Click Here to Download PDF Version
Telehealth Newsletter
Official Newsletter of Telemedicine Society of India

What is New?
The month of March has been marked by three important milestones for the Society.
The first was a webinar to discuss the requirements of the new Telemedicine Practice Guidelines (TPG), which are expected to supersede the original guidelines issued in March 2020 during the COVID-19 pandemic by the National Medical Commission (NMC). This 70-minute webinar was attended by the Director of the Ethics Committee, Mr. Abhijeet Chakraborty.
Following the discussions, it was decided to constitute a committee to redraft the TPG, incorporating relevant provisions from the Digital Personal Data Protection (DPDP) Act as applicable to healthcare, and to further elaborate on the role of AI in telemedicine practice. Key deliberations also included the need to move away from the distinction between first and follow-up consultations, revise and expand the medication lists, strengthen the role of caregivers in consultations, and more clearly define the standard of care within the guidelines.
The key event was the inaugural one-day conference of the Gujarat Chapter of TSI, held in Ahmedabad. The conference brought together experts and stakeholders, fostering meaningful dialogue and strengthening collaboration within the field. Dr.Rajrawal along with his team pulled off a stellar show.
These initiatives reflect the growing momentum of TSI and reaffirm its commitment to advancing its mission across diverse regions of the country.
In this issue, I have also addressed an emerging concern associated with the rapid adoption of AI in healthcare-“Shadow AI.” I encourage you to read the article and deepen your understanding of this important and evolving risk.
Thank You
Dr. Sunil Shroff
Chief Editor
President, TSI
Transitioning to Digital Public Health
Dr. K. Ganapathy
Hon Distinguished Professor IIM Jammu
Distinguished Professor, The Tamilnadu Dr MGR Medical University
Emeritus Professor, National Academy of Medical Sciences
Formerly Distinguished Visiting Professor IIT Kanpur
Past President, Telemedicine Society & Neurological Society of India
Formerly WHO Digital Health expert
(This article was published in the March 2026 issue of Medical Buyer and is reprinted with-permission)
Surgery of the unborn and robotic telesurgery is thrilling but a digitally enabled Public Health medical doctor working with policy makers and civil servants can do greater wonders What does India need? Digital Public Health or helicopter ambulances & intra operative MRI?Digital Public Health can radically transform Healthcare. No longer do we leap frog – after all how far can a frog leap – we have already started pole vaulting!
It was in 1998 that I first encountered the term “Telemedicine”. At the peak of my neurosurgical career, I got bitten by the IT bug. I realised that as a neurosurgeon I could at best contribute to the care of several thousand individuals. However technology enabled remote health care could make distance meaningless and Geography History! The urban rural health divide then was striking. In 2015, in a now oft quoted publication I had shown that 935 million Indians lived in areas where there was not a single neurologist or neurosurgeon. In this milieu it has been amazing to see the phenomenal transitioning to DIGITAL PUBLIC HEALTH (DPH) an entity which does not exist even today in scores of countries.
Introduction to DPH
India is now regarded as a global leader in DPH, especially among LMIC. India influence strategies even in high‑income settings. India is distinctive not just for scale, but for using open, interoperable (DPI) Digital Public Infrastructure (ABDM, CoWIN, UPI, Aadhaar) as a health “railway” rather than a collection of isolated IT projects. India’s ABDM is explicitly framed as a DPI – open APIs, federated data, consent-driven exchange, and a unique health ID (ABHA) that can work across public and private providers. It cannot be denied that a strand of RNA acted as a Global CTO (Chief Transformation Officer). Ensuring vaccination 2 billion times seamlessly making available digital certificates, demonstrated that India no longer leap frogs. We pole vault!
DPH Illustrations
Ayushman Bharath Digital Mission has a laudable goal of having an interoperable digital infrastructure for all health actors. This citizen-centric, consent‑based health data exchange could provide a digital documentation, never achieved. eSanjeevani the Govt of India Telemedicine platform is used about 400,000 times a day. 430 million teleconsultations have already been documented. As a guestimate probably 200,000 teleconsults occur daily using other platforms. 875 million ABHA numbers have been created. 350 million digital health records have been linked. 285,000 professionals and 400,000 institutions have been onboarded in ADHM. 5,000 + Real-time outbreak detections have been documented. Queue Time has been reduced from 35 minutes to 5-10 min in 75% of instances. Claim Processing became 85-90% faster- from 30 days to 4 days.
