeping well. Mr. A Bhaskarnarayana could not join. The discussion was moderated by Dr Sunil Shroff, President TSI (TN Chapter).
The following areas were discussed –
1. All the presidents shared – one impact area that they considered significant that led to growth of telemedicine during their tenure and one memory that they would always cherish of their tenure.
2. They all discussed the impact of emerging technologies in the domain of ‘Digital Health’ that would help with the evolution of Telemedicine.
3. Deliberations were made on the how TSI could play an active role and work with the Government for policies in the growth of telehealth in India.
4. TSI functioning was broadly discussed and included – a. TSI’s role in keeping the Telehealth ecosystem safe in India. b. How should state chapters of TSI evolve. c. Should TSI start its own journal. d. How should TSI professionalise its activities. e. What should be the roadmap for next 5 to 10 years for TSI.
Welcome by Dr Ashvini Goel & Inauguration by Dr Mahendra Bhandari
Panel discussion with Presidents (Margdarshaks)
Theme – ‘A Perspective of Journey of Two decades of Telemedicine Society of India & The Road Ahead.’ Moderator: Dr.Sunil Shroff, President, TN-TSI
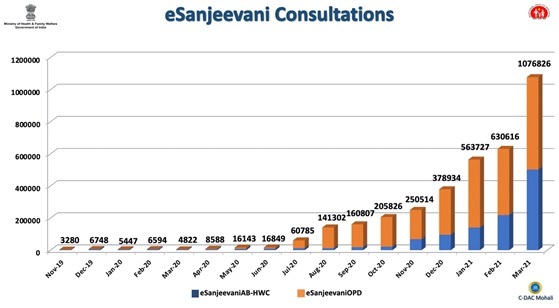
eSanjeevani – India’s National Telemedicine Service
Sh. Lav Aggarwal1, Dr. Sanjay Sood2 & Dr. P.K. Khosla2 1 Ministry of Health & Family Welfare, Govt. of India, New Delhi 2 Centre for Development of Advanced Computing, Mohali
eSanjeevani – National Telemedicine Service is a cutting-edge, indigenous telemedicine system that is not only bridging the rural-urban, digital health divide but is also provisioning health services for the Indian populace in the confines of their homes. eSanjeevani is an initiative of the Ministry of Health & Family Welfare, Govt. of India it has been developed and is being managed by the Health Informatics Group at the Centre for Development of Advanced Computing (C-DAC) in Mohali. eSanjeevani is providing telemedicine services in two variants: 1. eSanjeevaniAB-HWC: A Doctor-to-Doctor telemedicine system under Ayushman Bharat Scheme of Govt. of India at Health & Wellness Centres, to provision specialised health services in rural areas and isolated communities, and 2. eSanjeevaniOPD: a Patient-to-doctor, telemedicine system that is enabling people to get outpatient services in the confines of their homes.
In a very short span eSanjeevani has evolved into South-East Asia’s largest telemedicine service. Collectively, the eSanjeevani network is operational in 31 States, around 35,000 doctors and paramedics have been trained and onboarded, and around 18,000 Health and Wellness Centres (HWCs) have been enabled for telemedicine services across the country. 256 online OPDs have been set up on eSanjeevaniOPD. eSanjeevani telemedicine network is providing safe, contactless medical consultations without having the patient to travel to the doctors. eSanjeevani is supposedly India’s largest telemedicine service. In less than one-year eSanjeevani has served over 3.7 million patients and daily around 45,000 patients are served through eSanjeevani. Numerous premier institutions like AIIMS Bathinda, AIIMS Bibinagar, AIIMS Rishikesh, Lady Hardinge Medical College and Hospital, King George’s Medical University etc. are offering specialised services through eSanjeevani. This flagship telemedicine application of Government of India is in a continuous state of flux, it is being enriched on regular basis (with innovative concepts and flows) based on the feedback received from the State Administrations that are using eSanjeevani, and also on the basis of the directions of Ministry of Health & Family Welfare, Govt. of India.
eSanjeevani is the first telemedicine platform that conforms to the Electronic Health Records Guidelines issued by the Ministry of Health & Family Welfare, Govt. of India. It being a cloud-based system, the system can be configured and expanded in no time. The telemedicine platform enables health administrators to efficiently utilise doctors in their team as the system permits health administrators to dynamically regulate doctors onboarding and offboarding in OPDs, based on the footfall. In eSanjeevani, the processes have been designed in such a way that patients do not need to wait for more than 15 minutes to get a medical consultation. As of now average patient waiting time in eSanjeevaniOPD is 8 mins 47 sec.
eSanjeevani empowers, doctors and patients additionally as it is also integrated with few healthcareIT applications that are being used in the States. eSanjeevaniAB-HWC is seamlessly (& wirelessly) integrated with a compact and integrated diagnostic device. It can gather over 30 medical parameters based on point of care tests (POCT) and rapid diagnostic tests (RDTs) besides the physiological parameters. eSanjeevani variants are available as web-apps (esanjeevani.in & esanjeevaniopd.in) and Android application of eSanjeevaniOPD is also available, it has been downloaded by over 500,000 users. The iOS version of eSanjeevanOPD is undergoing testing and soon it will be rolled out. With the launch of iOS based app of eSanjeevaniOPD, it is anticipated that the utilisation of eSanjeevani would grow further. At the moment over two-thirds of the consultations are being executed through mobile application. eSanjeevani is being readied to comply with the compliances specified by the National Health Authority in National Digital Health Mission of National Health Authority, Govt. of India.
In December 2020, at Digital India Awards 2020 eSanjeevani was adjudged as the country’s best innovation during pandemic and the award was conferred by Honb’le President of India. eSanjeevani has also been recognized by Computer Society of India, SKOCH Group and has won the Gem of Digital India Award. eSanjeevani is also amongst the front-runners at Govt. of India’s National Awards for eGovernance (NAeG).
Foundation Day CME “COVID-19 and Telemedicine”: Department of Telemedicine, PGIMER, Chandigarh
The foundation day CME for department of telemedicine was inaugurated by Prof Jagat Ram Director, PGIMER and Prof G D Puri Dean Academics, PGIMER.
They congratulated Prof Meenu Singh Head, Department of Telemedicine on this occasion and appreciated all the work that has been done during the COVID – 19. Director emphasized on the importance of Telemedicine in this pandemic Scenario. This CME was chaired by distinguished dignitary, Dr K K Talwar health adviser Government of Punjab and Former Director, PGIMER.
The CME was presided eminent speakers Dr Sanjay Sood, Project Director eSanjeevani who briefed the audience that during the past one year of esanjeevani OPD almost 2.6 million consultations have been provided. Through Various other Telemedicine platforms run by govt of INDIA consultations have touched the 4 million mark. E Sanjeevani provides both doctor to doctor as well as doctor to patient consultations.
Dr Sood shed light on the future project such as SEHAT OPD, e Arogya Bharti and national HIV AIDS Telemedicine network which is first in the world.
The first panel discussion was chaired Dr Savita Malhotra Former Dean PGIMER and talks were given by Shri R K Saboo Past Rotary International Prident, Dr Vinayak M Prasad Senior Advisor, WHO, Geneva and Shri Anoop Kumar Gupta Principal Consultant, eVBAB Project, Ministry of External Affairs.
The discussion was centered on role of national and international Telemedicine agencies during the COVID-19 pandemic. The second Panel discussion was Chaired by Col. Dr. Ashvini Goel, President TSI and the speakers were Dr Sunil Shroff Foundation and Director MOHAN Foundation President TSI-Tamilnadu, Dr Murthy Remilla Hon. Secretary, TSI and Ms Bagmisikha Puhan Legal Expert technology Law Member EC TSI. The panel discussion was regarding Telemedicine practice guidelines
This followed talks by Dr Ravi Chittoria, Nodal Officer, Regional Resource Centre (Southern Region) JIPMER, Puducherry and Dr N. K Agarwal on Telemedicine activities in the NMCN project during COVID era and Clinical Application of Telemedicine respectively. This session was chaired by Dr S K Mishra Dean SGPGI Lucknow and Dr Biman Saikia from PGI Chandigarh.
The CME concluded by a lecture on role of health informatics in healthcare given by Dr Nishant Jaiswal Research Associate HEHTA, Institue of Health and well Being, University of Glasgow. This session was charied by Dr Nusrat Shafiq PGI, Chandigarh and Dr BS Bedi, Advisor to CDAC. Dr Meenu Singh gave the concluding remarks and thanks to all the dignitaries for their supports and Dr Amit Agarwal for organizing and smooth functioning of the CME.
First use of the Prefix ‘Tele’ for Telemedicine (History and Evolution of Telemedicine – 6th Milestone)
Dr. Sunil Shroff, MS, FRCS, Dip. Urol (Lond.)
President, Tamil Nadu Telemedicine Society of India,
Editor, www.medindia.net,
Consultant Urologist & Transplant Surgeon, Madras Medical Mission Hospital, Chennai, India (shroffmed@gmail.com).
The credit for using the prefix ‘Tele’ goes to the speciality of cardiology. In the earlier issue of the newsletter, the transmission of ECG over 1500 meters by Willem Einthoven, a Dutch professor of physiology (Telehealth Newsletter -Vol.1, Issue.2 Nov 2020) was covered. It was Einthoven who first to use this Latin prefix Tele to denote distant medical care and called it “telecardiogram”. He went on to publish this in 1906 in the journal “Archives Internationales de Physiologie” describing this experiment as the first tele-medical technology (Einthoven, 1906). After this over the years, several publications were made on the use of tele-ECG application that avoided the need for the patients to travel.
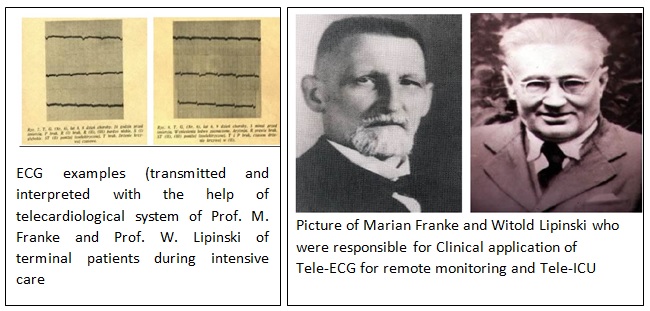
But it was M. Franke and W. Lipinski 1936 who published an article about clinical application and variations in tele-electrocardiogram of patients with infectious diseases (in particular with scarlet fever and diphtheria). They invented the Franke-Lipinski tele-cardiological system and helped patients to avoid travel. Franke said in an article, “keeping the patient in one place allowed avoiding adverse events, associated with the patient’s transportation.” This was more required for patients with infectious diseases where remote monitoring was required. They also felt that it could be applied for critically ill patients on ventilation and this was the first indication of the use of telemedicine for intensive care.
In 1980 E. Sh. Halfen, said “One of the characteristic features of medicine of our time is authoritative, irresistible penetration of mathematics and cybernetics into medicine” He determined three main lines for tele-ECG application (Halfen E., 1980; 1985; 1974; 1977; 1980 a; 1980 b; 1980 c; Khramov A. et al., 1996):
1. Clinical medicine (including rural health care, emergency medical service, large enterprises, sanatoria, etc.);
2. Mass preventive onsite screening examinations (combined with automated ECG analysis);
3. ECG patient-activated transmission (auto-transmission) during outpatient treatment.
And between 1972 and 1979 about 250 000 ECGs were transmitted in Saratov region.
Today India’s own STEMI project is an advanced application of remote monitoring through ECG transmission to reverse the fatal ST Elevation Myocardial Infarction (STEMI). This is a clinically a challenging condition that requires prompt intervention. In Tamil Nadu alone there have been over 2,400 early interventions in the last few years. The National Commission on Macro-economics and Health has projected the evolving epidemic of coronary artery disease in India. There were 60 million patients with coronary heart disease in the year 2015 with a yearly mortality close to 3 million. A substantial number of these were due to acute STEMI or the delayed consequences of STEMI. If the project is implemented nationally and connected to the 108 State Ambulance services it can save millions of lives.
Reference- 1. A Century of Telemedicine:Curatio Sine Distantia et Tempora by- Anton Vladzymyrskyy, Malina Jordanova, Frank Lievens 2. Telehealth Newsletter – Vol.1, Issue.2 Nov 2020 3. https://www.stemiindia.com/
Telemedicine – News from India & Abroad
India
India’s First Artificial Intelligence-based COVID Testing Facility at IGI Airport
India’s first Artificial Intelligence (AI)-enabled COVID testing facility for international passengers has commenced operations at Terminal 3 of the IGI Airport. The facility under the Garuda brand name is owned by AI company Thalamus Irwine.….. Read More
International
How innovations in digital health are opening new doors in healthcare system Technological advancements and innovation have played a big role in connecting people to healthcare professionals, allowing them to get the healthcare attention they need, especially during the COVID-19 pandemic..….. Read More
Companies That Are Taking Telemedicine By Storm When Covid-19 struck, the use of telemedicine exploded. At Los Angeles-based UCLA Health, for example, the average number of telehealth visits went from roughly 100 to 3,000-4,000 per day between March and May 2020. Companies include – 1. Teladoc, 2. Livongo, 3. Navigating Cancer, 4. 98point6, 5. 23andMe & 6. Amazon.. Read More
World’s First 5G Disinfection Robot Removes Bacteria On The Go The world’s first 5G-based disinfection robot automates anti-infection efforts against COVID-19 in health care facilities.….. Read More
New Model Predicts Spread of Covid-19 New model has been developed by scientists that helps predict the spread of covid-19. At first, a fragile, temporary state of immunity emerged during the early epidemic. Later, it got destroyed when people started changing their social behaviors leading to another wave of covid-19 infection..….. Read More
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Technical Partner- www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Technology in Telehealth
Prof. K. Ganapathy
Past President, Telemedicine Society of India, Neurological Society of India & Indian Society for Stereotactic & Functional Neurosurgery | Former Secretary general Asian Australasian Society of Neurological Surgery | Hon Distinguished Professor The Tamilnadu Dr MGR Medical University | Formerly Adjunct Professor IITM and Anna University | Director Apollo Telemedicine Networking Foundation & Apollo Tele Health Services
There is an erroneous perception that widespread adoption, upscaling and deployment of Telehealth is solely related to availability of cost effective, affordable, accessible, user friendly technology. There is no doubt that technology acceptance and behavioral modification, which we are witnessing particularly after the onset of COVID-19, has a major role to play. “ Customer delight” is what every e Commerce platform aims for. The Amazons and Flipkarts and Googles of the world package their products in such a way that even octogenarians from rural backgrounds get hooked to the incredible experience. Whom are we selling telehealth to? Who needs to get “ hooked on” to experience virtual remote health care. How do you convince a worried or sick patient tens, hundreds thousands of kilometers away that the specialist on the screen can do as good a job or even better than if he is holding your hands directly. How do you excite every individual doctor to evangelise Telehealth. This will happen only when his/her patient is convinced that telehealth is as good or better than a face to face consultation 5G, bandwidth of 100 Mbps, a 55” hi resolution screen, a future ready voice activated EMR where images uploaded with ease at the remote end can be digitally manipulated by the consultant, playing videos, a wide choice of highly secured payment gateways etc etc – the list can be never ending —– all this hi tech no doubt will help, but are we not missing the wood for the trees.
What does a patient using Telemedicine really want – even in 2021 . He wants TLC ( Tender Loving Care) “Listen, listen, listen he is telling you the diagnosis” said Sir William Osler 150 years ago. When I give a teleconsult I still listen!! Patients do not care how much you know. They want to know how much you care. Healthcare is personal – it is very hard to feel your experience was excellent, when those treating you don’t introduce themselves, or make eye contact, or say what they are doing to you and why. The doctor’s body language says it all. No AI, no technology will ever substitute for a doctor who empathises, sympathises with his far away patient, wiping the patients tears albeit virtually.
Alas the powers that be, including teleconsultants forget that providing remote health care is not like selling/ buying a pizza online or booking a train ticket. Technology in healthcare should only be a tool, a means to achieve an end, not an end by itself. Technology helps in producing remarkable solutions. Sometimes after this we go in search of problems! Lars Leksell the inventor of the Gamma Knife famously remarked half a century ago –“ A fool with a tool, is still a fool”. I belong to the BC era – not Before Covid but before Computers. Yes I am a technology buff. I even brought out a special edition for the journal Neurology India on “Extra Terrestrial Neurosciences” – the ultimate in Technology. Over the last 21 years when I first started Telemedicine, it has been my privilege to see the radical transformation and the exponential growth of Remote Health care . I am optimistic that soon Telehealth will be centre stage in the core of the health care delivery system. This phenomenal growth is no doubt a direct bye product of technological advances . An app a day may keep the doctor far far away but I would still like my tech savy doctor to be commiserating, to understand what I want so that he will prescribe the right apps for me !! “ Customer delight” is the only way that Telehealth will truly come centrestage and be integrated into the core of the health care delivery system. Worldwide remote health care is driven by technologists, software/ hardware entrepreneurs, communication engineers, mobile network operators, CEO’s of start ups. Manufacturers of peripheral medical devices, wearables etc. During the last 21 years 95% of the numerous talks I have given have been organized by the Telemedicine ecosystem!! Medical colleges, medical associations, clinical societies do not include Telehealth in any CME program. It is extremely unusual to find a clinician giving up a medical or surgical career to embrace telehealth .
The clinician should be the first among equals if patients are to get excited about telehealth abd take the initiative requesting his/ her doctor to appear on the screen. Circumstances and necessity will make doctors understand that this tool for connecting, ensuring a continuum of care will no longer be a choice but will become a differentiator The wrioting is on the wall !
Telemedicine Society of India and Practo launch ‘Rise of Telemedicine – 2020’ report
Dr. Neelesh Bhandari, MBBS (AFMC), MD (Pathology)
Head, Doctor Relations and Engagement | Former Founder and CEO, Healtho5 Solutions Private Limited | Former Chairman, Social Media Committee, Indian Association for Medical Informatics.
Summary: A joint collaboration with the Telemedicine Society of India (TSI), the report highlights the emergence of telemedicine in India, the reasons behind its meteoric rise amid the pandemic, and the advantages it can continue to offer in a post-COVID world.
The report was launched at Telemedicon 2020, by Col. (Dr.) Ashvini Goel, President, Telemedicine Society of India (TSI) in the presence of industry leaders – Dr. Alok Roy, Co-Chair, FICCI Health Services Committee and Chairman, Medica Group of Hospitals, Dr. Girdhar Gyani, Director-General, Association of Healthcare Providers (India), Dr. Vijay Agarwal, President, Consortium of Accredited Healthcare Organizations (CAHO).
The sense of urgency created by the COVID-19 pandemic has spurred medical establishments to overhaul their healthcare delivery systems in pursuit of maximizing patient care and minimizing the risk of infection. This accelerated the adoption of telemedicine practices in India, effectively mitigating the impact of the pandemic while laying the foundation for an innovation-led, patient-centric healthcare system in a post-COVID world.
By tracing the trajectory of the meteoric rise of telemedicine in India since the outbreak, this report by Practo and TSI, launched at Telemedicon 2020, has attempted to recapitulate the key factors contributing to this spike and its long-term benefits.
Commenting on the report, Col. (Dr.) Ashvini Goel, President, Telemedicine Society of India, said, “To witness the significant growth of telemedicine in the past few months has been overwhelming. In a short span of time, the digital health space has evolved and online consultations have become the spine of healthcare delivery systems globally. The pandemic has only allowed us to reiterate our vision for future healthcare that’s convenient, accessible, and affordable for a billion+ Indians.”
Adding to that, Dr. Alok Roy, Co-Chair, FICCI Health Services Committee and Chairman, Medica Group of Hospitals, said, “TSI-Practo telemedicine report is like the Harry Potter magic portal, showing both current and future realities; a step in the right direction will transform the way healthcare is accessed forever.”
Extensively researched and backed by insights culled from the experience of crores of Indians who used Practo between March 2020 and November 2020, this report provides valuable information and factual evidence for all stakeholders of the healthcare ecosystem seeking to understand the role and impact of telemedicine in India.
Shashank ND, CEO & Co-Founder, Practo, said, “Our aim with this report is to ignite meaningful discussions around telemedicine as a critical first step towards establishing more collaborations among stakeholders, tied by a common commitment to one industry. We have tried to cover all aspects of the upward trajectory taken by telemedicine during the pandemic, and the direction it is expected to take in a world no longer under the threat of COVID-19 by carefully analyzing data captured since the outbreak.”
Key insights from the report:
Physical appointments went down by 32%
Visits to secondary care specialists like neurosurgeon, somnologist, cardiologist, and oncologist grew dramatically
3x increase in the number of people using online consultations
26% of the consultations were with GPs, followed by Dermatology (20%) and Gynecology (16%) and others like Gastroenterology, ENT, and Pediatrics stood at 7% each
The fastest-growing health concerns included ophthalmology, ENT, orthopedics, pediatrics, and gastroenterology
Delhi, Mumbai, and Chennai saw an average of 16x growth in queries for ENT specialization
Non-metros saw the highest growth of 7x in online consultations, as compared to the same period in the previous year
During the same period last year, the split between metro:non-metro for online consultations stood at 75:25. This year, it is 60:40, demonstrating that the number of online consultations from non-metro cities is on the rise
Tier 2+ cities like Manjeri, Arrah, Balasore, Etah, Orai, Khopoli, Jagtial, and Shivpuri used telemedicine for the first time in this time period
Cities like Meerut, Jammu, Srinagar, Nellore, Kochi, Gorakhpur, Kakinada, Tirupati, Bhagalpur, Gaya, and Shimoga recorded a 10x growth
Non-metros saw the highest growth of 7x in online consultations, as compared to the same period in the previous year
During the same period last year, the split between metro:non-metro for online consultations stood at 75:25. This year, it is 60:40, demonstrating that the number of online consultations from non-metro cities is on the rise
Tier 2+ cities like Manjeri, Arrah, Balasore, Etah, Orai, Khopoli, Jagtial, and Shivpuri used telemedicine for the first time in this time period
Cities like Meerut, Jammu, Srinagar, Nellore, Kochi, Gorakhpur, Kakinada, Tirupati, Bhagalpur, Gaya, and Shimoga recorded a 10x growth
Among metros, Chennai witnessed the highest growth of 4x as compared to the previous year
Bengaluru, Delhi-NCR, Mumbai, Pune, Hyderabad, and Kolkata grew by more than 300% as compared to last year
More and more elderly people are now getting used to technology
There was a 502% spike in online consultations from people above the age of 50 during this crisis, who contributed to 12% of overall consultations, as compared to just 5% the previous year
More women are going online
Last year the men:women ratio stood at 75:25, while this year it’s 68:32
Gynecologists and General Physicians were two of the most consulted specialists by women in 2020
Online mental health consultations and queries continued to rise during this period
There was a 302% increase in overall mental health-related queries
Women contributed to 33% of overall queries for mental health specialists
More consultations at late hours
25% of online consultations were recorded between 10 pm and 4 am when people are not burdened with work responsibilities
One of the top specialties consulted during late-night hours was Psychiatry
Preferred day(s) to consult doctors online were Tuesdays, Wednesdays, Saturdays, and Sundays, while Saturdays, Sundays, and Mondays were preferred for in-person appointments
To know more about Telemedicine and its evolution post the COVID-19 outbreak, please refer to the report here – LINK
Apollo Tele Health – Teleconsultations during COVID-19
Dr. Ayesha Nazneen, Apollo Tele Health Mr. Vikram Thaploo, Apollo Tele Health
The epidemic of 2019 novel coronavirus (COVID-19) has expanded from Wuhan throughout China and is being exported to a growing number of countries including India. In India, pandemic created unrest amongst the population and uncertainty towards medical services accessibility. Government of India realising the potential of Telemedicine, issued guidelines in March 2020 to address many of the key challenges in providing health services during the outbreak of COVID-19.
Apollo Tele health being the leader in Telemedicine, has created an impact by reaching out to the populace during and post COVID-19 lockdown by providing real time Teleconsultations in 16+ specialties covering 28 states of India. During lockdown, services were provided for COVID-19 screening, counselling, treatment and referral by bringing doctor at their home through Teleconsultations if not would have remained deprived from treatment. Teleconsultation services helped them to overcome the challenge of health services accessibility. The services did not limit to the COVID-19 conditions but largely catered to the patients at risk with other health conditions. It provided equal opportunity to all men, women, children and geriatric population overcoming the barriers of lockdown.
The Public Private Partnership projects with multiple state governments of India, enhanced Apollo Tele Health’s capacity to provide Telemedicine services at government health facilities – UPHCs, PHCs and CHCs to both COVID-19 and non COVID-19 conditions during pandemic and touched 460000+ through Teleconsultations.
Highlighting one of the initiatives from many projects, Government of Madhya Pradesh approached Apollo Tele Health to activate (Sanjeevani Tele Health service) Doc on Call with a dedicated Toll-Free number for the entire population of Bhopal and Indore districts and later extended to all districts of Madhya Pradesh for the month of April and May 2020. It covered health related consultations including suspected cases of COVID-19 and essential Non COVID-19 cases ranging from simple infections to chronic diseases and post-surgical follow ups. The consultations were provided by General Physicians and Specialist doctors. Sanjeevani Tele Health service has been widely promoted by Government of Madhya Pradesh, through local newspapers, digital and social. It started with 9 specialities and later with increased demand extended to 11 speciality Teleconsultation services. Most of the consultations were audio but provision of video consultation was also made available based on patient need and clinical judgement of doctor. Suspected COVID-19 and high-risk cases were referred to Government facilities for immediate action. Total 8,600 patient availed the services from GP and specialist doctors. This service reached out to 12 % elderly and vulnerable population of the total patient who availed services.
Apollo Tele Health’s through one of its service “Doc on Call” provided Teleconsultation and counselling services to 2200+ COVID-19 positive cases and 40000+ suspected cases. It helped them to get treated without stepping out from their home. It also helped them to overcome the myths of COVID-19 and face the challenge with confidence. Non COVID-19 patients benefited at large by taking consultation from home without exposing to the risk of COVID-19. The patient feedbacks were positive, one of the patients said “I am so fortunate to avail Doc on Cell service. It felt very personal and professional. I was impressed that the doctor took time to understand my condition. I never imagined; I will beat COVID-19 through virtual consultations.
Apollo Tele Health has helped to transform and showed the path to deliver technology enabled Telemedicine services during lockdown. The enormous impact Apollo had in lives with treatment and suffering eased during pandemic, further strengthen its commitment to provide Telemedicine services in the years ahead.
The AmbuPod Project: Practical application of robotics in Rural Healthcare in India
Lavanian Dorairaj Director, LYNK AmbuPod Pvt Ltd | Certified HL7 and DICOM Specialist | Past Deputy Director, Medical Services, IAF | director@ambupod.com
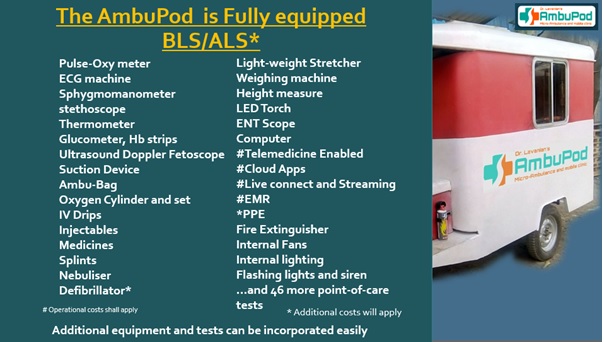
The AmbuPod project is a highly affordable, mass-production model for rural healthcare. It is a telemedicine supported, primary care mobile clinic that provides diagnostic, preventive and curative care along with its own ambulance with a setup cost of less than Rs 1 lakh per village. The ability to provide 6-days-a-week care to EVERY village within its jurisdiction is a powerful capability that is provided by almost no other such project at the price-point of the AmbuPod project.
The AmbuPod is fully equipped with diagnostics, medical and life-saving equipment to cater to mainly primary and preventive care. However, with the advent of 5G and the possibility of real-time remote instrumentation, it is the opinion of this author that the time is now ripe to apply real-time robotic telemedical instrumentation into rural care so as to provide the remote doctor the ability to remotely image, manipulate and, as we gain more experience, actually carry out remote procedures.
Robotics has traditionally been an area of esoteric and expensive research and work and mostly carried out in the US and the UK. The excellent work done by Boston Dynamics, an American engineering and robotics design company comes to mind. This author feels that it is now time to bring such technologies to the common man while also lowering costs to ensure true affordability. India with its numerous IITs and other centres of excellence could support us in this endeavour. If ISRO could successfully launch a satellite to reach Mars successfully in the verry first attempt, and that too, with a budget 1/10th of that spent by NASA for the same job, I do not see why we cannot take remote healthcare robotics to rural India.
We are now reaching out to centres of excellence (CoE) to work with AmbuPod to strategize and design remote healthcare robots to carry out a remote-doctor manipulated examination of the ear, nose, throat, lungs and heart. The proposal is to look for fund providers for this project and support from CoEs for a 2 year pilot utilizing 5G connectivity.
Any organisation interested it working with us on this pilot is welcome to contact this author.
Television for Telemedicine (History and Evolution of Telemedicine – 5th Milestone)
Dr. Sunil Shroff, MS, FRCS, Dip. Urol (Lond.)
President, Tamil Nadu Telemedicine Society of India,
Editor, www.medindia.net,
Consultant Urologist & Transplant Surgeon, Madras Medical Mission Hospital, Chennai, India (shroffmed@gmail.com).
Television was used in an interactive format for medical consultation in 1959 between a state mental hospital and Nebraska Psychiatric Institute through a microwave link. They actually used it for neurological examinations and other information across campus to medical students. They next explored its use for group therapy consultations, and in 1964 they established a telemedicine link with the Norfolk State Hospital (112 miles away) to provide speech therapy, neurological examinations, diagnosis of difficult psychiatric cases, case consultations, research seminars, and education and training. And slowly it was established and recognised as a powerful medium akin to face to face consultation.
However the idea of using television for such consultation emanated the first time in 1927 for a dialysis patient. The patient saw the consultant on one monitor and herself on another (See picture below).
It is thought that Marshall McLuhan may have coined the term coined “telemedicine” He said “time has ceased, space has vanished, we now live in a . . . simultaneous happening. Ours is a brand new world of all onceness.” McLuhan’s argument that broadcast television, as a form of “the most recent and spectacular electrical extension of our central nervous system.”
Electronic media have been the source of a biomedical revolution as much as antibiotics, anesthetics, or organ transplants.
Telemedicine – News from India & Abroad
Apple Watch yields heart data nearly as good as clinical tests, report claims
Apple has been playing a long game in digital healthcare. The main focus – where Apple is right now – CEO Tim Cook recently said , is “…to empower people to own their health.” And as the tools to enable such ownership develop, more opportunity knocks.….. Read More
The rapid uptake of 5G and its real potential
In name it may feel like just one small step from 4G. But the fifth generation of cellular networks is much more than blazing fast mobile broadband. By: Josh Aroner, vice-president: global customer marketing at Nokia.….. Read More
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Design – Sankara Nethralaya Technical Partner- www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Blockchain on the Horizon for Better Telehealth Solutions Dr. B S RATTA Paediatric Surgeon and Urologist, Certified Robotic Surgeon, Ruby Hall Clinic Pune, Fellow Institute of Child Health London, Fellow Texas Children’s Hospital Houston, Trustee Connecting, Past President TSI, Past President TSI Maharashtra, Past Chairman IAeHC, Past President Rotary club of Pune Riverside
Pradeep Goel CEO SolveCare, Past CEO,COO,CIO,CTO, Innovative Technology Co.s, Programme designer Medicare,Medicaid, Entrepreneur of 4 Health IT C
“The science that we work with today must have the innovativeness, foresight and the vision for it to be the centre of technology that we develop tomorrow. In whatever field we work, we have to remain in the service of the common man whose well being is central to all human knowledge and endeavour.”
– Dr. APJ Abdul Kalam
Covid19 has put global economy into a tail spin. There is a big shift taking place in the healthcare industry. Blockchain can create massive social impact in crisis like Covid pandemic. With remote access and telehealth services being sought after to tackle issues such as hospital overcrowding and social distancing, accessibility to digital solutions is more important than ever. However, teleconsultations not only require remote access but a secure way of transferring information from patient to doctor and doctor to patient. This, coupled with the growing usage of mobile health and remote monitoring devices, presents an opportunity to leverage blockchain technology.
Blockchain, at its core, is an infinite and immutable data ledger. The data on a blockchain is stored and repeated onto different unrelated nodes creating a decentralized database that cannot be altered or controlled from any one node. A strict record-keeping technology that provides transparency and auditability by design adds more levels of oversight where issues can be quickly flagged.
Imagine a patient record in hospital or clinic which is written by an indelible ink and is password protected, records names of everyone who has opened ,edited the file is available anywhere, anytime anyplace. It can also integrate data from all types of healthcare services and thousands of healthcare ecosystems working in silos ,like Drs, hospitals, clinics in compliance with strict data privacy regulations.
The emergence of technologies such as blockchain is a game changer for the healthcare industry. This sunrise industry is a market disruptor, Telehealth solutions can be developed to allow for the provision of functionalities and services that are able to assist in making healthcare providers and their work more autonomous. When blockchain technology is used in conjunction with telehealth, it can create the most efficient possible interaction between patients and doctors, ensure the security and privacy of patient data, and most importantly, uphold the sovereignty of physicians.
The true revolutionization of healthcare brought about by implementing blockchain solutions is the ability to empower patients to make better-informed decisions, making the healthcare journey a more patient-centric one. Furthermore, such solutions can automate the enforcement of patient rights and privacy, while providing ownership over their own healthcare data. Data security and control are increasing concerns to patients around the world. Blockchain also allows, with patient consent, for doctors to immediately access a patient’s past medical records, reducing wasted time conducting repeat assessments and unnecessary medical tests. A patient retains access to their segment of data on a blockchain and retains the permission to revoke or track access to that data at all times. Patients don’t have have to entrust the safety of their information to institutions, or any other 3rd party that can be bogged down by having to track thousands, or millions, of patients’ data. This change in how we handle patient data will enhance our abilities in delivering better continuity of care and thereby improve patient outcomes.
The integration of blockchain technology with telehealth services gives us the opportunity to provide real-world solutions that break down barriers between patients, doctors, and institutions, while increasing accessibility and reducing inequality in healthcare. These solutions should be designed to meet the needs of doctors and patients alike, whilst minimizing paperwork and bureaucracy and respecting the rights and privacy of both parties. The need for greater patient empowerment and respect for the sovereignty of physicians has never been more pronounced. Access to quality healthcare should not be restricted by geographical, societal, or administrative barriers.
This is one of the great opportunities of our time, and it is up to us in the medical profession to ensure it reaches its full potential for the benefit of those who depend on us for their healthcare.
Privacy and Digital Health in India
Bagmisikha Puhan, Member, EC – TSI Associate Partner, TMT Law Practice, C-2/39 | Safdarjung Development Area New Delhi – 110016 | India.
The digital health ecosystem in India found a fillip last year, and ever since, the industry has been generating and consuming large volumes of personal as well as sensitive personal data. This has led to increasing concerns amongst the end users who are submitting their data to the digital platforms who are facilitating remote delivery of health care services and are fostering continuity of care.
With a rise in the number of people opting for at-home diagnostic services, and a rise in the number of tele-consults which are being opted by the end users, there is a pressing need to address the inadequacies of the present data privacy framework. While the present framework outlines the basic requirements, which are essential for compliance, they do not provide sufficient safeguards for the protection of all the information which is flowing through the entire ecosystem.
Simply put, while the Telemedicine Practice Guidelines (TPG) have provided a basic guiding element with respect to the procedure to be followed to preserve privacy of a patient, they do not provide a framework within which the same must play out. Additionally, the TPG carries a template for prescription, and the identifiers that can be captured therein, are extremely exhaustive in nature, and may lead to complete disclosure of a patient’s health and medical information when it is being shared on a third-party digital platform or is being shared with a pharmacy. Issues around this will continue to influence the minds of the consumers who are willing to realign their preferences with the digital world. As a consumer intends to move towards a digital based ecosystem, they might find the lack of a comprehensive legislation under which they can seek redressal, unsettling, which in turn will deter the geometric flourishing of the entire sector.
Under the pending Personal Data Protection Bill (PDP Bill), the entire life cycle of a person’s health information is being captured. As it is oft-put, digital health ecosystem has built a situation where the entire life cycle, that is the journey from the womb to the tomb, can be mapped out by the information fed to the digital systems. The PDP Bill promises safeguards and accounts for scenarios which are related to emergency situations, as well as continuity of care.
To surmise, the PDP Bill premises itself upon a nearly homogenous ecosystem, which is also allowing for interoperability. This is being supplemented by the expected National Digital Health Mission (NDHM), and the policies issued thereunder. The PDP Bill in conjunction with the NDHM will be in a position to bring in a certain degree of uniformity in the compliance conditions, in re the expected behavior on the part of the healthcare organizations, healthcare providers, and will also clarify on the obligations that the data subject is to be comply with. While the entity which seeks information is expected to ensure that the data available with them is accurate and updated, the onus in provisioning of such information is on the data subject or the patient who has to ensure that they are providing the information which is commensurate and essential for the healthcare service provider to address the concerns and medical situation of the patient.
The PDP Bill features exceptions whereby sensitive personal information of a person may be processed without the explicit consent of the patient for scenarios where vital interests of the end users must be preserved. The extreme caution and safeguard afforded to the elevated status of sensitive personal information are with the view that the end user must not be discriminated against on the grounds of any inherent bias or prejudice on the basis of inappropriate or unauthorized usage of sensitive personal information. It is with these concerns in mind that service providers, system participants and service recipients are waiting for the legislative framework with bated breath.
Telemedicine Enabled Clinics with Last Mile Healthcare Delivery
Doorstep Health Services (DHS) along with its Technology Partner- Remassis Solutions-is proud to announce the opening of its first Telemedicine enabled health centre in the North East -at Agartala.
While earlier concentrating around Pune, the dream is to provide accessible responsive care with last mile delivery across India-with a chain of clinics where the nurse is continuously supported by the Doctors on Telemedicine.
The model is a Hub and Spoke model which works under the overall direction of the Enterprise. The Enterprise undertakes forecasting, planning, organizing and such higher management functions. It analyses and evaluated data, creates linkages with secondary and tertiary care, develops training modules, standard treatment guidelines etc. The hub provides doctor consultations and technical support to multiple spokes via telemedicine. The spokes are at the grass roots. The spokes work like health centres and are managed by a Nurse or care giver (if nurse is unavailable). The nurse besides managing the health centre, executes the instructions of the doctor, provides measurements, takes blood for investigation, does ECGs and even conducts home visits for patients who need it.