Success of DPH
Built on national DPI, Digital Health (DH) was treated as a public good, not a product. India has demonstrated that population‑scale DH platforms can be implemented at very low per‑capita cost, using cloud, open APIs, and a modular DPI stack. India built health on top of existing national rails: Aadhaar (ID), UPI (payments), Digi Locker (secure document storage), and India Stack APIs. ABDM was then added as a health‑specific DPI. Steps preceding the implementation of DPH is critical. Early foundational work (digital ID, payments, visible, high‑impact success eg. Cowin’s 2 billion doses, real‑time dashboards helped create political and public confidence which is vital. Prior investment in governance, change management, allocating specific budgets for digital infrastructure, workforce training and maintenance was as important as software and hardware.
Challenges and how they are addressed
These include large rural and older populations, reduced device access, urban-rural digital divide, digital illiteracy, variable connectivity, privacy, cybersecurity, interoperability governance in a rapidly scaling system, increasing workload for health workers and institutions and workflow disruption. Building DH systems on top of robust national DPI, addresses many issues. Attention to Change Management, designing explicitly for equity, assisted access, multilingual interfaces, offline capability and federated, consent‑based data sharing is essential. Collaborating with private sector and tech companies to co-develop, maintain, and scale digital solutions ensure sustainability and innovation. Designs for the majority, not just the digitally literate is essential as is ensuring interoperability with other sectors and Digital competency among health professionals.
Deployment of AI in DPH
The enormous backing, to deployment of AI in the private and surprisingly the public sector, in all areas of healthcare will soon yield tangible measurable dividends. In DPH, AI is being used in management of TB, vector‑borne diseases, maternal health, radiology and predictive analytics.
Conclusion
India aims for near‑universal DH coverage, with AI‑enabled predictive public health, integrated chronic disease management and digitally competent health workforces. Healthcare should not become digital care. Healthcare will no longer depend on where one lives, but how well one is digitally connected. Technology is a means to achieve an end, not an end by itself. A fool with a tool is still a fool!! Digital should be the foundation, so healthcare can focus on human dimensions that no algorithm can ever replace.

How ‘Shadow AI’ Can Endanger Healthcare Ecosystem
Dr. Sunil Shroff
President, Telemedicine Society of India | Consultant Urologist & Transplant Surgeon
Artificial intelligence (AI) is making inroads across all domains of medicine
We are already seeing promising applications of AI such as:
Predictive models to identify high-risk patients and anticipate outcomes
Natural language models (NLMs) enabling conversational AI for emotional and psychological support
Administrative streamlining, reducing clinician burden and improving efficiency
Although the use of AI in medical specialties-is still evolving. There are important limitations and challenges that must be addressed, including data privacy, ethical concerns, and the need for robust validation studies.
I am particularly concerned about the current level of digital literacy among healthcare professionals. Increasingly, doctors and nurses are using tools like ChatGPT in their daily practice. The concern arises when patient information is entered into such platforms, as this data may be stored or used for training purposes. This creates a real risk of data leakage, breach of confidentiality, and violation of patient privacy.
What is Shadow AI?
Shadow AI refers to AI tools and models used inside a health system without formal approval, governance, or oversight. This can include consumer apps, chatbots, or vendor models that clinicians or staff adopt on their own. While convenient, Shadow AI poses real risks to patients, data privacy, and regulatory compliance.
Why this matters for you as a Clinician
1.Patient safety: Unvetted tools can give inaccurate or non-reproducible outputs, potentially affecting diagnoses or treatment plans.
2.Privacy and data security: Patient health information (PHI) may be uploaded to non-compliant tools, risking breaches or misuse. Data may be used to train external models without proper agreements.
3.Compliance gaps: Many AI tools fall under regulatory rules (HIPAA, FDA SaMD, GDPR). Shadow use can create blind spots with no audit trail.
4.Data quality and interoperability: Outputs may drift, be biased, or not integrate with EHRs, leading to inconsistent records.
What to do in daily practice
5.Use sanctioned tools only: Rely on the institution’s approved AI toolkit and guidelines. If unsure, pause and ask your supervisor or IT.*
6.Protect PHI: Do not upload or paste PHI into unapproved tools. Check data-sharing terms and ensure BAAs are in place before any use that involves PHI.
7.Validate and review: Treat AI outputs as decision-support. Always review against your clinical judgment, patient data, and local protocols before acting.
8.Documentation and audit trail: Record tool name, version, inputs, outputs, and how the result influenced care in the patient record where required.
9.Be transparent with patients: If AI assists care decisions, disclose its role when appropriate and be prepared to explain its role and limitations.
10.Security and privacy hygiene: Keep devices updated, use institution-approved networks, and report unusual data requests or tool behavior.