DHS believes that Telemedicine and last mile healthcare together are the most comprehensive way to provide better health in underserved communities. While telemedicine is important for improving access, responsiveness, retrievability and documentation, last mile health care delivery is crucial for timely initiation of treatment and support in terms of investigations and medication. Last mile delivery also helps provide the human touch which is so important and integral to patient care.
The model works not only in the rural space, but extremely well in urban areas-which also suffers due to lack of primary care. Urban areas have an advantage as lack of infrastructure, human resource, sociocultural mindsets, language, literacy and other such barriers are less encountered here.
We look forward to work with companies, CSR projects, hospitals, and like-minded philanthropists to make our dreams a reality.
For more information about us please visit www.doorstephealth.in or email care@doorstephelth.in
Dr (Gp Capt) Suchitra Mankar Founder Director Doorstep health Services, Pune, India. suchitramankar@gmail.com
Radio & Marine Telemedicine (History and Evolution of Telemedicine – 4th Milestone) Dr. Sunil Shroff, MS, FRCS, Dip. Urol (Lond.) President, Tamil Nadu Telemedicine Society of India, Editor, www.medindia.net, Consultant Urologist & Transplant Surgeon, Madras Medical Mission Hospital, Chennai, India (shroffmed@gmail.com)
In the evolution of telemedicine radio has played a significant role and has had an impact on saving lives of marooned sick marines on ships. For any big development or revolution to happen, there needs to be simultaneous multiple smaller revolutions. Similarly for marine telemedicine to happen the development of radio-telegraphy by Guglielmo Marconi in 1897 was important. This was soon followed by erection of coastal radio stations and the introduction of radio equipment on ships. For more than 100 years several radio medical services have provided and radio signals and Morse code have been used to help the sick.
On January 2, 1911 Captain McGray of the steamer Herman Frasch was stricken with serious ptomaine poisoning. A member of the crew asked the USA naval base 100 miles away to help but his message was received on board the Merida, which was 800 miles away. The surgeon of this ship gave his recommendations, thanks to which the captain was given the correct medicine and recovered quickly. This improvised teleconsultation occurred between the two vessels.
In 1920 Norway, used radio teleconsultations for seamen. Physicians not only made remote diagnoses and recommendations for treatment but also guided complicated surgical operations via Bergen Radio.
On November 3, 1920 Robert Huntington organized the service for radio consultations at sea for crews of merchant vessels. Captain Robert Huntington used to say: “It does not matter, where a vessel can be, after a captain asks for help over the radio, an ill seaman can get the most qualified medical consultation within 13 minutes“.
The first license for a radio medical service to ships was issued on November 18, 1920 to the Seamen’s Church Institute in New York and this service was called “How to help seamen Needing Medical Help.”
The first experience of radio medical assistance from a domestic to an international level occurred in Italy in 1935, with the constitution of the Centro Internazionale Radio Medico (International Radio Medical Centre, CIRM).
In 1958, the International Labor Organization (ILO) issued a Convention requiring all seafaring nations to have a service for radio medical advice to ships. The ILO Convention of 1987 released an important document that states that sailors should have health protection and access to medical care. The ILO Convention of 1987, art. 9 states that: “If one ship does not have a doctor, one or more people should be designated with specific duties and responsibility, such as medical care and administration of drugs as part of their normal functions. ‘Moreover, a person responsible for medical assistance on board…, who is not medical doctor’, shall have satisfactorily completed a course, theoretical and practical in medical skills, recognized by the competent authority”
Ship-to-shore transmission of electrocardiograms (ECGs) and x-rays was first reported in 1965. Marine telemedicine may offer some solution in providing to cross border telemedicine guidelines in the future.
.
Access the Latest News on Telemedicine and Telehealth
This is another source for the Latest News on Telemedicine and Telehealth that is brought to you by our TSI member Dr. Lavanian Dorairaj.
Each news article is carefully and painstakingly distilled from reliable sources from across the world, by actual human beings. We pride ourselves in providing focused and human-curated news. There are no BOTs or impersonal Algorithms involved here. We put in hours of hard work to ensure that YOU do not have to work hard.
‘Telemedicine can help treat lockdown sleep syndrome’
TNN | Jan 10, 2021, 04.20 AM IST Printed from Chennai: Telemedicine can provide uncompromised care to existing patients and also help identify and manage the onset of new sleep problems, says a new study ‘Tele-Sleep Medicine: An Opportunity In A Crisis’ conducted by Dr N Ramakrishnan, director, Nithra Institute of Sleep Sciences. It also documents the emergence of ‘Lockdown Sleep Syndrome’, ie, the onset or worsening of sleep disorders often related to inactivity, fear of the disease, and generalised anxiety caused by the uncertainty of the future….. Read More
Teleradiology Solutions announces reporting volumes and revenue bounce back post pandemic
3 February 2021 BENGALURU, India, Feb. 3, 2021 /PRNewswire/ — Teleradiology Solutions, a leading provider of teleradiology services, reports its volumes, which had seen business shrunk by 80% of pre pandemic volumes, have almost returned to normalcy.….. Read More
International
In-person medical visits waning because of COVID-19 safety concerns MORGANTOWN — Morgantown’s two largest health care providers –WVU Medicine and Mon Health – said people should not be afraid to seek medical treatment because of the pandemic. “If you have a chronic condition, don’t put off your care,” said Dr. Michael Edmond, WVU Medicine’s chief medical officer.….. Read More
Global Telemedicine Market- Industry Analysis and forecast 2027: Product Type, Shape, Operating System, End-Users and Region Maximize Market Research has recently published a “Global Telemedicine Market 2019 Industry Research Report. It is comprehensive analysis of past and current status Telemedicine Market’ with the forecast till 2027. The report covers the past market from 2017 to 2019 and forecast of 2020 to 2027 with key developments, key trends, M&A activities by value and their strategic intents. The report has analysed complex data and presented in simple format to make it easier to understand… Read More
Doctor visits online not expected to end following pandemic The coronavirus pandemic brought with it a boom of doing things virtually — education, work, happy hours and even routine doctors’ visits. While some have returned to in-person school and work days, medical experts told the Dayton Daily News they expect telemedicine will stick around long after the pandemic ends.….. Read More
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Design – Sankara Nethralaya Technical Partner- www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
In continuation to the Dec2020 issue this issue is covering highlights of a few sessions of The TELEMEDICON 2020
TELEMEDICON2020 – Highlights ‘From the Fringes to the Mainstream’
TELEMEDICON2020: Highlights of a Some Sessions By Dr.Sheila John
The TELEMEDICON 2020, the 16th International Annual Conference of ‘Telemedicine Society of India’ was conducted from 18th December to 20th December, 2020. This was the first International level Tele-Health conference after the Govt. of India’s notification of ‘Telemedicine Practice Guidelines’ during this ongoing COVID pandemic.
The three-day web conference was organized by the Tamil Nadu, Delhi-NCR, Rajasthan, Maharashtra and Karnataka chapters. The virtual conference attracted over 1200 participants across India and abroad.
The first session was “CME – COVID Pandemic and Telehealth Challenges in India” and was chaired by Dr. Meenu Singh and Mr.Bijoy, and the Moderator was Dr. Umashankar Subramaniam. Dr. Susheel Oommen John discussed “Digital health interventions for COVID19 public health response”; Dr. Naveen C Kumar spoke on the topic of “Mental Health and Telepsychiatry”; and Dr. Anoop Amarnath spoke on “Telemedicine During Covid 19 – The Karnataka Experience.” Dr.B.N Mohanty spoke about “Telemedicine Activities in Odisha during Covid-19 Pandemic”; and Dr. Sangeeta Desai spoke about “Coronation of Digital Pathology during Corona pandemic.”
The second session examined “CME – Data Breach.” The session covered “Cyber Security for doctors – Basic Precautions and how to keep consultations and records secure.” The session was split into 2 sections with a 20 minutes section devoted to how and why doctors are targeted, and basic information on “Cyber Security For Doctors.”
The second section was chaired by Dr. Krishna Kumar, Dr. Ikramullah and moderated by Mr. Manick Rajendran. The panelists, Cmdr. K. K. Chaudhary, Lt. Col (Dr.) T.K Das, and Mr. Alok Jha discussed on the topics of “Laws and implications on what is relevant for Doctors,” “Precautions and how to keep sensitive data and records secure,” “Best Practices for Doctors,” and “What is “Due Diligence” and how can it help.” A third section was a Q & A session open to the audience.
Col. (Dr) Ashvini Goel (Retd ), President Elect spoke about “Telehealth Standards – Work in Progress.” Dr. Anup Wadhawan, IAS, Commerce Secretary to the Government of India discussed the merits of “Telemedicine and its Role in Leveraging Healthcare Economy” and “Inauguration of Virtual Exhibition.” The session was presided over by Dr. A. K. Singh and Col. (Dr.) Ashvini Goel (Retd.) and moderated by Mr. Vimal Wakhlu.
Dr. S. Prakash, MD at Star Health and Allied Insurance, also spoke on the topic of Health Insurance Reimbursement for Telehealth.
Some international speakers of note were: Prof Thais Russomano (UK), Russomano, Co-Founder & CEO, InnovaSpace UK; Prof. Pramod Gaur (USA), Prof. Pramod Gaur, Pace University (former VP of Telehealth at UnitedHealth), New York, NY; and Mr. Pradeep Goel (Ukraine), CEO Solve.Care.
The sense of urgency created by the COVID-19 pandemic has spurred medical establishments to overhaul their healthcare delivery systems in pursuit of maximizing patient care and minimizing the risk of infection.
CME on Cyber Security for Doctors and Medical Staff
By Cmdr. K. K. Chaudhary, Lt. Col (Dr.) T.K Das, Mr. Alok Jha
Due to the highly valuable information in medical industry, patient health data (PHD) has become the prime target of hackers. Hackers are continuously trying to breach the defense of hospitals and medical facilities to harvest the information of patients and doctors. As per the statistics, patient health data is sold in Dark Web at 10-20 times the premium of financial data.
Some of the biggest healthcare data breaches of 2020 that forces us to deliberate more seriously on the safety of PHD are
• Inadequate Security, Policies Led to LifeLabs Data Breach of 15M Patients • Magellan Health breach of 365,000 patients • Dr Lal PathLabs leaks millions of patients data in public domain
According to Telemedicine Guidelines 2020 – Govt of India “it is doctor’s responsibilities to ensuring data privacy, ethics, and maintaining records of all the patients whose records are being collected during medical examination”. Similarly Digital Information Security in Healthcare Act (DISHA), which is in draft stage of formation and the personal Data Protection Bill-2019 have placed the onus of security of patient’s data on those who store and handle such data.
The relevant part of the amendment is as follows:
3.7.1 Medical Ethics, Data Privacy & Confidentiality: Principles of medical ethics, including professional norms for protecting patient privacy and confidentiality as per IMC Act shall be binding and must be upheld and practiced.
3.7.1.2 Registered Medical Practitioner would be required to fully abide by Indian Medical Council (Professional conduct, Etiquette and Ethics) Regulations, 2002 and with the relevant provisions of the IT Act, Data protection and privacy laws or any applicable rules notified from time to time for protecting patient privacy and confidentiality and regarding the handling and transfer of such personal information regarding the patient.
3.7.1.3 Registered Medical Practitioners will not be held responsible for breach of confidentiality if there is a reasonable evidence to believe that patient’s privacy and confidentiality has been compromised by a technology breach or by a person other than RMP. The RMPs should ensure that reasonable degree of care undertaken during hiring such services.
With reference to the above, the speakers highlighted why it is important for doctors to understand the underlying risk of holding PHD.
• Patient data can be stolen, lost or intentionally or un-intentionally transmitted. • Why custodians of DHD & PII are bound by National (DPDA/DISHA) and International (HIPAA) regulations • Intent and Pre-emptive action that can help • For this Awareness about basic digital Hygiene is very important • Ignorance of underlying technology of Internet • Connected to Internet-based Health Equipment
Speakers also highlighted various methods/tricks, such as Phishing, Vishing, Mail/Phone spoofing, Social Media Postings, Hacking computers/smartphones and Hacking the Internet-connected equipment.
It was concluded that the only safety for any medical practitioner in case of a data breach happens, is to prove that due diligence was done and all possible care to protect such data were taken by the data custodians. Hence, it is essential that doctors and medical staff must be aware of simple security steps can not only prevent a data breach but also prove ‘due diligence’ in case of such breaches.
Release of TSI – PRACTO Joint Report on Reinventing Health Care Delivery Telemedicine During the COVID-19 Pandemic
On the 19th Dec a report to provide a glimpse of telehealth consultation during the COVID pandemic was released jointly by Telemedicine Society of India (TSI) and Practo in presence of Maj Gen (Dr) AK Singh, President, Col (Dr) Ashvini Goel (Retd), Dr.Girdhar Gyani, Director General, AHPI, Dr.Vijay Agarwal, President, CAHO and Dr. Alok Roy, Chairman, Medica Group Hospitals
This was a 25 page document and the key Insights included the following:
• Physical appointments went down by 32% o Visits to secondary care specialists like neurosurgeon, somnologist, cardiologist and oncologist grew dramatically
• 3x increase in the number of people using online consultations o 26% of the consultations were with GPs, followed by Dermatology (20%) and Gynecology (16%) and others like Gastroenterology, ENT, Pediatrics stood at 7% each o The fastest-growing health concerns included ophthalmology, ENT, orthopedics, pediatrics and gastroenterology o Delhi, Mumbai, and Chennai – saw an average of 16x growth in queries for ENT specialization
• Non-metros saw the highest growth of 7x in online consultations, as compared to the same period in the previous year o During the same period last year, the split between metro:non-metro consultations stood at 75:25. This year, it is 60:40, demonstrating that the number of consultations from non-metro cities is on the rise o Tier 2+ cities like Manjeri, Arrah, Balasore, Etah, Orai, Khopoli, Jagtial and Shivpuri used telemedicine for the first time in this time period o Cities like Meerut, Jammu, Srinagar, Nellore, Kochi, Gorakhpur, Kakinada, Tirupati, Bhagalpur, Gaya and Shimoga recorded a 10x growth
• Among metros, Chennai witnessed the highest growth of 4x as compared to the previous year o Bengaluru, Delhi-NCR, Mumbai, Pune, Hyderabad and Kolkata grew by more than 300% as compared to last year
• More and more elderly people are now getting used to technology o There was a 502% spike in online consultations from people above the age of 50 during this crisis, who contributed to 12% of overall consultations, as compared to just 5% the previous year
• More women are going online o Last year the men:women ratio stood at 75:25, while this year it’s 68:32 o Gynecologists and General Physicians were two of the most consulted specialists by women in 2020
• Online mental health consultations and queries continued to rise during this period o There was a 302% increase in overall mental health-related queries o Women contributed to 33% of overall queries for mental health specialists
• More consultations at late hours o 25% of online consultations were recorded between 10 pm and 4 am when people are not burdened with work responsibilities o One of the top specialties consulted during late-night hours was Psychiatry
Preferred day(s) to consult doctors online were Tuesdays, Wednesdays, Saturdays, and Sundays, while Saturdays, Sundays,and Mondays preferred for in-person appointments.
Training for Telemedicine in India for Registered Medical Practitioners – Seminar
By Dr. Sunil Shroff, Ms. Bagmisikha Puhan, Wg Cmdr (Dr) Lavanian Dorairaj (Retd), Mr. Mayank Agarwal, Mr. Manick Rajendran, Dr. Ravi Modalli, Dr. (Gp Capt) Suchitra Mankar, Mr. P Ramkumar
This important session provided an overview of training conducted for registered medical practitioners (RMP’s) by Telemedicine Society of India (TSI) after the announcement of the Telemedicine Practice Guidelines (TPG) on 25th March 2020 the Board of Governors in supersession of the Medical Council of India. These Telemedicine Practice Guidelines, were subsequently notified by the government as a gazette on May 14, 2020, as an amendment to the Indian Medical Council. The regulation requires all medical practitioners intending to practice telemedicine in India to take an online course and get certified within three years from the date of notification.
Training of 1.1 million RMP’s in India poses a huge challenge and to address the issue of training in telemedicine, a course called “Train to Practice” was designed by the TSI. This project was voluntary efforts by the members of the society though online structured webinars and was helped by a member (Dr.P.Ramkumar) offering his education platform to house the activities. It was announced within two weeks after the TPG was announced . TSI executive body with senior members designed four modules for training of RMP’s to get familiar with the guidelines and use it to follow ethical and safe standards of practice of telemedicine as a means to increase their outreach and foster increased access to healthcare.
The candidates had to register and create an account. Once this was done they were expected to take a pre course quiz to assess their knowledge about telehealth. This was followed by 150 minutes of an online face to face course that had four modules and these included – Module 1: Legal Aspects & Telemedicine Module 2: Clinical Aspects & Telemedicine Module 3: Tele-triage & Telemedicine Module 4: Technical Application & Telemedicine
Each module was delivered as a lecture for about 20 to 30 mins and this was followed by a question answer session. Once the face to face webinar course was over the participants were provided with post course assessment and finally if they obtained 80% marks a certificate of completion of the course was issued. The course also put together FAQs that went through several stage of iterations before being given out to the trainees as a reference document and could be used at any time before they took the online test or afterwards as a reference document. A feedback form was also included at the end of the course.
There were 35 training sessions that were conducted in 6 months from April to Sept 2020. Majority of 80% were offered free (28/35) and a small number or 20% were paid or sponsored sessions (7/35). 2946 candidates took the course. The total time spent for the delivery of the course by the faculty was 142 hours. Four sessions were also undertaken free of cost, to train the Army Medical Corps medical officers and specialists.
The total monetary value of the course was Rs.3.74 Million (or US$ 51,233 ). Most of the course was subsidised and offered free. There were seven paid or sponsored sessions that paid the society Rs. 0.84 Million ( US $ 11,507 ) . The course was subsidised by Rs.2.9 Million ( US $ 39,726 ). The overall rating from the course was 4.7 out of 5.
The training course was the first of its kind course in India and was received enthusiastically by all the doctors who came from different specialities. The level of knowledge on telemedicine was variable and most had some basic understanding of the subject. Most RMP’s were not sure if cross state tele-consultations required registration with other states. Most were anxious to understand the legality of telehealth consultations.
Further modules are to be developed in future that would cover common medical specialities that use telemedicine along with a few topics of general interest to include diabetes & telemedicine, Cardiology & Telemedicine, Paediatrics & Telemedicine, Obstetrics – Gynec & Telemedicine, Home-healthcare & Telemedicine, ICU and Telemedicine, Recent Advances & Future of Telemedicine, Legal Cases in Telemedicine and Standards for software and Hardware.
Teleophthalmology Symposium – An overview
By Dr. Sheila John
The COVID-19 pandemic dealt a big blow to the healthcare sector worldwide. With everyone concentrating on managing the pandemic, patients with non-COVID-19 diseases suffered due to a dearth of healthcare access. Previously reserved for underserved areas, tele-health now has become mainstream now because the pandemic has left a vast majority of people remote and underserved.