11.Report and escalate: If you encounter or suspect Shadow AI use, report to your supervisor, IT/privacy, or the AI governance contact. Do not ignore potential risks.
12. Check the AI app security: Switch off section for data sharing for training
13. Delete chats and initiate temporary or “non-retained” chats (including ChatGPT), and they are one of the key safeguards to reduce data exposure. But they are not a complete solution
Simple Safe Practice Rule which everyone can follow:
Turn off data sharing / training always
Use temporary chats where available
- But NEVER enter identifiable patient data unless:
The tool is institution-approved
There is a formal data protection agreement
It is clinically validated and secure
Activating these safeguards should be the first step before using any AI tool more so if you are using it in a clinical context. We must also recognize that we are now governed by the Digital Personal Data Protection Act, under which penalties for violations can go up to ₹250 crore. Even a single high-profile breach could not only affect an individual clinician but also create widespread fear, potentially stifling innovation across the healthcare sector.
Bottom line Shadow AI can undermine patient safety and privacy if left unchecked. Use only approved tools, understand data handling, and engage governance processes.
AI holds tremendous promise-but it must be used responsibly and ethically. Let us embrace innovation, but not at the cost of patient safety, trust, and professional integrity.
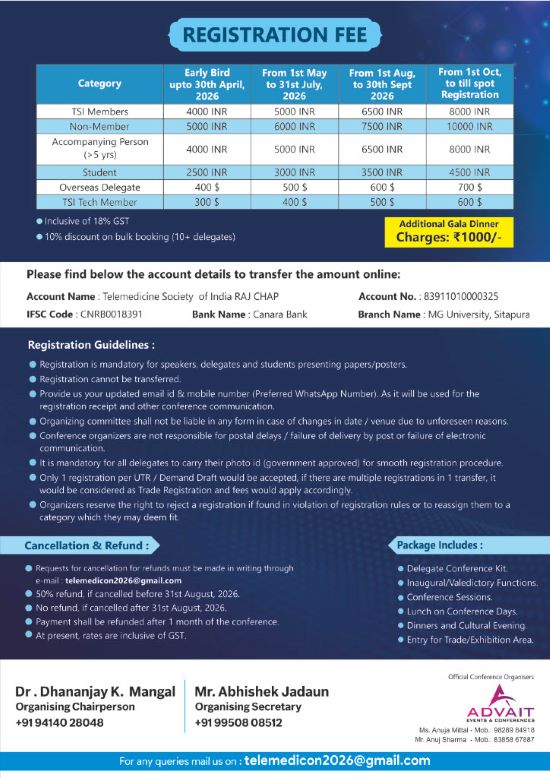
TSI GUJCON 2026 Conference
DATE : 22/03/26, SUNDAY
VENUE : ATAL-KALAM BHAVAN, GUSEC
TSI GUJCON 2026 conference, focussed on the strategic, legal, and technological evolution of telemedicine in India.
Inaugural Session: Strategic Vision and History
ISRO’s Role: Dr. Nilesh Desai (Director, SAC-ISRO) highlighted ISRO’s 25-year legacy in telemedicine, including a recent MOU with Integrated Defense Services. He introduced future technologies like “Satcom on the Move” (mobile telemedicine nodes) and Quantum Key Distribution (QKD) to secure medical and financial data.
Digital Health Vision: Dr. Sunil Shroff (President, TSI) emphasized that technology is now a primary care driver, moving toward precision medicine while cautioning that the “human touch” must remain central.
- Ecosystem Growth: Dr. Shrinivas Rao (CEO, GUSEC) discussed the “telemedicine revolution” and GUSEC’s role in incubating med-tech startups to reach inaccessible regions.
Session 1: Implementation Challenges in India
Panel Discussion: Moderated by Dr. Vivek Dave, the panel addressed infrastructure and digital literacy gaps in rural India.
- Key Takeaways:
- The Telemedicine Practice Guidelines (TPG) 2020 provided the essential legal framework that protected both patients and doctors during the pandemic.
- Panelists discussed “website manners” to improve patient empathy during video calls, such as looking at the camera rather than the screen.
- The Hub and Spoke model was identified as the most effective rural delivery method.
Session 2: Ayushman Bharat Digital Mission (ABDM)
- Building Blocks: Dr. Vatsrajani detailed the implementation of the ABHA (Ayushman Bharat Health Account), which allows for consent-based, paperless health record sharing.
- Professional Registries: The session urged all doctors to register on the Healthcare Professional Registry (HPR) and Health Facility Registry (HFR) to integrate into the national digital backbone.
- Incentives: The government is offering digital health incentive schemes (DHIS) to hospitals to encourage the linkage of digital health records.