Dr.R.Kim, Chief Medical Officer, Senior Medical Consultant, Retina & Vitreous Services, Aravind Eye Hospital, Madurai took the podium for the afternoon session of day 1 of the virtual meet. He spoke about the importance of Tele- screening for Retinopathy of Prematurity. Retinopathy of prematurity (ROP) affects developing retinal vessels in premature infants and can lead to severe and irreversible visual loss if left untreated. Screening of the premature babies is the first step in ROP management. In India, tele-screening techniques can bring premature babies from both urban and rural areas into the screening network.
On day 3, the twelfth session featured a symposium on Tele -Ophthalmology (Parallel Session) Dr.R.Kim was the moderator of the session. Dr. Sheila John discussed the topic of “Teleophthalmology to reach the unreached – Mobile Teleophthalmology.” The major role in this endeavor is to provide an ophthalmic service to remote rural areas, where people cannot afford to go to a hospital because of unawareness and poverty. In remote rural areas, ophthalmic services are nearly impossible. The teleophthalmology unit can be a very useful tool to improve eye care delivery in rural areas.
Dr. Kim is the director of Arvind’s telemedicine network and IT services. He discussed “Teleophthalmology to reach the unreached – The Vision Center Model,” In a lot of developing countries, teleophthalmology enables ophthalmologists to provide good eye care to the unserved remote rural and underserved urban populations. Technological innovations through the years have led to advances and teleophthalmology has progressed from a research tool to a clinical tool.
Dr. Padmaja Kumari Rani spoke about ‘Teleconsultation experience in the COVID Era.” The COVID-19 pandemic dealt a big blow to the healthcare sector worldwide. With everyone concentrating on managing the pandemic, patients with non-COVID-19 diseases suffered due to a dearth of healthcare access. Previously reserved for underserved areas, tele-health has become mainstream now because the pandemic has left a vast majority of people remote and underserved. During the pandemic crisis, there was an almost 500% surge in online consultations from people above the age of 50. Older persons accounted for over 10% of overall consultations, as compared to just 5% the previous year.
Padmashri Prof. Dr. S. Natarajan, is renowned for his skills as a vitreoretinal surgeon, keen academic mind and for his philanthropic initiatives in prevention of blindness. He spoke on the topic of “Offline AI using a Smartphone for Diabetic Retinopathy (DR) Screening. India has pioneered the development and validation of artificial intelligence-based algorithms in DR. Likewise, the study done by AJFTLE has shown promise in the use of an offline AI system in community screening for referable DR with a smartphone-based fundus camera and it is a practical way to provide more patient satisfaction as it saves time and cost.
Dr. Senthil CEO welcare system discussed about the various business models for Teleophthalmology like Teleconsultation, ROP Screening, Diabetic Retinopathy Screening and Tele refraction. Diabetic Retinopathy Screening has been the most successful model and he discussed in detail regarding the implementation and outcomes has been followed by Welcare system. The business model has been implemented at 275 Locations and they have screened more than 12.5 lakh patients.
The keynote on Tele-Ophthalmology was provided by Prof. Mingguang He is Founding Chairman, Asia-Pacific Tele-Ophthalmological Society, Managing Director, and Asia-Pacific Academy of Ophthalmology. Cataract, glaucoma, age-related macular degeneration, diabetic retinopathy, and retinopathy of prematurity are among the common causes of blindness in many countries. The session was moderated by Dr. T. Senthil, Dr. Gunda Srinivas, Dr.Vikas Gaur, and moderated by Mr. Mayank Agarwal.
Teleophthalmology, the branch of telemedicine that delivers eye care through digital medical equipment and telecommunications technology, includes access to eye specialists for patients in remote areas, ophthalmic disease screening, diagnosis and monitoring; as well as distant learning.
TELEMEDICINE IN DIABETES CARE Symposium
Dr. Jothydev Kesavadev, Dr. Mohan V, Dr. Sanjay Sharma
The first talk by Dr.V.Mohan covered Experience with Telemedicine for Diabetes during Lockdown (COVID-19).
The COVID-19 had played havoc on the health care sector globally. The hurdles imposed by COVID-19 restrictions on health care professionals were discussed among the diabetics especially among the high-risk group of COVID-19: type 1 and type 2 diabetes patients, adults above 65 years of age, people with multiple comorbidities, unstable HbA1c ≥8.5% and smokers.
Telemedicine helped provide a relief for diabetes care.. The study by Dr. Anjana et al on the ‘acceptability and utilization of newer technologies and effects of glycemic control in type 2 diabetes: lessons learnt from lockdown’ conducted in 3000 subjects summed up the challenges, acceptability and utilization of telemedicine in diabetes patients. Research outcomes highlighted that 82% of the patients who adhered to telemedicine were satisfied with the telemedicine services, out of which 58.1% is interested to continue the telemedicine services in the future. There was a significant improvement in clinical and biochemical parameters in diabetes population during lockdown. During the lockdown, the number of patients performing SMBG increased from 15.5% to 51.3% which led to a significant improvement in glycemic control and other metabolic parameters. Take-home message included:
The challenges imposed by Covid-19 restrictions include lack of motivation to monitor blood glucose, reduced access to lab testing, ineffective implementation of a healthy lifestyle such as improper diet and lack of exercise, insufficient guidance and awareness and spread of fake news and fear which in turn affect their quality of life.
Telemedicine is a proven treatment modality for diabetes care.
Effective implementation of telemedicine can result in a significant improvement in glycemic and other metabolic parameters.
The second talk was on Dr. Jothydev Kesavadev covered 23 Years of Telemedicine Practice in Diabetes its merits and demerits.
Diabetes Tele Management System (DTMS®) was launched in 1997 with an intention to better manage diabetes when the prevailing status of care was disappointing with an average A1c above 9%. By way of successful partnership with technologies, over the next ten years, DTMS® evolved into a decision support system; the major components being electronic medical records, personalized diabetes care and a multidisciplinary team consisting of trained physicians, nurses, dietitians, diabetes educators, pharmacists and psychologists. Telemedicine in diabetes care was not widely accepted due to several challenges which included funding, the reluctance of patients to pay, long duration of consultations etc.
Effective use of telemedicine resulted in more than 86% of the patients successfully reaching the customized targets of A1c, Evidence demonstrated significant reduction in A1c without hypoglycemia, preventing the progression of diabetic kidney disease, sustainable benefits for over 15 years, prevention of microvascular complications, benefits regardless of the geographical location and above all cost-effectiveness.
The key take-home message included:
Diabetes is the most important non-communicable disease where the expensive complications can be successfully averted with the implementation of telemedicine.
Telemedicine in diabetes care will invariably help in reaching targets when conventional therapy is failing in the majority.
Sufficient evidence from India proves the superiority of telemedicine in diabetes over conventional care.
There is a robust reduction in cost and complications. However, hospitals and doctors need to be adequately compensated for their time and services for the sustainability of telemedicine in diabetes.
Third party platforms for telemedicine need to be engaged cautiously due to fear of breach of confidentiality and probable commercial interests.
The third talk covered ‘Tele Wound Care for Diabetes Foot Ulcer. By Dr. Sanjay Sharma
Tele wound care was critical in India as the statistics reveal that there are 120 million people in more than 60 age group and 1 in 5 has diabetes. Approximately 22 lakh patients have diabetes foot ulcer and about 500 lakhs require wound dressings.
Diabetes foot care is worsened by the unexpected outbreak of COVID-19 which posed logistic and travel challenges and needs special attention as even the slightest negligence may raise the number of leg amputations.
On an average, to heal a chronic wound, it takes 12-28 weeks and may go up to 52 weeks, which ultimately results in 24-84 clinic visits. These numbers emphasize the necessity for implementing tele wound care for diabetes foot care; the advantage being effective utilization of technology to guide patients to manage wounds at their dwelling places.
Development of various apps such as Foot 360 and Wound360 and its integration to existing therapeutic measures paved the way for patients to share the information regarding their wound such as size, nature, associated complications and the images. The challenges in tele wound care in Indian scenario lies in the willingness and perseverance of physicians, patients, and caregivers in accepting the technology, skill of the patient/caregiver, patient’s environment at home, nutrition status, family and care support.
Take-home message included:
The effective management of diabetes is possible with the advent of cost-effective technologies.
Diabetes foot ulcer is a major diabetes complication leading to increased number of leg amputations.
Tele wound care and apps support patients and health care professionals to have better treatment outcomes with reduced face-to-face consultations.
Panel Discussion on DIGITAL AYUSH
By Moderator, Arjun Bhaskaran, Country Manager – India & Middle East, Gamasec, Israel
The panel on Digital AYUSH discussed the possibilities, constraints, way forward for implementing the Telemedicine Guidelines from CCIM, CCH, CCRYNS in AYUSH sector. The key points discussed were:
With the acceptance of Yoga under the United Nations, the potential for providing Telemedicine in Yoga is immense. This along with the wide presence on the NRI diaspora, the potential for accelerating AYUSH telemedicine for NRIs needs to be urgently leveraged.
AYUSH being rooted in Socio, cultural settings can provide low-cost, medical interventions and guidance for 3 million expatriate workers in Middle East in vernacular medium like Ayurveda Telemedicine in Malayalam and Siddha Telemedicine in Tamil to 2 million NRIs in Malaysia, Singapore.
AYUSH Telemedicine could make a strong beginning with AYUSH Medical Colleges as Telemedicine Providers. AYUSH Colleges have experienced Faculty to deliver Telemedicine, as per the guidelines on CCIM, CCH and CCRYNS.
AYUSH PG & UG students are digital-natives who will adopt and evangelize AYUSH telemedicine faster.
With the Insurance Regulatory & Development Authority making it mandatory from April 2020 for all insurance companies to provide 100% coverage in Sum Insured for AYUSH under AROGYA SANJEEVANI Scheme, AYUSH Telemedicine will get a big boost from Insurance. AYUSH Telemedicine can play a key role in achieving Universal Health Coverage.
AYUSH can leapfrog in Telemedicine, EMR as it has very few baggage IT systems.
There is a need for a strong IT Platform run by a Neutral, Credible Market Aggregator to promote AYUSH Telemedicine. Care needs to be taken to ensure adequate visibility is provided in the IT Platform for all credible, experienced AYUSH doctors, all of whom may not be market-savvy or technology-savvy to promote themselves in Social Media.
The panel identified Bangalore, Kerala and Chennai as suitable Telemedicine ecosystems to implement Proof-of-concept Telemedicine practices – Kerala has state-wide acceptance of AYUSH as mainstream medicine, Bangalore has over 10+ AYUSH medical colleges and a vibrant AYUSH clinical practice, Chennai has the strong support of Tamil Nadu Government in promoting Siddha.
The panel recognized that AYUSH Telemedicine should steer clear of COVID19 related controversies and complications.
Virtual General Body Meeting of Telemedcine Society of India
For the first time in the ere of new normal Telemedcine Society of India held its meeting virtually. There was enthusistic participation by the offcie bearers and members of the society.
Announcements
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Design – Sankara Nethralaya Technical Partner- www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
The December issue of TN-TSI Newsletter is dedicated to TELEMEDICON2020
TELEMEDICON2020 – Highlights ‘From the Fringes to the Mainstream’
The 16th International Annual Conference of ‘Telemedicine Society of India’ (TELEMEDICON2020) was held virtually from the 18th December to 20th December, 2020. This was the first International level Tele-Health conference after the notification of ‘Telemedicine Practice Guidelines’ by the Govt. of India in this ongoing COVID pandemic.
Since Lucknow could not do a physical conference due to the ongoing pandemic, it was decided to go ahead with a virtual meeting and Tamil Nadu chapter along with four other TSI state chapters which included Delhi-NCR, Rajasthan, Maharashtra and Karnataka took up the responsibility and mandate to conduct this web conference. The time was very short and the task herculean,however due to cooperation from many this was accomplished successfully.
As an organising body we created various committees and the scientificcommittee met over six times to put forward a compelling program with an objective to capture the essence of the theme of the conference on how Telemedicine in India had moved from the very ‘Fringes to the Mainstream’ within a very short span of few months.
Scientific committee Meeting on Zoom
The Conference was graced with the stellar presence of Hon’ble Justice of Supreme Court ShripathiRavindra Bhat, Mr. AnupWadhawan, IAS, Secretary, Ministry ofCommerce and Industry; Dr. Vinod KPaul, Member, NITI AAYOG; Dr Dharmendra Singh Gangwar, IAS, Addl. Secy. & Fin Advisor Min of Health &Family Welfare; Mr. Lav Agarwal, IAS, Jt. Secy., Ministry of Health and Family Welfare; Dr.SoumyaSwaminathan, Chief Scientist, WHO, Lt Gen ( Dr) MadhuriKanitkar;Ms. VandanaGurnani, Addl. Secy. and Mission Director of the national Health Mission at theMinistry of Health and Family Welfare, Government of India; Mr. Frank Lievens ( Belgium),ISfTeH Executive Secretary (Switzerland) and Dr.Prof. Thais Russomano (UK),Space Physiology, Aviation Medicine, Telemedicine & Digital Health Co-Founder & CEO, InnovaSpace UKamongst others.
The presidential Oration was delivered by President Maj Gen (Dr) AK Singh (Retd.)and he spoke about his experience over the years in the Telehealth space in India.
The chief guest for the inauguration Dr. Vinod KPaul, Member, NITI AAYOG, spoke truly from his heart and gave a message of hope and spoke about the responsibility that had been bestowed on the medical fraternity for creating a tele-health ecosystem as a new enabler for providing affordable access to universal healthcare in India.
Chief Guest for Inauguration function of TELEMEDICON2020Dr. Vinod KPaul, Member, NITI AAYOG delivered his chief guest address.
Dr Dharmendra Singh Gangwar, IAS, Addl. Secy. & Fin Advisor Min of Health & Family Welfare delivering the Keynote address. He inaugurated the Virtual Exhibition for TELEMEDICON2020
Presidential Oration by Maj Gen (Dr) AK Singh (Retd.)
Dr. B.N Gangadhara, Chairman, Ethics & Medical Registration Board, National Medical Commission gave his keynote address on ‘Emerging Ethical challenges in Digital Health’
Mr. Lav Agarwal, IAS, Jt. Secy., Ministry of Health and Family Welfare delivering his keynote address at the Valedictory Function on the Way Forward for Telehealth. He also released the Telemedicine Practice Guidelines FAQ’s for Medical Practitioners from TSI.
Synopsis of Presidential address
Maj Gen Dr. A K Singh (Retd.) President
In his own words –
The year 2020 has been a very tough year for all of us but for Telemedicine Society of India it has been a year where the TSI has trained over 15,000 Doctors after the Telemedicine Practice guidelines were issued by the board of governors (MCI).
The training team led by Dr Sunil Shroff curated a very comprehensive training programme. What I have realised is that majority of TSI members are indifferent to the activities of the TSI. I appeal to the TSI members to be more proactive and become fellow members. The TSI requires more mature TSI members as executive committee.
In future Telemedicine will grow rapidly and we, the TSI, need to be very clear in what we advocate about teleconsultations. Documentation of Teleconsultations is of paramount importance. TSI needs to shift the HQs to the NCR and start a Telehealth education wing.
Please ensure positive participation in all TSI activities.
The New President Speaks
Col (Dr) AshviniGoel (Retd.) President, Telemedicine Society of India
As I done the unenviable mantle of the President of Telemedicine Society of India, I cannot help but reflect upon the year gone by. It has indeed been a year that no one will forget in a hurry. Some notable events of the past year being; the TELEMEDICON 2019 organised at Indian Spinal Injuries Centre in New Delhi with the largest gathering of very senior government functionaries in any TSI conference so far; the proclamation of Govt support for ‘Regulatory Framework for the Practice of Telemedicine in India’; the hurried and intense work on the Draft Telemedicine Practice Guidelines by a small group of dedicated and sincere TSI members with legal background at behest of the Chairman Board of Governors MCI and Member NITI Aayog; the issuance of the “Telemedicine Practice Guidelines” for RMPs on 25th March 2020 quickly followed by similar guidelines for ASU practitioners by CCIM on 7th April and for Homeopathy practitioners by CCH on 10th April 2020; the quick and successful response by a committed group of TSI members in forming the Training Team and conducting ‘Online Basic Orientation Course on Telemedicine Practice Guidelines’, training a large number of doctors (RMPs) by curating content equalling global standards, mostly working ‘pro bono’; the havoc created by Covid Pandemic; the disruption of the daily life and acceptance of the ‘New Normal’; the ‘feeling of being in doldrums’ at the realization that we may have to forego TLELEMEDICON 2020 this year; the serendipitous decision by the Immediate Past President and the undersigned to approach a State Chapter of TSI (or a group of more than one) to organise the conference on a Virtual mode; TN Chapter taking up cudgels under the capable leadership of its President and the resulting stupendous success of the TELEMEDICON 2020.
The hurried melange of activities has left an indelible impression on my mind and possibly helped to shape my thoughts for the future. I wish to take this opportunity to share my thoughts with you all. As with all such endeavours, there is a great deal of subjectivity. Many of the thoughts and ideas are offshoots of observations over the past twenty years. If we attempt most, accomplish some and others do not see the light of the day; I think we would have done our job of doing a sincere effort of getting our Society on an even keel. Getting the process started and making it a self-sustaining process is what we must ensure.
In our consolidated effort to move forward as a society, there are a few housekeeping matters which require to be streamlined. A notable few being: manpower concerns within the society; financial avenues for sustaining the capacity building programs initiated by the society; partnering with other associations, industrial bodies as a matter of public outreach exercise; review of internal milieu, organisational restructuring. In order to achieve the foregoing, I intend to realize the following:
1.Implementing agile and decisive decision making: Implementing agile and decisive decision making within the Executive Committee and beyond the closed group, to ensure no new partnering initiative or moot point is side-lined: The entire world has now woken up to the benefits of Telemedicine technology after the advent of Covid pandemic. This has resulted in all and sundry jumping onto the Telehealth bandwagon with the majority of them being hard core profit oriented business entities well entrenched in cut-throat business and “for-profit” ethos. If we at TSI, want to have a place in this eco-system, we will have to follow a process of rationality in our thought process, well-researched and well-informed decisions and most importantly agile and decisive decision making.
2.Inclusive and participative governance of TSI activities: By office bearers, and other senior members who have been spearheading the cumulative efforts of the society over the years. TSI is now almost 800 members strong, and growing day by day in strength. I feel it is far too ambitious to think that an Executive Committee of 14 members comprising of COO, Immediate Past President, President, President Elect, Vice President, Secretary, Jt.Secy& Treasurer and the seven EC members; can do justice to all the decision making required to make TSI a globally recognized think-tank and promoter for Telehealth activities, especially when we are competing with organisations like ATA, HIMMS and other similar entities in the field of digital health. Hence, to be able to fulfil our obligations we need to reach out to all our members, especially the senior members, the TSI Margdarshaks to seek their views and recommendations in a process of participative governance. A number of committees have been constituted recently to enable this, and I exhort all TSI members to take this responsibility with all seriousness and in the right spirit to help steer TSI on the path of progress of being ‘Numero Uno’ in the field. I request that more and more members seek to be involved with the various committees that have been formed for ‘governance’ of TSI matters.
3.Growth and empowerment of Regional chapters: By supporting them financially, as well as extending institutional support, as and where required, to increase outreach, and make telemedicine available to the last mile. The Regional Chapters are the functional arms of The Society. The growth and empowerment of the Regional Chapters will go a long way towards progressing the agenda of The Society. I request all TSI members to explore avenues of growth within the spheres of influence of their Chapters. I promise that as President TSI, I will extend all support for all such activities.
4.Explore reasons for lack of involvement by TSI members in TSI activities: Remove any hurdles for involvement of TSI members in TSI activities, increase participation for inclusive growth of the society and its members. See para 3 above;
5.Increase membership: Increase membership both at individual and institutional levels; “each one, get one” is a strategy which could be adopted by us all to ensure that the opportunity which has been presented this year is not lost and we attempt to gainfully utilize this ‘God given’ opportunity to maximal benefit for The Society;
6.Revision of Bylaws: Revision of Bylaws is necessitated as the present are antiquated and must be aligned with the change in the overall ethos pertaining to the field of Telehealth, growing participation of the private sector, and other industry associations as well as NGOs seeking an alignment with TSI in augmenting the vision and activities of The Society;
7.Lateral linkages: In order to grow in this rapidly progressive field of Telehealth, TSI has to strike synergistic liaisons with other NGOs and industry majors who are functioning in this field. Lateral linkages with the industry and other agencies were forthcoming in plenty, however the various MOUs could not be finalised due to internal misgivings and apprehensions of some EC members. Our intention should be to streamline the internal processes for engaging in such partnerships to the betterment of The Society and to keep the momentum going;
8.Financially sustainable activities: Financially sustainable activities for the purposes of ensuring growth and smooth functioning of the society will go a long way towards fulfilling the aims and goals of The Society.
9.Training with Certification: Training with certification will have to be promoted to ach.ieve the goal set out by the Member, NITI AAYOG and in conformity with the Telemedicine Practice Guidelines for evangelizing telemedicine and accurate adoption of the Telemedicine Practice Guidelines by the community;
10.TSI website: Website of an organisation is its face that the visitors look at for the first time while enquiring about its activities, “first impressions are lasting impressions”. TSI website must be updated continuously to reflect the activities of the society, as well as to keep the community abreast with the latest updates from around the world;
11.TSI eMagazine/Journal: TSI eMagazine/Journal has to be rolled out on a defined, periodic basis, with high quality scientific content, demonstrating the commitment of the society to the cause of telemedicine;
12.Liaison with Govt functionaries: Sustained liaison with the concerned Govt functionaries, both at Centre and State level, in furthering the regulatory and policy work in the domain and practice of telemedicine;
13.Relocation of TSI HQ: Relocation of TSI HQ to NCR to facilitate convenience in conversations with the centre;
14.Development of Telehealth Standards and benchmarking capabilities: Development of Telehealth Standards, alongside government agencies, private bodies, and other designate agencies in collaborative efforts. Also, developing bench marking capabilities for Telehealth apps and platforms, by engaging with the industry and by advising and consulting within the society, leveraging the cumulative experience of the members from different walks of professional life;
15.Restructuring TSI as a corporate body: Restructuring TSI on lines of ATA/HIMSS ( Healthcare Information and Management Systems Society), which work in close contact with the Government, private players and take pride in operating as corporate bodies.
As a way forward, I invite participation of one and all, in the smooth functioning, promotion and activities of Our Society. Stay Safe, Stay Healthy.
TELEMEDICON2020 Stats
The registration fee for delegates was a meagre token amount to get their valuable commitment to attend and enjoy the 3 days of virtual technical feast.
The registration was slow to start but gradually towards the end touched 1126
Further breakup showed that the registrations included:
TSI member Registration – 220 Doctors – 586 Students 154
We had a small participation from the industry with about a dozen sponsors who were provided with a stall in the Virtual Exhibition hall.
The scope of the conference enlarged as the dates got closer. Finally we had almost 24 hours of conference time that were spent in three concurrent sessions on day two and three, making it almost 52 hours of deliberations on Telehealth. There were 18CME’s, Symposiums and Workshops including a Hackathon.
All the sessions have been video-recorded and we hope to make it available to all the members.
Claim Credit Hours for Attendance to TELEMEDICON 2020
The doctors who attended and submitted their medical registration numbers of council would be able to claim four credit hours from the Maharashtra Medical Council. Though the time was short but this was made possible due to the efforts of Dr. B.S. Ratta, Co-Chairman of the meeting. This made TELEMEDICON 2020 truly an academic meet.
TELEMEDICON2020 – A Summary of the Event
Bagmisikha Puhan Executive Member, TSI
TELEMEDICON2020 was a new experience in this new normal. To encapsulate 52 hours of deliberations of the virtual meet would be impossible. However we would like to highlight few key takeaways from the event as this difficult year 2020 comes to close.
1.With the introduction of the legal framework, the trust in the ecosystem has been supplemented,and has fostered faith in the practitioners, patients, and the other valuable stakeholders in the ecosystem, in terms of care delivery.
2.In terms of rural health vis a vis telemedicine, reaching the last mile would require greater public-private participation; it is felt that increased interactions between the practitioner and the patients will increase the faith restored by the patients in the infrastructure. The government’s plans are laudable through its various projects to reach the last mile to deliver health to the masses using telehealth, however there are likely to be huge implementation challenges.
3.There is apprehension in the minds of the practitioners, in terms of the incumbency to comply with data privacy and protection laws.
4.Integration of the patient’s health / medical records in a centralized system would enable the practitioners to access documents from secure servers without having to concern themselves with storing the same onto their local servers and exposing themselves to additional risk.Furthermore, lack of clarity in respect of the retention timelines may lead to potential lapses on part of the data fiduciary / custodian with respect to data storage principles.
5.Training and capacity building exercises will have to be amplified, to bring the practitioners up to speed with the advanced technology, as well as the regulatory norms which they must adhere to in terms of delivery healthcare via means of information and communications technology (ICT).
6. In the face of the ongoing pandemic of Covid-19, the practicing physicians (from across several clinical specialties) have had to attend to a diverse spectrum of ailments via telemedicine consults; in doing so, they feel, the lists of medicines which are referred to within the TPG are limited and restrict the physician from managing the patient effectively / desirably. While the potential for abuse of medication/ drugs is relevant, the restrictions on drugs which can be prescribed over a telemedicine consult, undermines the very purpose of digital health, which is to widen the outreach, and serve the underserved.
7.There were deliberations with respect to the benefits of telemedicine, in reaching out to the vulnerable population in augmenting the mental health care infrastructure. The mental health practitioners have realized the benefits of telemedicine, which allows women, elderly, and home-bound citizenry to reach out to them for consultations. TPG has given the necessary fillip to the home-bound citizenry to access mental health professionals, without having to worry about their privacy, or their prowess to access such services, as and when necessary.
8.Deliberations were also made with respect to the minor/ children/ adolescent population, who are benefiting from access to mental health practitioners from across the vast geographical spectrum, without exposing themselves to the undue / unwarranted / unsupported physical visit to the practitioner/s.
9.The specialists have also witnessed a boost to their consultancy services and have been able to engage with the treating physicians, who may be situated in a poorly accessible demographic landscape (Tier-3 cities, remote areas).
10.Several practitioners have also brought to the fore, the challenge in spending a longer time in ‘raw data-entry’, especially the ones who are not conversant with the technology at hand. This leads to delay and extends the average discussion/ consultation time with the patient, adding to the already disparate physician-to-patient ratio in the country.
.11.A solution-oriented approach, leading to introduction of homogenous/ interoperable systems would be preferred.
12.Greater involvement of ancillary workers in supporting the physicians, patients, and other stakeholders in the ecosystem, is the need of the hour.
13.Practo in collaboration with TSI released a position paper, emphasizing on the gaps in the system and the overbearing positive implications of the new regulations. The paper highlights the associated statistics and the key levers in the ecosystem.
To surmise, during the conference, while the above factors were discussed, the participating delegates and faculty have expressed their gratitude to the government in enabling the ecosystem to flourish by way of the introduction and successful implementation of TPG.
The participation from dignitaries situated outside the country, brought to the fore, that as a society we have along way to go in terms of imbibing the practice of telemedicine in our daily lives. There is a pressing need to build the confidence in the patients to favor the practice and adoption of telemedicine, which is critical tosupport the lifestyle medicine practice, moving us from illness to wellness. Also, with the necessary capacity building and structured trainings, the practitioners will be able to become better aware of the telemedicine related laws and be more confident in their use of ICT in healthcare. A study presented by a French practitioner, showed that the numbers featuring the willingness to imbibe telemedicine practice have only risen since the country first introduced the legal framework over a decade ago. For India, while the geography and the demography pose challenges, there is also an invaluable opportunity presented by the onset of the pandemic, which is changing the perspective of the larger population, and reassuring faith in ICT for delivery of services.
This document only lends a very brief, high-level insight to the lengthy and engaging discussions during the conference; however, it brings to the fore the pressing needs, and the positive feedback since the release of TPG, and the continued practice of telemedicine through decades. We expect the healthcare fraternity to adopt ICT and augment their practices, as well as the patients to feel safer in interacting with their physicianstranscending physical barriers.
TELEMEDICON2020 – Free Papers and their Winners
There were 34 free papers submitted of which 27 were presented. There were thirteen podium and fourteenposters presentations.
Six Podium papers were selected as winners for best papers and will be issued certificates and cash award
These were as follows:
PODIUM WINNERS
1.Dr Sarang Patil, MUHS Nashik Tele-pulmonology a ray of hope in elderly COPD patients
2.Moaz Hamid, Western Sussex Hospital, UK Mobile Health Apps: Using the Five-Factor Model of Personality as a predictor of the preference for gamified features and their usage characteristics
3.Govinda Narke, Free Asthma Clinic Hadpsar Pune Use of telemedicine for asthma control and follow up consultation during COVID pandemic
4.Akhila Kosuru, Deputy General Manager, Apollo Tele Health Services, Hyderabad Perception of doctor for prescribing drugs in teleconsultation
5.Ms Jinchu Paul, NIMHANS, Bangalore Effectiveness of the addition of virtual NIMHANS ECHO tele-mentoring model for skilled capacity building in providing quality care in alcohol use disorders in DMHP districts
6.Dr Avinash T,, Kidwai Memorial Institute of Oncology, Bangalore Roadmap to paediatric oncology palliative care services through Telemedicine.POSTER PRESENTATION WINNERS
First
Aditi Kini, HCG Hospital Feasibility of Tele-rehabilitation of swallow and communication & Functions–
Second
Zeenat Fatima, AIIMS, Bhopal Feasibility and acceptability of Teleconsultation through video mode for diabetes at a tertiary care centre in India
Third
Vijayalakshmi Poreddi, NIMHANS Bengaluru -Nursing Interns perceptions of Telenursing Implications
TELEMEDICON2020 Feedback
TELEMEDICON2020 – ‘Picture that Said It All’
TELEMEDCION2020 was attended by at least four speakers who were suffering from active COVID19 infections. COVID infection did not deter them from participating in this virtual meet. In fact Mr. Harish Manian, CEO of MGM Healthcare, Chennai spoke from his hospital bed about the Hospital Perspective for Tele-health Insurance.
Mr. Harish Manian, CEO of MGM Healthcare, Chennai spoke from his Hospital Bed
The next issue in Jan 2021 would carry the Part- 2 of TELEMEDICON2020 and cover the highlights of the various sessions
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Design – Sankara Nethralaya Technical Partner- www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
This will be the 16th International conference of the Telemedicine Society of India. The meeting will be in a virtual web mode in keeping with the current new normal.
The TN chapter along with four other state chapters (Delhi-NCR, Rajasthan, Maharashtra and Karnataka) have taken up the responsibility to conduct TELEMEDICON 2020 from 18th to 20th Dec 2020.
Telehealth in India has grown exponentially in a very short time after the notification of the Telemedicine Practice Guidelines by the Govt. of India. In keeping with the above the theme of the conference has been aptly adopted as ‘Telehealth – From the Fringes to the Mainstream’
The conference will have 2.5 hours of morning and another 2.5 hours of evening deliberations with 4 hours of virtual exhibition and sponsored webinars in the afternoon from our potential sponsors.
Medicall – an established medical exhibition company for the last 20 years has agreed to take up the responsibility for handling our virtual exhibition.
The registration amount for the three days web-conference is very nominal.
TELEMEDICON 2020 will connect healthcare professionals, policy makers, industrialists, health insurance providers, online pharmacy chains, nurses, students, and various stakeholders from the field of Telemedicine and Health Informatics, over one common platform and bring to the fore the pain points, as well as the possible solutions, that could resolve existing issues.
Association with entities
Telemedicine Society of India invites you to participate at various levels –
Industry sponsor of the conference with its various benefits to showcase the brand and products.
Knowledge partner, whereby, an organisation can add value in terms of policy development and organise webinars keeping the above program in mind with mutual agreement.
Affiliate partner, whereby, the partnership adds value in terms of providing services such as hosting of the conference on a platform, hosting the website, creating design, sending mailers, helping with sponsorship or any other way to help the conference. TSI will share the logo and acknowledge such partnerships.
Planned Themes
1. Transforming Telehealth Training for Registered Medical Practitioners in India
a. Format of Training b. Current Experience with Training c. Virtual and augmented reality d. The way forward
2. Legal & Ethical Aspects – The Grey Areas
a. TPG – what needs to be changed? b. Data Protection Act and Health c. Good Practices – learnings from abroad
3. Challenges in Health Data Integration – National and State
4. 5G and Telehealth – the Larger Impact
5. AI, Block chain and Telehealth
6. Wearables and impact on Tele-health
7. Remote Monitoring – How to cut costs and Improving Patient care
8. History of Telemedicine
a. India b. International
9. Standards
10. Health Apps in India
11. COVID-19 and impetus to Telehealth
12. Wellness & Telehealth
13. STEMI project in Cardiology
14. ECHO global project
15. Health Insurance and Telehealth
16. Online pharmacies – Getting it Right for Telehealth in India
17. How can Rural Health care be Transformed Using Telemedicine?
18. Planned Workshops & Parallel Tracks
a. How to set up a Telehealth consultation Platform – DIY b. Taking care of Security issues in Telehealth c. Setting up Payment Gateway d. Standards – software and Hardware e. Teleopthalmology – Joint meeting with WHO group & ITU f. International Telehealth Societies – working together and sharing of good practice documents g. Tele- health Initiatives by central & State Govt in India – Examples of Excellence
Dr. Sunil Shroff Organizing Secretary President, TN – Telemedicine Society of India
Telemedicine pRoject for screENing Diabetes and its complications in rural Tamil Nadu (TREND) project
Dr. V. MOHAN, MD,FRCP, Ph.D, D.Sc, FNA,FACE, FTWAS, MACP, FRCE Chairman, Dr. Mohan’s Diabetes Specialities Centre and President, Madras Diabetes Research Foundation, Chennai.
Awareness, diagnosis, regular checkups and other ways of preventing as well as treating NCDs especially diabetes, are very low among the rural sector. Hence, to study the status of diabetes and associated complications in rural Tamil Nadu, the Madras Diabetes Research Foundation (MDRF), Chennai and the University of Dundee, UK have taken up a joint research collaboration to screen 15,000 people in 25 shortlisted villages in Kancheepuram and Chengalpet districts of Tamil Nadu. The program called as the TREND (Telemedicine pRoject for screENing Diabetes and its complications in rural Tamil Nadu) project focuses on finding the burden due to diabetes and its complications in rural Tamil Nadu and providing novel solutions for its management. This project is funded by the National Institute for Health Research (NIHR) of the Department of Health, UK to take up the INdia-Scotland PartnershIp for pRecision mEdicine in Diabetes (INSPIRED) project. The TREND project is part of the overall INSPIRED program. Through the TREND project, we aim to address the challenges with innovative use of technology that will enable even remote areas gain access to quality medical diagnosis and care.
Early and timely screening for diabetes and pre-diabetes, prevalence of hypertension and obesity, screening diabetic complications in eye using retinal images, foot and kidney as well as assessing diabetes control among individuals etc. are being carried out through this project. We are utilizing telemedicine technology in the chosen villages to screen for diabetes related complications. A fully equipped mobile telemedicine van fitted with all equipment necessary for screening for diabetes and its complications has been set up. The infrastructure in the telemedicine van includes an inexpensive mydriatic Remidio “fundus on Phone” apparatus, computerized electrocardiography (ECG), Doppler and biothesiometry. The telemedicine van also includes facilities for blood sampling. So far, nearly 10,000 individuals aged =18 years have been screened for diabetes and other metabolic NCDs.
Tele Counselling Solutions From Sankara Nethralaya S. Chandra Mouli
Chief Information & Technology Officer,
Sankara Nethralaya, Chennai.
INDIAN TELE HEALTH MARKET TRENDS : MARCH – JUL 2020
50 MILLION INDIANS ACCESSED HEALTHCARE ONLINE
700% GROWTH IN TELE OPHTHALMOLOGY
80% EXPERIENCED IT FIRST TIME
44% WERE FROM NON-METRO CITIES
67% DROP IN PERSON DOCTOR VISITS
The pandemic outbreak was a perfect storm warranting fast tracking innovation in health tech.and its adoption at a rapid pace never thought of before with the providers and its participants.
Sankara Nethralaya being a pioneer in the country in adoption of Technology through its adoption of specialty EMR and Hospital Management systems fast tracked its adoption of its Innovative Tele counselling solutions to its Patients as its COVID response. Social distancing, concerns on Hygiene warranted disruption to the OPD at large and forced Medical fraternity to adopt newer ways to engage with Patients and also provide services on demand.
In view of the early lock down SN realized that it needs to reach out to all its patients who were operated upon and provide counselling. We realized the need for an autonomous, smart and self aware system that
Need to manage appointments for the patients with their respective doctors with whom they consulted
Provide the doctors with relevant clinical information for decision making
Capture Action plan and update the EMR
Provides a frictionless compute & highly automated with the least manual intervention in view of remote working and servicing.
Solution & approaches
Key objectives – Provide patient delight and actionable insight to Consultants through smart solutions.
Key design principles
Zero UI concept – Familiar Email interface, smart texts leveraging SMS, proven APPS for patient engagement, Web based solutions and Voice based services
Simplicity in design
Focus on superior user experience
Development approaches
Agile / Extreme programing
Remote working & usage of collaborative tools & technologies
Working code as a measure of progress
Incremental build – over 90+ enhancements and feedback were factored as changes
Secure coding practices IT Infra, Cyber security & Cloud
Leveraging existing highly resilient data center
Multi cloud and best in class on demand services like voice telephony, messaging and email
Disaster recovery on private cloud
Secure infrastructure and continuous monitoring for performance
Monitoring for any cyber attacks and ensuring high availability
Leveraging IT Help desk for proactive support
Technology used
Microsoft based Techstack
MS SQL2016
.net 4.5 framework
Cloud telephony & voice basedservices
MESSAGINGServices
Emailintegration
Secure hostedsolutions
API based integration into coreservices
Analytics
Outcome
Over 10,000 SN patients were provided tele counselling services leveraging the platform since April 2020. 98%ofthepatientswereextremelysatisfiedandprovidedravingfeedbackonthequalityofservices. Dissatisfied patients or negative or feedback were followed up and continuous enhancement to servicesmade.
Lessonslearnt
Keep communicating Every resource isimportant Distribute work and manage stress & also risk Progress is important. Working code is the best test of success. Manage surprises & have a plan B for every contingency Leverage proven tools Incremental innovation – no big bang approaches. Continuous feedback and go the extra mile to provide patient and user delight Train and educate users and reduce adoption risks.