Session 3: Digital Health Law, Ethics, and Responsible Innovation
- TPG Compliance: Dr. Sunil Shroff provided a deep dive into the TPG 2020, clarifying that telemedicine is an enabler, not a replacement, for traditional care.
- Record Preservation: Records must be kept for 3 years (10 years for medico-legal cases).
- Shadow AI: A critical warning was issued regarding “Shadow AI”—the unauthorized use of public AI tools (like ChatGPT) with sensitive patient data, which can lead to severe privacy breaches and massive legal fines under the DPDP Act.
Session 4: Data Privacy and Cyber Security
- Threat Landscape: Mr. Dhaval Davesar highlighted the CIA Triad (Confidentiality, Integrity, Availability) and the rising threat of ransomware in healthcare, citing the KD Hospital attack as a case study.
- Security Protocols: The session covered vulnerabilities in IoT medical devices (e.g., infusion pumps) and recommended regular security audits and avoiding public Wi-Fi for clinical work.
Session 5: Deep Dive into Tele-Medicine Practice Guidelines
- Regulatory Framework: Dr. Krishna Kumar clarified that TPG remains legally valid under the NMC Act 2019.
- Consultation Categories: Detailed the requirements for “First Consult” versus “Follow-up Consult” and the strict categorization of drugs (Lists O, A, B, and Prohibited) that can be prescribed remotely.
Session 6: Tele-Robotics and Future Surgery
- Milestone Achievement: Dr. Sanjiv Haribhakti presented the first tele-robotic surgery in Gujarat, performed on a patient in Ahmedabad while he was in Delhi.
- SSI Mantra: The use of the indigenous SSI Mantra robot, which is CDSCO-approved for tele-surgery, was highlighted as India leading the world in this field.
- Technical Needs: Successful tele-surgery requires a latency of less than 200 milliseconds to ensure the surgeon does not feel a lag.
Session 7: ISRO’s Continuing Medical Education (CME)
- Educational Outreach: ISRO has conducted 109 CME sessions since 2012, reaching over 20,000 healthcare professionals, particularly those in remote defense outposts like the Siachen Glacier.
- Space Medicine: Future ISRO projects will focus on Space Medicine, researching how microgravity affects molecule binding for new drugs and crop cultivation for long-term space missions.
Session 8: Startups and Mobile Innovations
- Patient-Centric Shifts: The move from “hospital-centric” to “mobile-first” care was discussed, with mobile apps acting as the fulcrum for real-time monitoring.
- Innovative Prototypes:
- RespiGO: A portable capnography device for real-time CO2 monitoring.
- Locomotion: A wearable sensor for clinical gate analysis.
- D3S Healthcare: The “VR Skin Scan Light,” a portable red-light technology for early-stage breast cancer screening
- Locomotion: A wearable sensor for clinical gate analysis.
Strategic Vision and ISRO’s Legacy
The conference highlighted ISRO’s 25-year history in pioneering telemedicine, which began with connecting super-speciality hospitals to remote areas using satellite technology. A recent milestone is the MOU with Integrated Defence Services (IDS) to provide medical services to strategic forces and their families in remote regions. Future technological frontiers include “Satcom on the Move” (mobile telemedicine nodes) to reach multiple villages and Quantum Key Distribution (QKD) to secure medical and financial data.
Implementation and the Digital Backbone
The shift from “hospital-centric” to “mobile-first” care was a central theme, with mobile apps acting as the primary point for real-time patient monitoring. The Ayushman Bharat Digital Mission (ABDM) is building the national digital infrastructure through several key components:
ABHA (Ayushman Bharat Health Account): Enables paperless, consent-based sharing of longitudinal health records.
Registries (HPR/HFR): Doctors and facilities must register on the Healthcare Professional Registry and Health Facility Registry to integrate into the national ecosystem.
- Incentives: The Digital Health Incentive Scheme (DHIS) offers hospitals financial rewards (up to ₹5 crore) for linking digital health records.
Legal Framework and Professional Standards
The Telemedicine Practice Guidelines (TPG) 2020 remain the essential legal framework, validated under the NMC Act 2019.
Consultation Standards: Guidelines define “First Consult” versus “Follow-up Consult” and strictly categorise drugs (Lists O, A, B, and Prohibited) for remote prescription.
Record Preservation: Records must be maintained for 3 years, or 10 years for medico-legal cases.
- Professionalism: Panelists emphasized “website manners,” such as maintaining eye contact with the camera to preserve patient empathy during video calls.
Data Privacy and Cyber Security
With the rise of digital health, security has become paramount, guided by the CIA Triad (Confidentiality, Integrity, and Availability).
Ransomware: Healthcare is a major target, as seen in the KD Hospital case study; hackers often use extortion by threatening to release data on the dark web.
Shadow AI: A critical warning was issued regarding the unauthorized use of public AI tools (like ChatGPT) with sensitive patient data, which can lead to severe privacy breaches and massive legal fines under the DPDP Act.
IoT Vulnerabilities: Medical devices like infusion pumps are increasingly susceptible to attacks, requiring regular security audits and avoiding public Wi-Fi.
Technological Frontiers: Tele-Robotics and Space Medicine
India is leading the world in tele-robotic surgery using the indigenous, CDSCO-approved SSI Mantra robot.
Milestone Surgery: The first tele-robotic surgery in Gujarat was performed on a patient in Ahmedabad by a surgeon located in Delhi.
Technical Requirements: Successful tele-surgery requires a latency of less than 200 milliseconds to prevent lag during procedures.
- Space Medicine: ISRO is researching how microgravity affects molecule binding for new drugs and crop cultivation for long-term space missions.
Innovation and Startups
GUSEC is actively incubating med-tech startups to address rural healthcare gaps. Featured prototypes include:
RespiGO: A portable capnography device for CO2 monitoring.
Locomotion: A wearable sensor for clinical gate analysis.
- D3S Healthcare: The “VR Skin Scan Light” for early-stage breast cancer screening.


Telemedicine Society of India Webinar Report
Celebrating Women, Advancing Health, Transforming Care
Commemorating International Women’s Day & World Kidney Day | 12th March 2026
Compiled by Ms. Neeraj Chaudhary
Introduction
The Telemedicine Society of India proudly hosted a special webinar commemorating International Women’s Day and World Kidney Day on 12th March 2026 a powerful convergence two important day celebrated across the globe.
This unique platform brought together distinguished women leaders from healthcare, public service, academia, and digital health to share insights, experiences, and innovations shaping the future of care. The discussions highlighted the intersection of gender, technology, and health equity, emphasizing how telemedicine is not only expanding access but also empowering women as both providers and beneficiaries of healthcare. The webinar stood as a testament to the growing leadership of women in shaping a more inclusive, accessible, and technology-enabled healthcare ecosystem.
Telehealth as a Tool for Women’s Empowerment
Dr. Uma Nambiar beautifully described telehealth as a “silent transformation”-one that is steadily changing women’s lives without always being visible. She spoke about how, despite growing conversations around gender equality, there is still a long way to go in achieving real, everyday equity.
Telemedicine, she explained, is helping bridge that gap. For women doctors, it offers the safety and comfort of consulting from home, reducing the stress of travel and long working hours. For many women who had to pause their careers due to family responsibilities, it opens a door to return, rebuild, and rediscover their professional identity.
For women as patients, the impact is equally powerful. In many homes, women’s health often takes a backseat. Teleconsultations allow them to seek care privately, conveniently, and without depending on others. Dr. Nambiar also highlighted how more women are stepping into leadership roles in digital health, driven by empathy and a strong sense of community.
Her message was simple yet powerful-telemedicine is not just technology; it is a quiet force for social change.
Session on Chronic Kidney Disease
In a very insightful session, Dr. Haritha Karuparti spoke about how digital health is improving the way we understand and manage Chronic Kidney Disease and Acute Kidney Injury.
She explained the vital role our kidneys play in maintaining balance in the body—from managing fluids to regulating blood pressure—and how early detection can make a life-saving difference. With tools like Electronic Medical Records, doctors can now identify risks earlier and act faster.
She also pointed out the importance of being cautious with commonly used medications like Nonsteroidal anti-inflammatory drugs, which can sometimes harm kidney function if not monitored properly. Technology, through smart alerts and monitoring systems, is helping doctors stay one step ahead.
What stood out in her talk was the emphasis on awareness—because informed patients and proactive care can truly change outcomes.
Leadership, Safety, and Women Empowerment
Dr. Anshu Singla delivered a deeply motivating talk that resonated far beyond the field of healthcare. Drawing from her journey as both a doctor and an IPS officer, she shared simple yet powerful life principles that can guide anyone.
She spoke about the importance of financial independence-not just as a goal, but as a foundation for confidence and freedom. She encouraged regular self-reflection, building meaningful relationships, and stepping out into the world to gain new perspectives through travel and exposure.
Her thoughts on setting personal boundaries, managing digital well-being, and taking care of physical health were especially relevant in today’s fast-paced world. Above all, she reminded everyone that giving back to society-no matter how small the act-adds meaning to our lives.
Her message was inspiring and clear: when women are empowered, communities become stronger and safer.