Transmission of ECG over Telephone Lines – 1905 (History and Evolution of Telemedicine – 3rd Milestone)
Dr. Sunil Shroff, MS, FRCS, Dip. Urol (Lond.) President, Tamil Nadu Telemedicine Society of India,Editor, www.medindia.net, Consultant Urologist & Transplant Surgeon, Madras Medical Mission Hospital, Chennai, India (shroffmed@gmail.com).
On March 22nd 1905 Willem Einthoven, a Dutch professor of physiology recoded the first tele-cardiogram. He utilized a telephone cable to transmit the signal from the hospital to his laboratory 1.5 km to record the ECG. He was the first to introduce the Latin term ‘tele’ as a prefix to indicate remote delivery of medical service. The term he used for this was “telecardiogramme.” The original ECG Machine weighed 270 kilograms required five people to operate and the patient had to immerse their legs and hand in saline water. It also required cooling for the powerful electromagnets.
Einthoven graduated in medicine from the University of Utrecht and served as professor of physiology at the University of Leiden from 1886 until his death. It was in 1903 he first invented a galvanometer that was used to measure the changes of electrical potential caused by contractions of the heart muscle and to record them graphically and he coined the term electrocardiogram for this process. Apparently his hospital did not allow him to use the ECG machine in its premises and he hence transmitted the ECG over the telephone line and recorded it in his lab. He received Nobel Prize for this important invention of ECG in 1924.
In current age of so many technical advances with so many tools to evaluate and treat the heart we can still refer to Einthoven’s remarks in 1920s when he said – “An instrument takes its true value not so much from the work it might possibly do but from the work it really does” and “Truth is all that matters, what you or I may think is inconsequential.”
Artificial Intelligence Smartphone Tool Could Diagnose Strokes Within Minutes Novel tool can diagnose stroke with the accuracy of an emergency room clinician from interaction with a smartphone, reports a new study. The tool can diagnose a stroke based on abnormalities in a patient’s speech ability and facial muscular movements within minutes from an interaction with a smartphone….. Read More
Novel Wearable Sensor Help ALS Patients Communicate New wearable sensor was developed by MIT researchers to help those living with amyotrophic lateral sclerosis (ALS) communicate. The findings of the study are published in the journal Nature Biomedical Engineering. ….. Read More
Virtual Reality Helps Patients Address Eating Disorders Virtual Reality (VR) technology can significantly impact the validity of remote health appointments for those with eating disorders. Through a process known as Virtual Reality Exposure Therapy (VRET) ….. Read More
Novel Chili-shaped Device may Reveal Just How Hot That Pepper is Novel chili pepper-shaped device containing a paper-based electrochemical sensor can be connected to a smartphone to know how much capsaicin is in hot pepper, reports a new study. The findings of the study are published in the journal ACS Applied Nano Materials.….. Read More
International
Abboud Chaballout Is Using AI to Revolutionize the Healthcare System Abboud is an entrepreneur and thought leader in the field of health and medicine. He earned his law degree from the University of California Berkeley School of Law, one of the most prestigious institutions and one of the top ten universities for law studies….. Read More
United Airlines Rolls Out Digital Health Passport (CBS DETROIT) – United Airlines is testing out digital health passports. The digital health dossier houses Covid-19 tests results for passengers. Travelers can take coronavirus tests up to 72 hours pre-flight and then input their results on what’s called the common-pass app.. Read More
India & EU explore possibilities of enhanced cooperation In a statement, the MEA said that leaders explored the possibilities which can help to strengthen India-EU strategic partnership in the post-COVID-19 world. In the meeting, decisions which were taken at the 15th India-EU Summit held in July 2020 were also reviewed….. Read More
Scientists Develop First Smartphone App That can Detect Ear Infections in Children University of Washington researchers have created a new smartphone app that can detect ear infections in children. The app detects fluid behind the eardrum by simply using a piece of paper and a smartphone’s microphone and speaker..….. Read More
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Design – Sankara Nethralaya Technical Partner- www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Vision Centres
Dr. Kim Ramasamy Aravind Eye Hospitals, Madurai
With over a billion people living with blindness or visual impairment due to preventable or treatable conditions, universal coverage for eye care is still a largely unmet need. This is especially because those who need care are in remote and rural locations where service delivery is a challenge.
Primary eye care remains a challenge especially because it has been difficult to provide comprehensive care for all the conditions encountered at the primary level. However, with the arrival of broadband internet, this has become a possibility. Vision Centres or primary eye care centres now provide comprehensive and complete eye care to the rural population.
Most notably, Aravind Eye Hospitals and LV Prasad Eye Institute in India have a large network of rural vision centres. This model is now being rapidly replicated by national and state governments.
Comprehensive care:Patients who visit the vision centre receive a comprehensive eye examination by an allied ophthalmic personnel or vision technician. The technician captures the findings in a cloud-basedelectronic medical record – including any images of the eye. These records are accessed by an ophthalmologist at a secondary or tertiary eye care facility. The patient is able to have a teleconsultation immediately with the ophthalmologist, who gives the final treatment advice and prescription. The technician prints out the prescription and gives it to the patient along with counselling about the treatment.
Complete care:It is important that patients are able to act upon the doctors advice. So as to complete the loop,it is important that affordable spectacles and ocular drugs are made available at the vision centres itself for the patients. If the patient needs to be referred for higher levels of care, clear instructions and counselling needs to be given to ensure that patients act upon the referral.
Coverage:Each vision centre serves a rural population of 70,000-100,000. An estimated 30% of this population would need some form of eye care. Evidence shows that over four years 82% of those in need have been seen at the vision centres! This coverage is not only true at the level of gross patient numbers – but also for individual eye conditions too.
Vision centres, being closer to the community have a unique advantage to ensure treatment of chronic conditions are truly effective. Given that they are local to the patient, they are more accessible for regular follow up visits and can ensure patients stay on-track for their treatment. Aravind Eye Hospitals have ensured that patients with chronic conditions can procure medication and a patient registry helps to longitudinally monitor these patients over time.
The model has been successfully replicated and scaled up by other governments and NGOs in different parts of the Indian Subcontinent:
Aravind assisted the state government of Tripura to set up 40 vision centres across the hilly state of Tripura where access to health care is a major issue.
Aravind is also working with other state governments in India to replicate this model: so far, 10 centres have been set up in Chhattisgarh and 32 in Tamil Nadu, as pilot initiatives.
Aravind has helped the Government of Bangladesh set up 50 vision centres, with another 40 in the immediate pipeline. The commitment is to set up a total of 400 vision centres across the country.
A senior ophthalmologist at the State Blindness Control Society of Tripura observes how the tertiary government hospital at the capital city used to receive several patients with minor eye ailments. This not only meant that critical resources of the hospital were being used for minor treatment but also meant a great financial burden on the patients who travelled so far. But now, a much larger number of such patients are seen locally at the vision centres and only those with more complex eye conditions show up at the tertiary facility.
What does it take to set up a successful vision centre network?
Patient centric workflows
Comprehensive eye examination
One-stop services (eyeglasses, ocular drugs etc. should be made available)
Staff trained to provide high quality, patient centric care
Telemedicine consultation
Affiliation with a referral hospital
Strong monitoring system to ensure quality of care (patient feedback surveys)
Staff engagement, motivation and continuous education
Tele-ICU: Distance is not a real barrier for Critical Care
Dr. N. Ramakrishnan AB (Int Med), AB (Crit Care), AB (Sleep Med), AB (Obesity Med), MMM, FACP, FCCP, FCCM, FAASM, FISDA, FICCM Founder & Managing Director, Chennai Critical Care Consultants & TACT Academy for Clinical Training Director, Nithra Institute of Sleep Sciences
What is TeleICU?
Tele-ICU or Tele-Critical Care is a customized solution for hospitals using technology to bridge experienced Critical Care Specialists (Intensivists) and nurses to monitor and support care for patients in the Intensive Care Unit (ICU). The Intensivists and nurses operate from a centralized monitoring center
What are the various models of care?
Remote monitoring is referred as ‘continuous’ when care is provided proactively round the clock usually from a centralized monitoring center (often referred to as ‘Command Center”).
Alternatively, ‘episodic’ care could be provided reactively ‘on-demand’ when the ICUs requiring support could request services as needed. With increasing use of smartphones and tablets, this model has been facilitated by specialized Tele-ICU applications (apps).
Tele-ICU rounds have been helpful in assisting ICUs. In this model the Intensivists remotely connects with the Doctor at the user end and is available to facilitate and discuss about patients and assist with care plans. Focused rounds for Nutrition support, implementing antibiotic stewardship are also an option with this model
What are the advantages?
It is currently not feasible to staff every ICU with qualified Intensivists as they are far and few and mostly concentrated in tertiary care centers in larger cities. Tele-Critical care helps to reach specialized services anywhere, anytime.
Remote monitoring services have consistently shown to improve implementation of evidence based best practices
Monitoring by specialists has shown to improve outcome such as reduction of length of stay, implementing care bundles and reducing infections and also reducing mortality rate.
Hospitals have noticed that there is an increased retention of patients who would have otherwise been transferred out.
ICU care is complex – How can it be provided remotely?
Critical care involves several interventions by a multidisciplinary team. Most of these are ‘cognitive’ while some involve bedside procedures.
It is important to understand that the remote ICU model complements and does not replace the bedside team. The input from the bedside team is crucial for the remote Intensivist to provide input.
Specialist team of Intensivists, Physician assistants, Respiratory Therapists, Critical Care Nurses, Clinical Nutritionist & Pharmacist can remotely offer several cognitive inputs that could greatly benefit patient care. They need to closely interact with the bedside team to implement these decisions and also for any procedures that may be required.
Are TeleICU services available in India?
Chennai has been a leader in healthcare in our country and has several firsts to its credit. The first TeleICU anywhere outside the USA was a collaborative effort by Chennai Critical Care Services. We partnered with Advanced ICU Care, USA and started providing Tele-ICU for hospitals in America from 2010.
The fact that the first successful remote monitoring services in India were for ICUs in USA clearly confirms that distance is not the real barrier. We continue to provide these services successfully for over 10 years now.
Proactive continuous monitoring services in India were provided by us (InTeleICU™) and providers including Critinext. With the new telehealth policy of Ministry of Health, there is a scope for modified services particularly in a reactive episodic model to extend the outreach of specialized services.
We refer the readers to our recent article calling for an urgent action on Tele-ICU services published in Indian Journal of Critical Care Medicine cited below:
Ramakrishnan N, Vijayaraghavan BKT, Venkataraman R. Breaking Barriers to Reach Farther: A Call for Urgent Action on Tele-ICU Services. Indian J Crit Care Med 2020;24(6): 393–397.
Blockchain Use and Opportunity in Healthcare
Tory Cenaj, Founder, Partners in Digital Health, Publisher, BHTY
According to a 2018 a SERMO survey, physicians across all specialties lack awareness for blockchain technology impacting healthcare providers and payers at institutions and clinical settings around the US.
47% of physicians polled have not heard of blockchain
25% indicated blockchain is ready to enter healthcare
28% reported blockchain was not ready to enter healthcare
In 2020, an American Medical Association (AMA) Survey reported:
Physicians weighed in on emerging technologies such as blockchain and augmented intelligence (AI), which is often called artificial intelligence. While 46% of physicians are familiar with the blockchain technology, 0% are using it.
Before we explore the potential applications for blockchain, let’s first provide a top line definition for it. Blockchain is a shared distributed digital ledger technology (network platform), that securely facilitates interoperable data management and provides any original source of ownership, that can potentially transform healthcare. The technology is currently utilized in pilots and scaled ecosystems in healthcare around the wordto optimize business processes, lower costs, improve patient outcomes and enable better use of data interoperability.
Unlike traditional centralized databases, data on a blockchain can be distributed across multiple databases and computers (also known as ‘nodes’) so that everyone has the same version(or “ledger) of a process or transaction. ‘Blocks’ of data are linked together by a hash (a digital signature of random letters and numbers) that form a ‘chain’ of data containing a complete history of the performed transaction that cannot be changed – only added to, so it is considered “tamper resistant.” Data is secured through cryptography (advanced encryption) for participants can trust the ‘blocks’ of data posted are authenticated and verifiable. These features result in decentralized data systems that are not controlled by a central authority that are usually vulnerable to breaches or points for failure. Blocks represent a single source of information all participants agree to as true, resulting in higher levels of trust by participants.
Applications and Studies
Blockchains offer the option to be permissioned/private or consortium networks, not open to the public but used by a group of participants to limit the participation and access to shared data, or they can be public blockchains.
The technology as an appropriate network sharing platform electronic health records to reduce errors and increase interoperability while preserving data privacy. It also enables analysis and payments for claims or contracts between provider, health system(s) and patients. Most physicians aren’t aware of the efficient, error free utilization the technology provides – particularly since the onset of the Covid-19 pandemic has highlighted deficiencies in the marketplace. To learn more, view articles below:
Blockchain technology can significantly reduce the cost and speed of clinical trials. This includes a shared data ledger, security of data, patient recruitment and retention, interoperability between all devices used, efficient and validated clinical and patient data management and analysis, increased data integrity, and payment portals – all while reducing human error and increasing security. See the article below for more details.
Pharmaceutical supplies also include multidisciplinary stakeholders including manufacturers, wholesalers, packagers, logistics, regulators, hospitals, pharmacies and patients across countries creating a global ecosystem.Consider drug fraud, mismanagement, quality and safety. Blockchain resolves many supply chain challenges and provides cost efficiencies and faster turnaround. Tracking and tracing becomes seamless in a modernized system. Consider the publications below describing methodologies and pilots in more detail. We already find blockchain utilized in other industries.
Many breakthrough articles have been published in Blockchain in Healthcare Today (BHTY), the world’s first open access peer reviewed journal that amplifies and disseminates distributed ledger technology research and innovations in the healthcare sector. We encourage authors to submit manuscripts and join the ecosystem. The journal is published on a continuous basis with a world-class peer-review board and registers original research article provenance on the blockchain. The journal is indexed in Science Open, Unpaywall, Google Scholar and the PKP Indexes.
The journal hosts the annual ConVerg2Xelerate (ConV2X) conference. Registration is open for the November 10 and 11 symposium with the theme “US -World Health Transformation.” Attendance is free. For more information click here.
India leads the world in Telehealth Cross-Sector Partnerships
Dr. William B. Eimicke is Professor of Practice and Director of the Picker Center for Executive Education at the School of International and Public Affairs at Columbia University. He retired from the FDNY as Deputy Commissioner for Strategic Planning and Performance Management and served as New York State Housing “czar” under Governor Mario M. Cuomo. He is also the co-author of Management Fundamentals (2020) and Social Value Investing (2018), both published by Columbia University Press
Adam Stepan is the Director of the Picker Center Digital Education Group, and Adjunct Professor at the Picker Center. Adam oversees creation of online class materials and audiovisual case studies for the global EMPA program and works with SIPA faculty on the research and creation of audiovisual case studies.
In 2014, my colleague Adam Stepan and I began a project to develop original video and written case studies for a new hybrid MPA at the School of International and Public Affairs (SIPA) at Columbia University. We focused on innovations in providing essential public services such as police, fire, education, sustainable agriculture and health care. After considerable research, our innovation in health care focused on telemedicine and electronic record-sharing identified India as being at the cutting edge of that innovation.
Our team then made several trips to India to meet with Dr. K. Ganapathy, film what was going on at Apollo Hospitals, look at the history of telemedicine and its future and then make what is now a widely used case film and written case study ( https://vimeo.com/200378894 ), comparing India to less advanced efforts in the United States and Brazil. The case study was presented and discussed at a major conference here at SIPA, appropriately simulcast to other experts across the global.
As we continued our research, we observed a series of emerging public-private partnershipsin India. By 2018, another colleague, Howard W. Buffett and I published what is now a very well-known book—Social Value Investing (https://www.sipa.columbia.edu/svi) which features an array of cross-sector partnerships called Digital India that developed from the earlier foundation by a wide array of public and community partners.This this spring and summer, telemedicine emerged as one of the most effective tools in fighting the COVID-19 virus in the United States and now in India and other countries across the world.
For example, in New York City telehealth insurance claims have accounted for approximately 13% of patient activity compared to 0.15% only a year earlier, according to one monitoring organization. Another survey in April found 50% of responding patients said they were using telemedicine, many for the first time. Among doctors, 85% reported using telemedicine, compared to 25% at the end of 2019. A major heath care service provider, New York-Presbyterian reported that its telemedicine service use during the pandemic reached 70,000 cases per month and is continuing to rise steadily.
In India, Modi government sees Common Service Centres as a cornerstone of Digital India, as they provide access points to every corner of India to the increasing number of services and assistance the government hopes will create a much more inclusive society that will improve the quality of life for India’s very large population of poor families and individuals. Many organizations seethe program as an opportunity to do good while simultaneously attracting new customers and perfecting a new way of delivering medical services.
While the potential is great, this initiative is complex and expensive with a relatively high risk of failure. Indian telemedicine continues to face ongoing technical challenges: unreliable electrical supply, inadequate Internet bandwidth, video distortions, and software malfunctions. Even so telemedicine examinations provide reliable diagnoses for 80 percent of patients. Telemedicine examinations are generally videotaped (with permission of the patient), providing the physician with an opportunity to review, or “see” the patient again several times, to make sure the initial diagnosis was correct and that no important information was missed.
In the United States, major providers face challenges as well such as getting thousands of physicians, behavioral health specialists and office staff onto a telehealth platform and training them on how to use it. Also, many low-income patients had insufficient data plans and/or limited internet-connected devices. In some cases, this requires a regular phone call rather than a video chat. From a reimbursement perspective, health care providers are working to figure out how to incentivize the use of telehealth services while still covering their operating costs overall.
These partnerships of public and private organizations are providing potentially world-class health care for patients in urban and rural areas and even serving those with little or no income. Telehealth creates the opportunity to attract new patients, more easily offering virtual second opinions, more effectively treating addictions, improving management of chronic conditions and enhancing the lifestyle choices for doctors. In this COVID-19 pandemic, the telemedicine model developed in India helped hospitals in the United States and many other countries manage the burden on hospital emergency rooms, diagnosis and provide medicine to vulnerable patients unable or unwilling to leave their homes and ultimately help control the spread of the virus. Through the effort and expertise and hard, sustained work by several groups starting two decades ago,thousands of dedicated doctors, nurses and health care workers in India and the Indian government and its civil servants are now leading the way to a more affordable and accessible health care system for all.
Telephone call for Tele-Consultation (History and Evolution of Telemedicine – 2nd Milestone )
Dr.Sunil Shroff, MS, FRCS, Dip. Urol (Lond.)
President, Tamil Nadu Telemedicine Society of India, Editor, www.medindia.net, Consultant Urologist & Transplant Surgeon, Madras Medical Mission Hospital, Chennai, India (shroffmed@gmail.com)
For doctors ‘Tele-consultations’ is nothing new. It started soon after the telephone was invented by Alexander Bell in 1876.Little do people know that the first call that Mr. Bell made was for medical help or for an emergency of sorts. Mr. Bell called his assistant Thomas Watson and said:
“Mr. Watson, come here, I want you.”