Telemedicine in Pediatric Liver Care
In a session that touched both the mind and the heart, Dr. Arti Pawaria spoke about caring for children with chronic liver diseases and the role telemedicine plays in supporting families through this journey.
She highlighted how managing such conditions is not a one-time effort but a long-term commitment involving multiple specialists. Telemedicine helps make this journey easier by reducing the need for frequent travel and allowing families to stay connected with doctors from their homes.
She shared a powerful real-life example of a child diagnosed with Wilson’s disease in a remote area—where telemedicine helped connect the dots, arrange testing, and ensure timely treatment. Stories like these show how technology can truly save lives.
Her message was deeply human—telemedicine is not just about convenience; it is about supporting families, reducing stress, and giving children a better chance at life.
Community Support and Breast Cancer Rehabilitation
Bringing a beautiful perspective on compassion in action, Ms. Srividya Gopinath from the Saisha India Foundation shared how small acts of kindness can make a big difference.
She spoke about supporting women recovering from Breast Cancer, especially those who have undergone Mastectomy, by providing handmade knitted prostheses. These are not just medical aids—they restore dignity, confidence, and comfort.
The initiative also extends to children undergoing chemotherapy and even premature babies in neonatal care, reflecting a deep commitment to care across all stages of life. With volunteers across the world, the movement continues to grow.
She also highlighted how telemedicine can help such initiatives reach more people, connect communities, and spread awareness.
“Give to Gain”: Compassion and Telemedicine
Gp. Capt. (Dr.) Suchitra Mankar brought in a powerful reflection on the idea of “Give to Gain.” Through her experiences in the Armed Forces Medical Services, she showed how selfless service can create lasting impact.
She spoke about the early days of telemedicine, when it was met with doubt and uncertainty. Despite this, she continued to believe in its potential and worked to bring healthcare to rural communities. Today, her efforts have helped bring medical care to villages that once had limited access.
Her journey is a reminder that meaningful change often begins with belief, persistence, and a willingness to serve.
Valedictory Remarks and Conclusion
Maj. (Dr.) Ashlesha Tawde Kelkar summarized the webinar as a powerful demonstration of leadership, compassion, innovation, and service by women in healthcare. She appreciated the Telemedicine Society of India for creating a platform that celebrates women’s contributions while addressing critical healthcare challenges.
Dr. Umashankar S expressed gratitude to all speakers and participants and reaffirmed the organization’s commitment to continuing such knowledge-sharing initiatives to promote telemedicine adoption across the country.
The webinar successfully highlighted how telemedicine, community participation, and women’s leadership are collectively transforming healthcare delivery in India. It demonstrated that when technology is combined with empathy and outreach, it can significantly enhance accessibility, affordability, and quality of healthcare services. The event concluded with a renewed commitment to advancing telemedicine-enabled care models and ensuring equitable healthcare reaches every corner of the nation.
Note: We acknowledge the use AI notes while documenting during the webinar.


A position Paper on reimaging Telehealth care services in India
– Telemedicine services in India are poised for a rebirth-
L.S.Satyamurthy
Former Director ISRO and Past President TSI
Background
Two decades of Telemedicine movement in India faced a Roller Coaster journey with the challenges of Technology evolution, demonstration, and standardization by Government of India and executed through Indian space research organization (ISRO) and Department of information technology(DITY) with the support of dedicated Doctors, State Health administrator’s, para medics, District and Specialty hospitals and the patient community at large.,
The fast developments and later retardation in Telehealth service are the hallmarks of implementation process in any country because of the inherent mind set/ orthodoxy among some stake holders compounded by technology obsolescence, connectivity issues, ambiguous Business/revenue models and uncertain regulatory framework.
Though the growth of several Telemedicine centers all over India was overwhelming with major Specialty Hospitals providing Tele-consultation and treatment to various rural remote district//Taluka hospitals/primary care centers in many States. This showed the potential thrust of Telehealth during the first decade of telemedicine (TM1.0) and during the second decade during Covid implementation in India (TM2.0) but later the effort is lukewarm in spite of the efforts by TSI and many institutions to promote Telemedicine.
Issues to be noted
As compared to first two decades (2001-2020) Telemedicine implementation, the technology of TM platform has undergone a metamorphic change from Desktop to Laptop to Mobile phone with software Cloud, customized/optimized EMR and multiparticipant Video conference systems.
On the connectivity side, the free Satellite connectivity provided by ISRO was withdrawn from many State centers in 2012 to enable them to use lower cost broadband/ wireless connectivity available in market
Today Telemedicine equipment industries/startups are bleeding and do not have major market share because of fewer customer base. All the Govt hospitals are dependent only “e Sajeevani“ platform provided by GOI free or very subsidized cost while it was envisaged that the major market for Telemedicine would be from the State Govt’s District, Taluk and primary health (PHCs) centers apart from private rural/urban clinics across India.
While the Telemedicine technology and service originated from the real necessity of providing Specialty care to the rural /Semi rural and semi urban areas who are deprived of such facility all along, telemedicine service in India is in dire straits without a proper direction and it is only more of research, academic and development activity of some dedicated specialty hospitals and medical institutions in spite of major references made by Hon’ble Prime Minister all along.
Artificial Intelligence is making big inroads in Health care services and more so for Telemedicine service.
The National TM task force formed in 2005 announced the formation of National Telemedicine grid which outcome remains as dream till today.
During Telemedicon conference at Amaravathi AP, the Niti Ayog representative took active participation and agreed to support the development of TM in the country and yet no tangible outcome.
Regarding Armed Forces TM network jointly setup by ISRO and AFMS over 100 centers, it was informed during Telemedicon2025 at Bangalore that they have taken up the Repurpose exercise to use TM network for post operative Medical Follow up services only in future.
What action is required now with TM 3.0
For Government hospitals networks all over the country:
All State governments should establish a Telemedicine Directorate under the guidelines from Minitry of Health GOI, for forming a Separate entity under the State’s Commissioner of H & FW and establish/ revive all the Telemedicine centers all over the state in District/Taluk hospital and PHCs and they should be connected to Specialty hospital Telemedicine centers Hub in few major towns/cities (like NSEW zone) within the state depending on size of state.
A few Senior Doctors/Specialist should be posted to the Specialist Govt Telemedicine centers Hub or with arranged Private hospitals TM Hubs for providing service as per established procedure and regulatory regime.
The funding approved under Unio budget needs to come from Ministry Health GOI to be distributed to states on selective first cum first serve basis.
A detailed plan and proposal to be worked out by a revised National Task force
For private Hospital networks they can follow their exiting setup and methodology as per TM guidelines
Conclusion and Recommendation
Establishment of Telemedicine Directorate in each state under the Commissioner of Health & Family Wellness department to take Telemedicine to the next level using any competitive platform for TM 3.0 for Indian health care system.
Let us put our effort in this Direction when our TM Margha Darshak’s and TSI experts are still active and ready to plunge in. Bravo India-Telemedicine-TSI.

A Pilgrimage Telemedicine Initiatives
Dr. Sreekumar C,
Professor of General Surgery and Telemedicine Medical Officer
Mr. Rajeesh M. V
Department of Amrita ISRO Telemedicine/Project
(Telemedicine System Administrator)
A Medical Camp was conducted at Kadampuzha Sri Bhagavathy Temple:
The Kadampuzha Devi temple is revered among worshippers as one of the most powerful shrines dedicated to Goddess Parvati. Located at Kadampuzha, 16km from Tirur, Malappuram, Kerala. Goddess Parvathi is worshipped here in the Kiratha rupa (in the form of a forest hunter). The temple dates back to more than 1900 years and is unique in that it does not have an idol.
The Medical Camp was conducted on 7th December 2025 in connection with Thrikarthika Festival. About 7000-9000 Pilgrims attended the Festival.
The camp was held in association with Malabar Devaswom board, Amrita Institute of Medical Sciences, Kochi, Amrita Telemedicine Unit, and the Telemedicine Society of India, Kerala Chapter.
The camp was inaugurated by Dr. Jaggu Swami (Hospital Administrator Amrita Hospital), Swamini Athulyamrita Praana (MA Math , Thirur ) delivered the benedictory address. Dr. D. M. Vasudevan (Dean – Research and Head of Telemedicine Amrita) was the Chief Guest. Dr. Sreekumar C, (Professor of General Surgery and Telemedicine Medical Officer) explained the details of the medical camp .The event was graced by PC Biju (Commissioner ,Malabar Devaswom Board), Pramod Kumar ( Assistant Commissioner, Malabar DB ), Renjan S ( Executive Officer, Kadampuzha Devaswom ), Dr Arun Vivek (Utilization Review Medical Officer, ASM -Hospital Administration ) Dr KV Sanjeevan (HOD Urology AIMS), Dr. Zachariah Paul (Nephrologist AIMS), and Dr Siva Kumar AIMS.