What had happened was that the sulphuric acid from the wet battery which was powering the telephone transmitter had spilled on clothes of Bell. And after the very first conversation on the telephone for medical help, Watson quickly appeared to administer the first aid.This first call on the telephone for medical help from Mr.Bell, was almost prophetic and 140 later, the mobile phones are now being considered to be the preferred device that will help provide universal and affordable healthcare to the people of the world.
Just two years after the invention of the telephone two letters to the editor appeared in the famous medical journalLancet on 9 February1878, The first, from “A.B.M.” of Hornsey suggesting that the telephone could improve medical diagnosis and that it might be specially useful in “demonstrating and studying the sound produced by a muscleduring contact, the negative contraction, etc.” This way of listening-auscultation in medical terminology-could be done, according to A.B.M., by applying the electrodes (presumably of the telephone transmitter) directly to the muscle.
And on Nov’1879 another piece in Lancet spoke of Practice by telephone and its use that could bring down the visits to doctors clinics in the future.The commonest consultation on the telephone over the years perhaps has been – ‘Doctor I have a headache, what can I do.’
Next issue: Read about Willem Einthoven and how ECG was transmitted over telephone lines.
Telemedicine – News from India & Abroad
India
Apple Watch Saves Man’s Life
In India, the electrocardiogram (ECG) feature on Apple Watch has saved the life of a 61-year-old Indore resident. Apple CEO Tim Cook wished him fast recovery post-surgery.R. Rajhans, a retired pharma professional who uses an Apple Watch Series 5 …Read More
Younger and female doctors adopted telemedicine more during Covid in India, study says
More of the younger and female doctors adopted telemedicine or online consultations as a practice in India compared to male and older doctors in the June-July period this year, reveals a new study.A joint study by India-based healthcare research organisation Strategic Marketing Solutions & Research Centre (SMSRC) l…… Read More
India’s Telemedicine Service Completes 5 Lakh Consultations
eSanjeevani, India’s new telemedicine platform, has recorded five lakh teleconsultations. The last one lakh consultations were completed in a record time of 17 days.As a digital modality of healthcare services delivery ….. Read More
Telehealth Trains Parents to Improve Behavior Skills of Autism Kids
during the coronavirus pandemic or in other instances when in-person instruction is not possible, according to a Rutgers researcher.The study, which was published in The Journal of Applied Behavioral Analysis, broadens the treatment options for parents of children with autism who lack access to in-person training as they do now …. Read More
Demand for Telemedicine to Rise Post Covid-19: Survey
A survey on growth in telemedicine consultation in India since Covid shows that digital adoption of medicinal services grew three times during this period. According to the survey, conducted by DrOnA Health in collaboration with Mankind Pharma, 60% of respondents reported high satisfaction with telemedicine consultation…. Read More
DIVOC Health Set To Launch 20 New Telemedicine Laboratories In India By 2021.
India, October 2020: With a mission to create the most advanced digital diagnostic laboratory network enabling the connected world and to provide telemedicine and instant care, DIVOC Health launched its first, one-of-a-kind, technologically advanced DIVOC Laboratories in New Delhi in August 2020… Read More
International
New Tool Allows Easy, Effective Disease Tracking
New study used the novel IDseq tool to confirm and sequence the whole genome of the country’s first case of COVID-19. The findings of the study are published in the journal GigaScience.This tool can distinguish pathogens before there is an available complete genome sequence…Read More
Telehealth Services: A Post COVID-19 Reality? The regular use of telehealth services for cancer patients was found to have long-lasting and unforeseen effects on the provision and quality of care, said an article published in JAMA Oncology, Trevor Royce, MD, MS, MPH, an assistant professor of radiation oncology at the University of North Carolina Lineberger Comprehensive Cancer Center and UNC School of Medicine. Read More
Morneau Shepell launches unified telemedicine solution to enhance Canadians’ total wellbeing
Morneau Shepell, Canada’s largest provider of wellbeing and mental health solutions, has expanded into the rapidly growing telemedicine market to provide the employees of Canadian clients and their families with easier, more convenient access to digital health care services. . … Read More
StudyKIK Introduces Remote eConsent Technology Solution with Integrated Telemedicine Video Calling for Clinical Trials
StudyKIK, a full service patient recruitment & retention technology company headquartered in Irvine, CA announced today the release of their fully remote eConsent platform with Telemedicine Video Calling technology. Now, any sponsor who has provided their enrolling sites access to StudyKIK’s…… Read More
Health Recovery Solutions Announces Lineup of Telehealth Experts for October Vision to Virtual Conference
Health Recovery Solutions (HRS), a national provider of Telehealth and Remote Patient Monitoring (RPM) solutions, is excited to announce its incredible lineup of speakers for the upcoming Vision to Virtual conference. From October 15 to October 16, HRS will welcome telehealth experts from across the healthcare industry including those from health systems,… Read More
The “Global Next-Generation Surgical Robotics Market: Analysis and Forecast, 2020-2030” report has been added to ResearchAndMarkets.com’s offering.
The market size of next-generation surgical robotics was valued at $10.9 million in 2019. The global next-generation surgical robotics market is expected to grow at a robust rate. It is anticipated to reach $884.5 million in 2030 with a CAGR of 44.6% during the forecast period 2020-2030…Read More
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Design – Sankara Nethralaya Technical Partner- www.medindia.net
Official Newsletter of Tamil Nadu Chapter of Telemedicine Society of India
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Message from Maj Gen (Retd.) A K Singh, President, TSI
It gives me great pleasure and satisfaction that the Tamil Nadu Chapter of Telemedicine Society of India’s first Newsletter is being launched. Last three months have been very busy and productive. The training team led by Dr Sunil Shroff has done a commendable job of providing par excellent training to over 3500+ doctors. The Armed Forces Medical Services led by Lt Gen Madhuri Kanitkar had two sessions, in one the DGAFMS attended. That was the crowning glory of the TSI. The volunteering effort of the editorial team headed by Dr Shiela John is worth appreciating.
A short piece by our executive committee member Ms. Bagamishika Puhan about these training program also is enclosed.
I thank all members of the TSI in contributing to the growth of Telemedicine. The margadarshaks ( Past Presidents) have been a guiding force.
Jai Hind.
Maj Gen (Retd.) A K Singh President, TSI
Telemedicine in India: Personal Reminiscences from 1996
K. Ganapathy M.Ch (Neurosurgery) FACS FICS FAMS Ph.D is a Past President of the Telemedicine Society of India, Former Secretary & Past President Neurological Society of India, Past President, Indian Society for Stereotactic & Functional Neurosurgery, Formerly Adjunct Professor IIT Madras & Anna University, Madras & Emeritus Professor Tamilnadu Dr MGR Medical University. He is on the Board of Directors of Apollo Telemedicine Networking Foundation & Apollo Tele Health Services.
“Excellence is not a destination – it is a never ending journey”
The beginnings
It all started on the night of Sep 16 1996, I had just finished delivering an institute lecture an IIT Kanpur. Just after the Q&A ended at 09:00PM, Prof. Srivathsan, HOD of Electrical Engineering Department insisted I have dinner with him. He introduced me to the word “Telemedicine” and persuaded me to prepare a project report from 11:00PM – 04:00AM. Then commenced a love affair, which over the next 24 years has taken its toll. My legally wedded wife is often relegated to No. 3. Initially, I was wedded to Neurosurgery and now it is Telehealth. Looking back the journey has always been exciting. Arduous, often frustrating,sniggers were common, comments included “Telemedicine Ha ha ha”- but that was the 20th century. In 1998, I even had the audacity to request the association of Rural Surgeons of India to embrace Telemedicine ( Fig 1). .Having started the first Stereotactic Radiosurgery unit in South Asia and as Secretary of the then 2200 strong Neurological Society of India, conventional wisdom dictated that I should continue to focus my skills and energy completely, on what I was trained for, namely neurosurgery .However deep down was a nagging feeling , “Was there not something else, which I could do, which could help more than a few thousand neurosurgical patients ” and then the story began . I took the road less travelled by and the rest – as they say is history !! In fact I embarked on making Geography History ! and distance meaningless.
The Aragonda Story On March 24th 2000 Bill Clinton formally commissioned the world’s first VSAT enabled village hospital at Aragonda in Andhra Pradesh . In the first 2 years two hundred fifty echocardiograms were done there, telementored from Chennai by Dr Premshekar a pediatric cardiologist. Unfortunately we were all so inundated with clinical work that no papers were published, in what may have been a first of its kind initiative even globally. Every Tuesday morning, a tele–grand round took place with super specialists from the Department of Pediatrics at Apollo Hospitals, Chennai interacting with doctors in the village hospital.More than 200 tele grand rounds took place up to 2005. When Dr Vilvanathan Pediatrician who worked in this village hospital left it was not continued. Again this herculean effort was never documented.
Formation of ATNF In 2001 Apollo Telemedicine Networking Foundation was formally established as a not for profit Section 25 company . Taking modern healthcare to remote areas using technology was the mission of ATNF . In between my neurosurgical commitments I spent time and effort to help a skeleton staff of four full time employees to achieve , what in 2001 appeared preposterous – remote consultation !! Every opportunity to put a then hardly existent Indian telemedicine on the world map was utilised. I took part in the first intercontinental live multipoint telemedicine symposium on June 19 2001. Bill Gates was also a speaker .Though today it looks juvenile, it was thrilling to talk to people across the globe from Chennai. I could not resist starting with “ Good morning, good afternoon, good evening and good night ladies and gentlemen!!” Then started teleconferences with, Japan, USA, Saudi Arabia, Hong Kong. 19 years ago for a hospital to embark on video conferencing to conduct clinical meetings was certainly not the norm. Over the next 20years more than 230 regional, national, and international videoconferences in different medical specialties have taken place.
2002
Feb 15 2002 was a red-letter day for the growth of Telemedicine in India. The tension which India went through when Chandraayan 2 was to land on the moon , was experienced by me and my team when we enabled the first VSAT teleconsultation to be witnessed by the Chairman of ISRO. ISRO has publicly acknowledged that their foray into Telemedicine was influenced by that demonstration. Such was my enthusiasm then, that the Vice Chancellor of Anna University even agreed to let me address principals of 600 engineering colleges of Tamilnadu to start telemedicine units. Needless to say only four responded and that too for a short time.Telemedicine for Armed Forces -It has been my privilege to have persuaded the Indian Army to set up telemedicine units in the southern and central commands as early as 2002 with the assistance of Lt Gen Anoop Jamwal who retired as Adjutant General. Unfortunately we were too far ahead of the time and the commissioned Telemedicine units became non functional . In 2017 Telemedicine in the Armed Forces was rte established.
2003
The first formal University accredited 4 week certificate course on Telehealth technology was started with Anna University. Over the next 3 years 150 candidates in 6 batches were trained. Unfortunately due to lack of employment opportunities the course was discontinued. At about this time the Ministry of External Affairs Govt of India produced a documentary India 2.0 where Apollo telemedicine was featured.Franchised Remote Telehealth Centres gradually increased in Tier II and Tier III cities mainly in North Eastern India . Port Blair, Andaman Islands and various other remote places followed. We had almost 30 centres then
2004-05
IIT Madras started working on telemedicine enabled indigenous peripheral medical devices, designed to transmit temperature, pulse rate, blood pressure, oxygen saturation, heart and lung sounds and a 12 lead ECG .We went to the villages, used kitchens in houses, got a 100 volunteers together and transmitted this clinical data to Apollo Main Hospital Chennai for doctors to evaluate. Several such testings and clinical feedbacks led to the birth of Remedi the first indigenous stand alone Telemedicine “ Black Box” . Due to a sickness at home I was unable to attend an international Critical Care Congress. Adversity was turned into Opportunity. I gave the talk from an ICU bedside . This had a great impact. Years later I had just landed in Chandigarh for the TSI annual conference. I was informed that my grand daughter was critical and admitted in the ICU at Bengaluru. I took the return flight. The next day I gave my scheduled talk on a mobile phone from the ICU. My younger colleague Aditi did a great job projecting the slides perfectly. This unscheduled virtual talk in 2008 was more effective than a normal talk.Telemedicine enabled Hospital on Wheels – In 2005 As part of the Distance Healthcare Advancement Project, along with Philips Medical Systems, ISRO, and the DHAN Foundation, a Hospital-on-Wheels (HoW) was made. The HoW would go to different villages and provide virtual teleconsults. Concentrating on the vehicle, its contents and satellite communication infrastructure. the low lying branches of trees and mud roads in villages was overlooked !! Subsequent VSAT receivers were made smaller and portable.Formation of TSI At the Telemedicine conference organized by ISRO at Bengaluru a few of us got together and decided to formalize the concept of TSI first mooted by Dr Saroj Mishra in 2001 at Lucknow. I became the first Treasurer ( and Joint Secretary) of TSI with the membership number of 001!!
2006- 2010
The next few years witnessed evangelisation of Telemedicine in India and overseas. Talks were given at Baghdad, Kosovo, Riyadh, USA and many other countries in the Middle East and Africa. Every opportunity was used to promote telemedicine. By this time, India has been placed on the world map in Telemedicine.Gradually VVIPs’ from other countries started to take notice of the work done here. The Prime Minister of Mauritius, the President of Nigeria and many, many other heads of states started visiting us to understand how we were making a difference. This resulted in setting up of telemedicine units in Lagos and Mauritius.Following visits from ministers from Uganda I received a “summons” from the First Lady of Uganda for a discussion to set up telemedicne units in Kampala. CII, FICCI and other organisations were pro actively contacted . Seminars, symposiums, workshops and conferences were conducted on a war footing throughout the length and breadth of India. Telemedicine became my second name. The audience were not convinced – ravings of another mad man ! . When The National Science Centre located at the National Science Museum New Delhi started a new gallery to showcase recent advances in science and technology a Telemedicine kiosk with facilities for live demos was set up. ATNF became a member of the Standards Committee on Telemedicine, the National Task Force on Telemedicine, the Working Group on Telemedicine of the Planning Commission, and the Working Group of the SARC Committee on Telemedicine.
International Conferences personally organised : In Nov 2007 the 3rd national conference of the TSI was held in conjunction with the 12th international conference of the International Society for Telemedicine and eHealth at Chennai. The conference was inaugurated by the Chief Minister of Tamilnadu. Over 300 Indian and 35 international delegates participated. In 2016 the ISfTeH conference was again held in Chennai along with the annual Conference of Transforming Health Care with IT Over 750 delegates participated. THCIT annual conference has been held regularly for the last decade.
mHealth – In August 2007 Ericsson requested me, to study for the first time in South Asia, the feasibility of remote clinical examinations through wireless connectivity. Special license was obtained to use 3G spectrum .We demonstrated that 12 lead ECG’s, blood pressure recordings, lung and heart sounds ,ultrasound studies and ECHO cardiograms could be transmitted wirelessly using 3G. For the trial demo availability of power for 10 hours in the outskirts of Madurai was organised. Backup generators with diesel for 4 hours as a standby was arranged. Due to an unexpected demise, staff of the Electricity Board left and there was no power !!. Getting additional diesel would take at least 4 hours. Diesel from two ambulances and a bus was removed and used. An example of how determination can solve any problem.This 3G trial was so successful that Ericcson requested us to showcase this in Bhutan and Bangla Desh. In July 2008 The Rockefeller Foundation organised a Making the eHealth Connection Conference at Bellagio Italy. I was invited for the 5 day brain storming session. The very term mHealth was conceptualised by mygroup.
Global telehealth initiatives of Govt of India – The Ministry of External Affairs, Govt. of India initiated the Pan Africa e-Network project for teleconsultations in 2009. ATNF was a major player in this project .Unfortunately the project was not sustainable. Again to advise the government on the Central Asia e-Network Project. I visited Uzbekistan, Kazakhstan and Turkmenistan and submitted a project report. This also did not materialise.Formation of ATHS . With increasing activities it was realised that we needed a full time CEO to head a regular company rather than a full time Neurosurgeon involved in Telemedicine as a passion . This suggestion was accepted and in October 2010 Apollo Telehealth Services was formed. An excellent team under the leadership of Vikram Thaploo has made use of the rich heritage. Being future ready the outstanding team have managed to operationalise what were originally concepts. My wish list is becoming real . It is also true that “ nothing can stop an idea whose time has come”. Today ATHS has one of the largest Call Centres and is the oldest and largest multi speciality Telemedicine Network in South Asia.
2011
eHome Visits Belonging to the BC era ( Before Computers, Before Christ & Before Covid are the same !!) I was keen on reviving house visits which were in vogue in the early seventies. Electronic house visits were initiated with a laptop/ dongle carrying attender connecting from the uninitiated patient’s home.Interestingly this simple innovation got the best poster award at the World Health summit at Washington in May 2011
2012
World’s largest number of Teleconsults from a HoW – In a first of its kind initiative, 527 patients in 13 different specialities were connected simultaneously to six tertiary Apollo hospitals, in different parts of India from a HoW at a mega health camp held at Ajmer in Northern India on 11th and 12th February 2012.Remote clinical evaluation was followed by ePrescriptions. Subsequently similar telecamps were held in different parts of Tamilnadu in southern India.
2014
Patient empowerment in rural India by promoting eHealth Literacy -Deploying multi point Videoconferencing, a knowledge empowerment programme, at the internet enabled Village Resource Centers of the MS Swaminathan Research Foundation, in rural Tamilnadu was started in 2014 . 115 talks have been given in Tamil so far attended on 25,000 occasions from 18 villages.
2015 ONWARDS
Virtual visits to ICU I-SEE-U® was a state of the art solution developed to enable virtual visits to ICU patients, from anywhere in the world, by authorised consultants, friends and relatives. The remotely enabled networked camera in the individual ICU cubicle can also focus on various monitors. The product got an award at an international conference at Singapore. Due to subsequent regulatory and privacy issues it was discontinued.
International Educational Activities : Columbia University , Wharton School of Business, the London School of Economics, Harvard Business school, Ross School of Business, Atlanta state University, Indian school of Business are some of the international organisations who have used Apollo Telemedicine as study material .Software An in house, custom built software “Medentegra” which in addition, to a user friendly EMR (facilitating uploading of images, investigations etc.) has inbuilt video conferencing capabilities started being used regularly.
eICU : eICU’s where smaller ICU’s are connected to highly trained experienced intensivists in larger ICU’s are now a reality. One of the largest such networks operates from Apollo Hospitals Hyderabad where 15 ICU’s are connected. 600 plus teleICU consults in subspecialoitries have already been given.
Public Private Partnerships – a few illustrations
a) Himachal Pradesh . The first Telehealth PPP project in India commenced 5 years ago . Over 18,500 teleconsultations were given at a height of 14,500 ft. The world’s first 24/7 Tele emergency Services has seen about 1300 patients. Today we have four different Telemedicine Centres in Himachal Pradesh
b) Over 1 million teleconsultations have been provided under the Mukhyamantri Arogya Kendram (e-UPHC)- project covering 182 Centres from October 2016.
c) Jharkhand Digital Dispensaries programme In the first 15 months alone 328,648 patients have attended these Digital Dispensaries
d) Uttar Pradesh Telemedicine programme in the first one year 141,793 patients visited 114 Government Community Health Centres
e) Uttar Pradesh Teleradiology PPP program – Systematic implementation of operational activities, beginning from site development and installation of IT equipment to training of human resource and trial testing for assessing functional status of Centres has led to commissioning of 127 teleradiology centres in rural UP – a mammoth undertaking by any standards. On an average 360 images are reported daily with a turn around time within 4 hours
f) Tele ophthalmology A major project is being carried out in 115 existing Community Health Centres / Vision Centres run by the Department of Health and Family Welfare, Government of Andhra Pradesh in 13 districts. Through this Mukhyamantri e-Eye Kendram or MeEK project 1,5 million patients have been screened in 2 years. 355,000 fundus examinations were done remotely by 30 Opthalmologists from Chennai .
g) National Thermal Power Corporation . Located in rural Assam 30 km from the China Border this Telemedicine enabled center has made a major difference.