Experts from various Departments including General Medicine, General Surgery, Paediatric Surgery, Gastro Medicine, ENT, OBG, Orthopaedics, Ophthalmology, and Dentistry attended the camp. In addition to the free consultation, medicines were distributed to the patients free of cost. Blood investigations, ECG, X-ray, PFT, Fibro Scan and ECHO were done for the patients. The patient registration and flow system was set up by the MHA Students, Academy of Hospital administration, Headed by Dr Dinesh Nair. Mr. Rajeesh M. V, (Telemedicine System Administrator) enabled telemedicine facilities. Telemedicine consultation was done for 32 patients and the tele faculties include Dr. Akhilesh K (Professor, Department of Respiratory Medicine), Dr. Hareesh M. D Cardiology, Dr. Siby Gopinath (Epilepsy), and Dr. Ageesh M. D, Dr Muraleekrishnan DM( Gastroentrology ) Dr Beena Bahuleyan Addl Professor OBG. A total of 1200 patients were evaluated and treated. MBBS Students, Dental Students, dietitians, psychological counsellors, Pharmacist and other paramedical staff from AIMS Kochi also participated in this camp.




::ANNOUNCEMENTS::
“The Telemedicine Society of India (TSI) is deeply honoured to have been recognized as an ABDM Ambassador by the National Health Authority, Government of India. This recognition was conferred at the National Health Claims Exchange (NHCX) Innovation Meet organized at Indian Institute of Technology Hyderabad.
We accept this recognition with gratitude and humility, viewing it not as an achievement, but as a responsibility to further support the vision of the Ayushman Bharat Digital Mission (ABDM). TSI remains committed to contributing, in its own modest way, toward strengthening digital health adoption, capacity building, and collaborative efforts across the healthcare ecosystem.
We sincerely thank the National Health Authority for this encouragement and reaffirm our dedication to working alongside all stakeholders in advancing accessible, efficient, and patient-centric digital healthcare in India.”


::CROSSWORD::
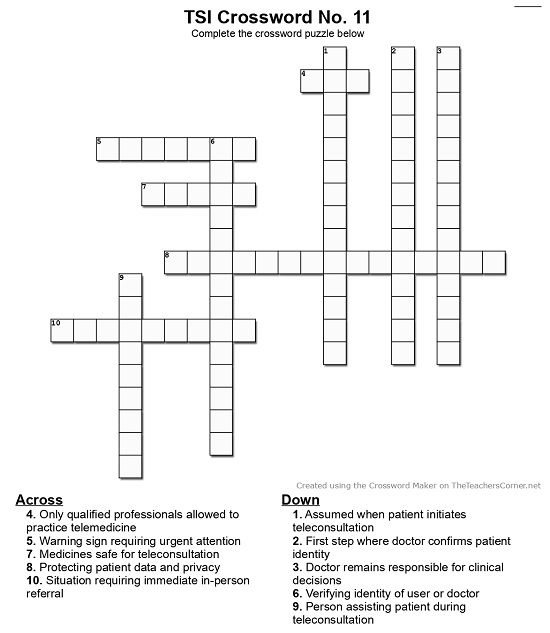
Click here to Print the Crossword
Click here to view the Crossword Rules and Regulations
Compiled by Dr.Umashankar
Answers in April 2026 Newsletter!
Telemedicine – News from India & Abroad
PULSE 2026: Maharashtra’s Blueprint for Affordable and Innovative Healthcare
Maharashtra’s PULSE 2026 aims to lead India in MedTech, better healthcare, and long-term economic growth…………….. Read More
Can Social Media Be Made Safer for Children Online?
As Indian states propose social media bans for minors, experts debate solutions like stricter age checks, safer algorithms and parental oversight………………… Read More
Telemedicine Practice Guidelines – A Foundation Course for RMPs by TSI Faculty
To know more about the Telemedicine Foundation Course click on the link below:
https://tsitn.org/tpg-course/
Medical Writing Certificate Course with Internship Opportunity!
TSI invites all the TSI Chapters and Members to submit information on their upcoming Webinar or Events (50 words), News related to Telemedicine (200 words) or short articles (500 words) for the monthly e-newsletter.Guidelines for submission to TSI Newsletter-
- Report can be from 500 to 600 words
- Report Should be relevant to Telemedicine or Medical Informatics
- No promotion of self or any product
- Avoid plagiarism
- All references should be included
- Provide any attributions
- Visuals are welcome including video links
- Send full authors name, degrees, affiliations along with a passport sized photograph of good resolution. If multiple authors only main author photo to be sent.
Submission may be sent to – tsigrouptn@gmail.com
Editors reserve the rights for accepting and publishing any submitted material.
Editor in Chief – Dr. Sunil Shroff
Editors – Dr. Senthil Tamilarasan & Dr. Sheila John
Technical Partner- https://www.medindia.net