2019
Extra-terrestrial Telemedicine . The ultimate in Remote Health Care would be to assist in providing health care to India’s first Vyomanauts in Outer Space . After editing a special supplement on “ Extra Terrestrial Neurosciences” for Neurology India and presenting the only medical paper at the Human Spaceflight Programme organised by ISRO, I have even offered my services !! 2020 Academic contributions – The crusade for popularizing telemedicine has included the presentation of more than 400 papers in regional, national and international meetings in India and 105 overseas . Over 180 articles have been published, on Telehealth including 45 in peer-reviewed journals and chapters in textbooks
Conclusion:
The journey has been exhilarating . I have no regrets for taking the road less travelled by. Encomiums and accolades received on reaching the destination is only ephemeral. The greatest danger for most of us, is not that our aim is too high and we miss it, but that it is too low and we reach it. The TSI should not believe in following high standards. We should set them. We no longer should strive to achieve world class. The world should strive to achieve India class. Looking back, the growth of telehealth during the last 20 years has been rather slow – many of us are in a hurry, impatient, wanting to get things done yesterday !!. The first decade was spent in evangelising the product, developing the product and generally creating awareness . For a product to excite the masses it must elicit customer delight and cater to the consumer. A major stumbling block retarding the take off of telemedicine is WiiiFM ( What is in it For Me). Every member of the telehealth ecosystem needs to get a RoI ( Return on Investment) not necessarily monetarily alone. In the third decade of telehealth business models are mandatory. Revenue generation is a must for sustenance. Philanthropy and corporate social responsibility can initiate an activity not maintain it.
Epilogue: Not in my wildest imagination would I have ever expected the slow incremental annual growth to radically transform into an explosion. A strand of RNA has become the Global CTO ( Chief Transforming Officer) for Telehealth. Contactless Health care will be the new normal.Distance will become meaningless. Geography will become History!. Recognition of Telemedicine by Insurance companies augurs well. Formal recognition of importance of Telemedicine by the Govt of India and state governments will make all the difference, I once gain thank the TSI for bringing out a Newsletter . Hopefully the newsletter will bring our ever expanding family closer .
Fig 1 Earliest communication for starting Telemedicine
Fig 2 Inauguration of world’s first VSAT enabled village hospital for Telemedicine March 24th 2000 @Aragonda, Andhra Pradesh
Tele-Ophthalmology – in a COVID world – Opportunities and Challenges Dr. T. Senthil, MBBS DO FICO. Founder and CEO Welcare Health Systems Pvt ltd – Honorary Secretory, Telemedicine Society of India Tamil Nadu Chapter. Dr. Senthil is an Ophthalmologist and Healthcare Entrepreneur, He established Welcare Health Systems in 2014 which has grown to become Indias Largest Teleophthalmology Company. He can be reached at senthil@welcaretelemed.com.
COVID 19 has brought in a drastic change in adoption of Teleophthalmology among Ophthalmologists in India. Since patients were not able to reach hospitals, and social distancing became the norm, hospitals in Corporate, Govt and Non-Profit sector started looking for Teleophthalmology Solutions to reach out to their patients. In Ophthalmology Telemedicine was used primarily in three scenarios. 1) Screening for Diseases such as Diabetic Retinopathy, Retinopathy of Prematurity etc. 2) Diagnostic Consultations. 3) For Long term follow ups of patients.
Screening for Diseases through Teleophthalmology has been the most successful of the above three models. There are many successful Screening projects in Teleophthalmology world over which has reached out to millions of patients. However, Challenges faced by Screening model providers are cost of the Technology such as fundus cameras, Internet connectivity, Paying capacity of patients etc.
The Diagnostic Consultation approach started getting traction during the COVID lockdown, since patients were not able to reach hospitals- they wanted to connect to Ophthalmologists from their homes. There was a huge spike in Teleconsultations during the initial lockdown periods. Hospitals and Clinics started teleconsultation services to reach patients. Many platform companies were able to generate patients to Ophthalmologists for consultation. The teleconsultation slowly started decreasing as Hospitals / clinics opened.
Challenges in Ophthalmic Teleconsultation a) Ophthalmology diagnosis includes a few basic tests such as Examination of Eye on a Slit Lamp, Fundus Examination, Refractory error examination etc which cannot be done in the patients’ homes since the equipment’s are not available for these tests. b) The willingness of Patients to pay for a online consultation was very poor. c) The Ophthalmologists also have a lot of apprehension on missing Diagnosis using a Teleconsultation mode.
The most effective model during the COVID time for Ophthalmology was for follow up of patients such as Postoperative patients where advise was given on Medication changes, or Tele triage wherein patients were seen online and decision was taken if they have to come to Hospital or can be advised online, or even if they come to hospital which specialist they had to see and so on.
For Teleophthalmology to Succeed 1) Low cost Diagnostic Devices such a Fundus Cameras and ROP cameras to be available in the market. 2) At Home Screening devices for Intra Ocular Pressure Measurements, Refraction and Visual acuity Measurements, Fundus / Anterior Segment Imaging to be innovated and made available. 3) Medico Legal Clarity and Data Protection Clarity to be brought in so that Doctors will be more comfortable in doing Teleconsultations.
Mobile Teleopthalmology
Dr. Sheila John, Consultant Ophthalmologist, Head of Teleophthalmology and E-Learning, Sankara Nethralaya, Chennai.
Mobile Tele-ophthalmology is evolving into an integral clinical tool in the Indian health care system. In a developing country like India, the ophthalmologist-patient ratio stands at a dismal 1:10,000. What makes this wide gap between demand and availability of eye care even more critical is its inequitable spread, 70% of the nation’s citizens live in rural areas while 70% of its eye care professionals live in urban areas.
Mobile Tele-ophthalmology BUS may potentially provide health services to underserve and remote rural populations who otherwise may not have access to specialized eyecare. Eye screenings are conducted within the community, often in schools, community halls, and places of workship.Bringing the facility directly to the patients allows health professionals to diagnose and prevent vision threatening diseases such as diabetic retinopathy, glaucoma, age-related macular degeneration and others By detecting causative blinding disease early on mobile, teleophthalmology allows for timely referral to appropriate experts and consequently, earlier treatment. However, on-site screenings may utilize the state of art equipment including an automated refractor, slit lamp with Applanation tonometer, Non-mydriatic retinal camera and others. An ophthalmologist is available in person at the hospital to do teleconsultations with the patient and develop an assessment and treatment plan for the screened patients. The ‘Mobile Refraction Van ‘accompanies the teleophthalmology van to the villages, addresses the refractive error, and dispense spectacles to rural people at campsite.
As an institution committed to its founding principle of cost free service with a personal touch to those who cannot afford to pay, Sankara Nethralaya realized right from the time of its inception that for every single indigent patient who visited its centers seeking cost free eye care there were two such patients outside needing such care. It also realized that patients in rural areas may not avail eye care dispensed at a base hospital in the city owing to several socio-economic factors and the only way to dispense preventive and curative eye care to this segment would be through outreach programs. ‘Mobile Teleophthalmology’ holds great potential to improve the quality, access and affordability in eye care especially for patients in rural areas by reducing the need for travel and providing virtual access to a super-specialist right at their doorstep.
Best practices!
Indiritta Singh Dmello, Director, Hospital Guide Foundation (An Oxford graduate in Politics, Philosophy & Economics with a PG Diploma in Medical Law & Ethics-National Law School, Bangalore)
“The developed India will not be a nation of cities. It will be a network of prosperous villages empowered by telemedicine, tele-education & e-commerce”-Dr. A.P.J. Abdul Kalam.
It is paradoxical that even though India has emerged as a hub for medical tourism, we are unable make healthcare accessible and affordable to the masses in India. As per the WHO statistics, India is far below the recommended Doctor Patient Ratio (recommended ratio 1:1000 & India1:1700). Further compounding the problem is that only 26% of these Doctors are present for 70 percent of the population in rural areas.
This is where Telemedicine plays a pivotal role in addressing this gap. Telemedicine is a tool that makes healthcare accessible and cost effective by engaging the Doctors and patients remotely through an integrated technology platform. This platform could be as basic as a simple Audio Visual with a software for patient details or as advanced as integrated diagnostic equipment, remote monitoring of Intensive Care Unit Patients or even remotely conducting a surgery.
Hospital Guide Foundation (HGF) has been running a Telemedicine project with the Govt of Uttar Pradesh in the rural area of Western UP, supported by the Doctors of National Heart Institute & Sita Ram Bhartia Institute of Research & Technology at New Delhi. While it is a Telemedicine project, the objective is to provide comprehensive healthcare with Telemedicine being an enabler. At HGF the following key factors were observed for making a Telemedicine project successful.
Holistic Approach: Telemedicine delivers significant advantages for the patients only with a complete treatment and support mechanism – ensuring tests & medicines, setting right expectations, counseling (about the process, disease & treatment), driving awareness, ensuring compliance with (tests, medicines & life style) and pro-active follow ups, which helps gain patient confidence & cooperation therefore delivering much better results.
Seemless process: Multiple touch points have to be managed seamlessly between patients, nurses,Doctors and telemedicine specialists for enabling a great healthcare experience. This makes it even more challenging in rural areas where we grapple with basic problems like electricity. Coordination to perfection is key for a sustainable telemedicine project, specially when the Doctor’s limited time should be well spent on communicating with patients rather than waiting for them.
Optimal technology: is also essential for a superior Doctor & patient experience. For eg the quality of internet bandwidth, audio visual can affect the dialogue between patients and Doctors who are trying to communicate remotely on sensitive health issues. The quality of communication will have a direct impact on the diagnosis, prognosis and treatment.
Quality diagnostics: Similarly, well calibrated high tech diagnostics is essential for the patients to get the right diagnosis, prognosis and treatment.
With the onset of the Pandemic COVID 19, Telemedicine has gained the much needed impetus that it has been yearning for. As it has become an important enabler in Healthcare delivery, not only for reasons of accessibility, affordability but for reasons of safety. In a country where there are several Telemedicine projects running in silos, it is important to continuously share best practices , for which Telemedicine Society of India (TSI) is a great platform & this newsletter a great initiative. With the astute leadership of TSI, I have no doubt that Telemedicine will be on a trajectory it so deserves!
Train to Practice Telemedicine Guidelines
Ms. Bagamishika Puhan, Advocate, Legal Advisor and EC Member, Telemedicine Society of India, Member, Indian Society for Clinical Research.
On April 04, 2020, after a tumultuous yet short ride, a group of TSI members came together to unfurl the Train to Practice project. This was the culmination of an informal mandate received from a benefactor to train and educate as many registered medical practitioners (RMPs) about the nuances of the Telemedicine Practice Guidelines (TPG) in particular and telemedicine in general.
The Society pioneered work in the field of telemedicine over the past many years, and now, is at the helm of inculcating the best practices in the field and has been successful in training over 3500+ RMPs directly under the project, and about 15000+ RMPs through the volunteers.
In this exercise, the focus has been to ensure that the participants take away an acute understanding of the legal aspects of telemedicine (TPGand allied laws), how to marry the legal concepts to their clinical practice, and also a basic understanding of how and when to triage a patient by means of telemedicine. As we continued with the project, we added another module which lends a helping hand to the practitioners who want to get started right after the discussion, with their own kit of telemedicine.
The project has witnessed roaring applause from various factions including the much revered Armed Forces Medical Services for the volunteering efforts and the dynamism of the project and the team. We have also sought support from entities who believe in this social and evolving practice of telemedicine. As the awareness amongst the user increases, we will continue to ensure that safety is not compromised, and we will continue to impart the necessary education concerning safe and convenient practices around telemedicine.
We welcome participation of volunteers to train, to learn, and to contribute to this endeavor of the Society in any manner and capacity that they wish to associate with the Society. Learn more at https://tsi.org.in/learn
History and Evolution of Telemedicine – Samuel Morse and Telegraph Dr. Sunil Shroff, President, Tamil Nadu Telemedicine Society of India, Consultant Urologist & Transplant Surgeon.
History and Evolution of Telemedicine – Samuel Morse and Telegraph (First of Ten important milestones). “The Past supplies the key to the Present and Future“ ~ Ancient Historian. The history of telemedicine is the history of evolution of distance communication. If it was not for the legacy laid down by many of the scientists, telemedicine may have never evolved as it has done currently.The start of this was the invention of the public telegraph system set up by Samuel Morse. Why did Samuel who had developed a reputation as a portrait painter go on to invent the telegraph system?
This is an interesting piece in the history of communication. Apparently he was hired to paint a portrait of a famous person and travelled out of his town. Back at home his wife fell ill and died of heart attack and it took Samuel days to reach back home and when he did return the wife’s funeral had already taken place.He was so upset with this episode in his life that he left his art career and started looking at ways to establish a way to communicate information at a distance. His pursuit lead him to become interested in the telegraph system.
He went on to invent a single-wire telegraph system and the first Intercity public telegraph services were set up between Washington and Baltimore in 1844. In almost all the wars that followed the telegraph was used by the military to order medical supplies, transmit list of casualty and it is probable that some use of the telegraph in its early decades involved medical consultations.He was also the co-developer of Morse code that helped the commercial use of telegraphy. One of such codes was the internationally recognized distress signal SOS. The SOS letters were chosen because they are easy to transmit in Morse code: “S” is three dots, and “O” is three dashes.
Telemedicine – News from India & Abroad
India
500% rise in healthcare teleconsultation in India, 80% are first-time users: Report Besides COVID-19 related symptoms, some of the other most-discussed queries included back pain, eye health and mental health issues. Online consultation for healthcare has increased by 500 per cent between March 1 to May 31, 2020…… Read More
Digital Care: The Way Forward for Management of Chronic Conditions The use of digital care in driving positive health outcomes, especially for chronic patients, it is possible because of the availability of remote monitoring and virtual care tools backed by the spread of affordable smartphones and data consumption, it’s the next major emerging disruption in India after e-commerce, fin-tech ….. Read More
Telemedicine is the roadmap to improve medical Care in rural areas : Ayush Mishra According to the Medical Council of India the doctor to patient ratio in India may be as low as 1:2000 if not lower. This is a serious challenge to the health of Indians and is compounded by the fact that most doctors practice in larger cities where opportunities are greatest …. Read More
Today technology can make physicians available to patients: Sunil Wadhwani Artificial intelligence really can have dramatic impact on how we address healthcare in India, how we can become the leading country in the developing world, on how AI is being applied to improve healthcare…. Read More
Telemedicine Guidelines Released in India Notified and Gazetted The Government of India Notified and gazetted the Telemedicine Guidelines that were released on 25th March 2020. What it means is that this framework is here to stay even after the current COVID-19 pandemic recedes. While 25th March was a historic day when the guidelines were released by the BOARD OF GOVERNORS – In super session of the Medical Council of India under NitiAayog, 14th of May the guidelines have officially been notified and gazetted. Read More
International
Telehealth Services: A Post COVID-19 Reality? The regular use of telehealth services for cancer patients was found to have long-lasting and unforeseen effects on the provision and quality of care, said an article published in JAMA Oncology, Trevor Royce, MD, MS, MPH, an assistant professor of radiation oncology at the University of North Carolina Lineberger Comprehensive Cancer Center and UNC School of Medicine. Read More
Heart Failure Assessment Via Telemedicine The jugular venous pressure is an indicator of fluid retention and build-up of pressure inside the heart. Being able to check jugular venous pressure using telemedicine, virtually, will help doctors assess heart failure patients remotely by just using the camera on a smartphone. Read More
Digital Health Unplugged: August news team debrief During the Covid-19 pandemic primary care was forced to go digital-first to avoid unnecessary face-to-face consultations in a bid to control the virus, but now lockdown restrictions are easing are those services here to stay? Speaking at a Royal College of Physicians event in the UK on the future of healthcare post-Covid, Hancock said teleconsultations would allow the NHS to provide a “much better” service. Read More
Telemedicine Market- Growth Insight, Rising Demand, Share and Healthy CAGR in the Upcoming Forecast 2024 BY NEWS@RESEARCHNESTER.COM ON AUGUST 11, 2020 Global Telemedicine Market is growing immensely due to its growing application; Tele-cardiology, Tele-radiology, Tele- dermatology, Tele-gynecology etc. At 19%, Tele-dermatology had the highest share in the global applications market in 2015 and is expected to lead in next five years followed by Tele-cardiology. The report titled, “Global Telemedicine Market 2024”, projects the global Telemedicine market to grow at a CAGR of 14.8% during the forecasted period of 2017-2024 according to our research report. Read More
TN – TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.
Submission may be sent to – tsigrouptn@gmail.com Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff Editors – Dr. Senthil Tamilarasan & Dr. Sheila John Design – Sankara Nethralaya Technical Partner- www.medindia.net


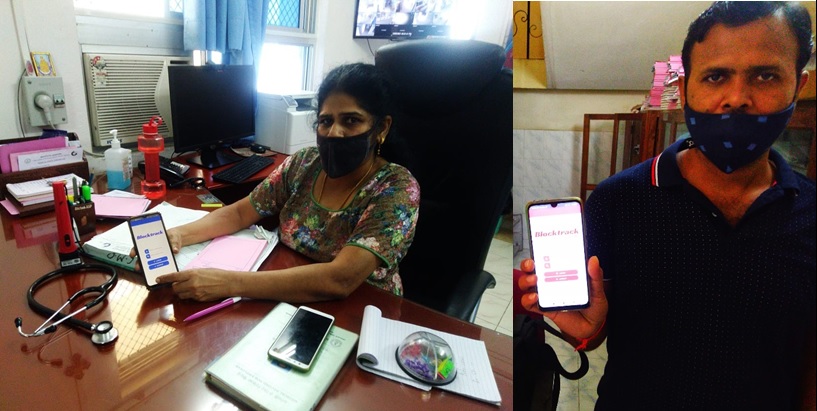
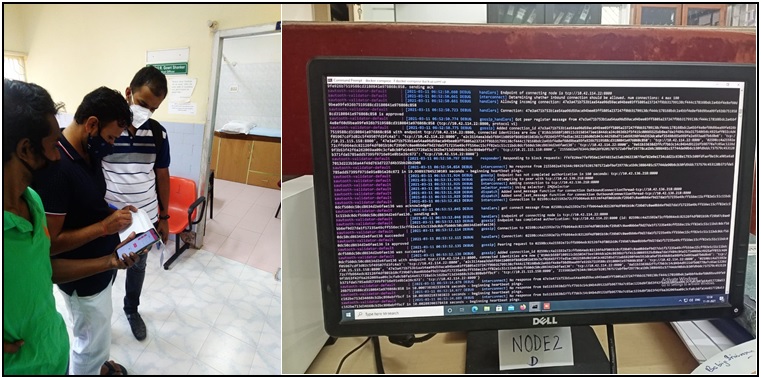

 Teleophthalmology Adoption – Barriers and Solutions
Teleophthalmology Adoption – Barriers and Solutions